
Extra articular synovial chondromatosis is a rare unusual cause of shoulder pain.
Dr. C Yashavantha Kumar, Department of Orthopaedic Surgery, Ramaiah Medical College and Hospital, Bengaluru, Karnataka, India. E-mail: kumyashwanth@gmail.com
Introduction: Synovial chondromatosis is a rare benign tumor involving the major joints. This condition results from metaplasia of synovium into chondrocytes leading to formation of multiple loose bodies. Extra articular glenohumeral joint synovial chondromatosis involving long head of biceps is very rare.
Case Report: A 38-year-old male presented with history of insidious onset, dull aching pain in right shoulder for 6 months. Clinicoradiological examination revealed calcific mass around the long head of biceps tendon. The calcific mass and loose bodies were removed en bloc. Histopathological examination concurred to be synovial chondromatosis.
Conclusion: We hereby report a rare case of long head biceps tendon synovial chondromatosis of shoulder which was successfully treated by combined arthroscopic and open method. The results of surgical excision are excellent.
Keywords: Long head biceps, synovial chondromatosis, metaplasia.
Synovial chondromatosis is a rare benign condition involving major joints where synovium undergoes metaplasia into chondrocytes [1]. This metaplasia leads to formation of intraarticular cartilaginous nodule and loose bodies [2]. It is commonly seen in middle age and 3 times more common in males than females. Although it is a rare and monoarticular, commonly involves knee, hip and elbow joints. To best of our knowledge very few cases of synovial chondromatosis involving shoulder have been reported in literature. We hereby report a unusual case of long head of biceps tendon synovial chondromatosis in a 38-year-old male treated successfully.
A 38-year-old male presented with history of insidious onset, dull aching pain in right shoulder for 6 months. He also had difficulty in carrying out activities of daily living and restriction of movements of same shoulder. He had no constitutional symptoms and rest pain. On examination diffuse swelling on anterior aspect of shoulder along the bicipital grove. Terminal restriction of both active and passive movements of shoulder. Speed test and Yargasson test were positive. The strength of rotator cuff muscles were normal. Plain radiographs of shoulder revealed calcific mass around the long head of biceps tendon. The glenohumeral joint seems to be free of calcification and loose bodies (Fig. 1 and 2).  Magnetic resonance imaging (MRI) confirmed chondroid calcification and loose bodies around long head of biceps tendon (Fig. 3 and 4).
Magnetic resonance imaging (MRI) confirmed chondroid calcification and loose bodies around long head of biceps tendon (Fig. 3 and 4).  Routine laboratory investigations were unremarkable and alkaline phosphatase levels were normal. Diagnostic arthroscopy revealed normal glenohumeral joint and loose bodies in the bicipital groove. Deltopectoral approach made and the long head of biceps exposed (Fig. 5). The calcific mass and loose bodies were removed en bloc. The synovium around the long head of biceps excised. Histopathological examination concurred to be synovial chondromatosis (Fig. 6). Postoperatively patient was put on shoulder immobilizer for 2 weeks and mobilized later. At 3 months post-surgery patient painless joint with complete Range of motion. At 2 year follow up there is no clinical or radiological evidence of recurrence (Fig. 7).
