
Femoral head autograft can be used to reconstruct the femoral calcar with good outcomes.
Dr. Valentin Antoci, Department of Orthopaedics Surgery, Warren Alpert Medical School of Brown University, University Orthopedics Inc., 1 Kettle Point Drive, East Providence, Rhode Island 02914. E-mail: valentin.antoci@gmail.com
Introduction: The calcar femorale helps manage compressive loads on the femoral head and is an essential component in determining intertrochanteric (IT) femur fracture stability. Fracture fixation can be complicated when primary fixation techniques, such as cephalomedullary nailing fail. Unstable IT femur fractures involving disruption of the medial calcar present additional fixation challenges.
Case Report: This case reports a patient with unstable IT fracture due to medial calcar disruption that experienced failure of a short cephalomedullary nail. Secondary fixation involved total hip arthroplasty (THA) with medical calcar reconstruction using femoral head autograft. Outcomes were good at 2-year follow-up with a full return to baseline activities.
Conclusion: The results indicate that femoral head autografting can be a viable option, with good outcomes, for medial calcar reconstruction in cases of failed IT fracture fixations without calcar support, converted to THA.
Keywords: Intertrochanteric fracture, femoral head autograft, calcar reconstruction.
The calcar femorale, or medial calcar, plays a critical role in managing the compressive loads on the femoral head and effectively redistributing such forces through the diaphysis. In addition, the medial calcar has been identified as essential in determining intertrochanteric (IT) fracture stability [1]. Recent trends have shown that IT fractures are most commonly managed with intramedullary nailing [2]. Previous in vitro studies have demonstrated that medial calcar comminution is associated with increased implant loading and early nail failure [3, 4, 5]. These findings translate clinically with several studies concluding that medial calcar disruption predicts lag screw cut out in certain intramedullary nailing constructs [6, 7]. Although arthroplasty is not typically the first-line treatment modality for IT fractures, it may be considered in patients with a history of hip arthritis, salvage of failed internal fixation, and osteoporotic bone that is unlikely to hold internal fixation. Evidence suggests that medial calcar integrity is similarly important in hip arthroplasty, with unstable medial calcar fractures leading to an increased risk of revision [8]. Reconstructive options for unstable IT femur fractures after failed primary fixation remain challenging as patients already have poor bone stock and thus surgical options are limited. Depending on fracture morphology and the status of the acetabulum, these cases may be treated with revision nailing, proximal femoral plating, or arthroplasty [9]. When arthroplasty is the chosen technique, surgeons may opt to reconstruct medial support with the use of a calcar-replacing prosthesis to ensure safe immediate weight bearing and reduce femoral component fixation failure, particularly in patients with marked osteoporosis [10]. Alternatively, it is possible to surgically reconstruct the lesser trochanter to provide an alternative form of medial stability without the need for more specialized prostheses. There is no current consensus as to the optimal management of medial calcar disruption in IT fractures that have failed fixation with cephalomedullary nailing (CMN). We report a case of failed nailing for an unstable IT femur fracture, treated subsequently with total hip arthroplasty (THA) with femoral head autografting to recreate the lesser trochanter.
An 80-year-old male with a recent history of a right IT femur fracture treated with short CMN 20 days prior presented to the emergency department with right hip pain. The pain began 2 days prior after twisting his right hip during a physical therapy session and gradually progressed to an inability to bear weight on the right lower extremity. The patient’s medical history was significant for coronary artery disease, atrial fibrillation for which he was on anticoagulation, cirrhosis, and hypertension. Before his hip fracture, he lived independently and volunteered at his local fire department. Physical examination revealed well-healed surgical scars on the right lateral hip and thigh, a shortened right lower extremity, and pain with passive range of motion in all planes. His neurovascular examination was normal. Inflammatory laboratory results were significant for an erythrocyte sedimentation rate of 72 mm/h, and C-reactive protein of 118 mg/L, and a white blood cell count of 6.8 × 109/L. Plain radiographs demonstrated a right IT femur fracture status post-CMN with a superior cut out of the cephalomedullary screw from the femoral head with erosion into the right acetabulum (Fig. 1). 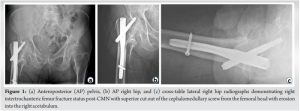
After internal medicine consultation and pre-operative risk assessment, the patient was consented for removal of hardware and right THA.
Surgical procedure
A standard posterior approach was utilized for the procedure. The cephalomedullary nail was removed with minimal bone loss. Following nail removal, the hip was dislocated, and the femoral neck was recut with an oscillating saw and an osteotome. The femoral head was removed and reserved. The acetabulum, femur, and the femoral canal were then prepared to accept THA cup and stem. A DePuy summit femoral stem was then placed into the prepared canal and gently impacted until it was almost fully seated. There was no visible medial cortex of the proximal femur. An attempt was made to retrieve the lesser trochanter, but it was not possible to mobilize safely. Thus, a new calcar was fashioned manually from the previously removed femoral head using an oscillating saw. This graft is useful as it preserves the remaining bone stock of the patient and provides native bone that should allow for some healing and integration resulting in better stability. The graft harvest technique was similar to that reported by Thakkar et al. 2015 [11]. The newly fashioned calcar replacement was secured in place with a proximal and distal cerclage wire (Fig. 2) with the new calcar secured the implant was then fully impacted. The femoral head was impacted onto the taper, the prosthesis was located and we were pleased with the stability and leg length. Following closure, the patient was transferred to the recovery room in stable condition. The patient tolerated the procedure without perioperative complications. Immediate post-operative radiographs demonstrated well seated and located right hip prosthesis with new calcar construction secured with cerclage wires and retained lesser trochanter fragment (Fig. 3).
Post-operative care
The patient was made weight-bearing as tolerated with a walker and instructed to avoid active abduction and to take anterolateral precautions. He was discharged on post-operative day 3 and was instructed to follow-up 3 weeks later for plain radiographs and a wound check. At the 3-week follow-up, radiographs demonstrated no interval changes in implant alignment (Fig. 4). 
He was managing pain adequately with Tylenol and reported a VAS score of 5. At 3 months postoperatively, he endorsed minimal hip pain and transitioned to outpatient physical therapy. One year postoperatively, radiographs demonstrated a right THA and cerclage wires in a stable and unchanged position, with complete healing of the femoral head to the calcar (Fig. 5). 
He had no acute complaints from his right hip at that time. At his 2-year follow-up, his radiographs were stable (Fig. 6)  and he was clinically doing well. Patient-reported outcomes were recorded at the 2-year follow-up, including SF-12 Physical Health score of 47.58, HOOS-Pain score of 72.50, HOOS – Sports and Recreational Activities score of 68.75, and HOOS, JR score of 67.52 (Table 1). He remains an independent ambulator and has returned to serving as a volunteer firefighter.
and he was clinically doing well. Patient-reported outcomes were recorded at the 2-year follow-up, including SF-12 Physical Health score of 47.58, HOOS-Pain score of 72.50, HOOS – Sports and Recreational Activities score of 68.75, and HOOS, JR score of 67.52 (Table 1). He remains an independent ambulator and has returned to serving as a volunteer firefighter.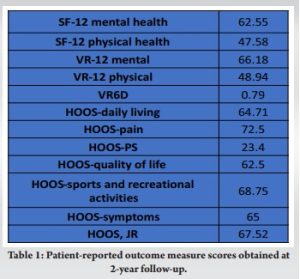
The current case reports a technique of utilizing femoral head autograft as a source for calcar restoration in the case of a failed CMN for an unstable IT femur fracture treated with THA. Several techniques for reconstructing the medial calcar have been described in the literature and typically involve either bone graft augmentation or the use of a calcar-replacing prosthetic femoral stem. In a case series of patients undergoing hemiarthroplasty for unstable IT fracture, Thakkar et al. found that 94% of patients with calcar femorale autografting achieved a satisfactory clinical outcome and graft healing [11]. In a case of multiple bilateral revisions THA for aseptic loosening and periprosthetic joint infection, Iwase et al. found viable bone regeneration between bone cement and metal wire mesh 4 years after impaction bone grafting for femoral calcar reconstruction. The calcar was sampled at the second revision of THA surgery and histological specimens demonstrated cortical and trabecular bone formation indicating active remodeling [12]. While we believe that medial calcar restoration is essential when using certain implants, it is important to note that it is possible to achieve acceptable clinical outcomes without reconstruction of the medial calcar. Zha et al. found satisfactory mid-term radiographic and clinical outcomes with cementless distal fixation modular prostheses without reconstruction of the medial calcar in their cohort of elderly patients with unstable IT fractures [13]. These results may not apply to more standard femoral stems, as distal fixation stems may be better suited to achieve stable fixation in cases of medial calcar disruption. Durgut et al. compared proximal femoral nail anti-rotation to cemented calcar-replacing hemiarthroplasty in a total of 94 patients and found both techniques equal in complications and outcomes and were seen as viable options for unstable IT fracture [14]. This case report demonstrates objectively good outcomes following conversion hip arthroplasty with femoral calcar reconstruction with femoral head autograft. Failure of femoral nailing does occur and having a technique to provide additional support in the case of conversion total arthroplasty is important information. This case provides evidence that calcar reconstruction with femoral head autograft results in good outcomes for patients. Surgeons in similar situations may utilize a similar strategy to achieve good outcomes for their patients. Further investigation will be necessary to determine if reconstruction of the medial calcar is necessary in all patients, and whether bone grafting or specialized calcar-replacing implants leads to superior post-operative outcomes.
While various techniques for medial calcar reconstruction have been described, this report is the first that focuses on the use of femoral head autografting to recreate the lesser trochanter for medial calcar restoration when performing conversion THA following the failure of intramedullary nailing. The patient in this case achieved satisfactory radiographic and clinical outcomes without signs of implant loosening or failure at the 2-year post-operative mark.
Femoral head autografting for medial calcar reconstruction in conversion hip arthroplasty following failed IT fracture fixation with CMN resulted in satisfactory radiographic and clinical outcomes.
References
- 1.Tarrant SM, Graan D, Tarrant DJ, Kim RG, Balogh ZJ. Medial calcar comminution and intramedullary nail failure in unstable geriatric trochanteric hip fractures. Medicina (Kaunas) 2021;57:338. [Google Scholar]
- 2.erner BC, Fashandi AH, Gwathmey FW, Yarboro SR. Trends in the management of intertrochanteric femur fractures in the United States 2005-2011. Hip Int 2015;25:270-6. [Google Scholar]
- 3.Do JH, Kim YS, Lee SJ, Jo ML, Han SK. Influence of fragment volume on stability of 3-part intertrochanteric fracture of the femur: A biomechanical study. Eur J Orthop Surg Traumatol 2013;23:371-7. [Google Scholar]
- 4.