Routine laboratory investigations were unremarkable and alkaline phosphatase levels were normal. Diagnostic arthroscopy revealed normal glenohumeral joint and loose bodies in the bicipital groove. Deltopectoral approach made and the long head of biceps exposed (Fig. 5). The calcific mass and loose bodies were removed en bloc. The synovium around the long head of biceps excised. Histopathological examination concurred to be synovial chondromatosis (Fig. 6). Postoperatively patient was put on shoulder immobilizer for 2 weeks and mobilized later. At 3 months post-surgery patient painless joint with complete Range of motion. At 2 year follow up there is no clinical or radiological evidence of recurrence (Fig. 7).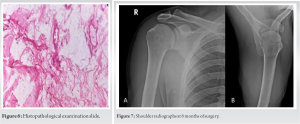
Synovial chondromatosis is a rare benign tumor. It is usually monoarticular involving large joints and knee joint is the most commonly involved joint. In pathogenesis synovium undergoes metaplasia into chondrocytes [3, 4]. This Metaplasia leads to formation of Intraarticular cartilaginous nodule and loose bodies. Two types of synovial chondromatosis have been described in literature, primary and secondary types. Etiology for secondary type of synovial chondromatosis are trauma, infection, degeneration or inflammatory arthritis [5, 6]. The exact etiology in primary type is not known. The clinical manifestations of disease are usually nonspecific and most commonly disease is self-limiting. Most common symptoms are pain, swelling and restriction of movements. Although natural history of disease is generally self-limiting, Davis et al. reported 5% relative risk of malignant transformation in primary synovial chondromatosis [7]. The standard radiographs usually demonstrate calcifications around the lesion and multiple loose bodies with various sizes are seen within the capsule [8]. MRI is usually preferred in cases where there is strong clinical suspicion and no calcification or loose bodies are seen on radiographs. The goal of surgical management of synovial chondromatosis is removal of loose bodies and synovium excision [9, 10]. The recurrence rates after successful surgery are 3–23%. Our patient underwent combined arthroscopic and open excision of the tumor. At 2 years of post-operative patient is free of symptoms and without recurrence.
In conclusion we hereby report a rare case of long head biceps tendon synovial chondromatosis of shoulder which was successfully treated by combined arthroscopic and open method. Synovial chondromatosis usually presents with nonspecific symptoms affecting large monoarticular joints. The results of surgical excision are excellent.
Synovial chondromatosis is a rare unusual cause of shoulder pain. Surgical excision has good clinical outcomes.
References
- 1.Ho YY, Choueka J. Synovial chondromatosis of the upper extremity. J Hand Surg Am 2013;38:804-10. [Google Scholar]
- 2.Adelani MA, Wupperman RM, Holt GE. Benign synovial disorders. J Am Acad Orthop Surg 2008;16:268-75. [Google Scholar]
- 3.Chen CY, Chen AC, Chang YH, Fu TS, Lee MS. Synovial chondromatosis of the hip: Management with arthroscope-assisted synovectomy and removal of loose bodies: Report of two cases. Chang Gung Med J 2003;26:208-14. [Google Scholar]
- 4.Shpitzer T, Ganel A, Engelberg S. Surgery for synovial chondromatosis. 26 cases followed up for 6 years. Acta Orthop Scand 1990;61:567-9. [Google Scholar]
- 5.Martinez R, Rubin AL. Synovial chondromatosis. Curr Sports Med Rep 2003,2:123-4. [Google Scholar]
- 6.Aydogan NH, Kocadal O, Ozmeric A, Aktekin CN. Arthroscopic treatment of concomitant subacromial and Subdeltoid synovial chondromatosis and labraum tear. Case Rep Orthop 2013;2013:636747. [Google Scholar]
- 7.Davis RI, Hamilton A, Biggart JD. Primary synovial chondromatosis: A clinicopathologic review and assessment of malignant potential. Hum Pathol 1998;29:683-8. [Google Scholar]
- 8.Wong K, Sallomi D, Janzen DL, Munk PL, O’Connell JX, Lee MJ. Monoarticular synovial lesions: Radiologic pictorial essay with pathologic illustration. Clin Radiol 1999;54:273-84. [Google Scholar]
- 9.Doral MN, Uzumcugil A, Bozkurt M, Atay OA, Cil A, Leblebicioglu G, et al. Arthroscopic treatment of synovial chondromatosis of the ankle. J Foot Ankle Surg 2007;46:192-5. [Google Scholar]
- 10.Moorthy V, Tay KS, Koo K. Arthroscopic treatment of primary synovial chondromatosis of the ankle: A case report and review of literature. J Orthop Case Rep 2020;10:54-9. [Google Scholar]






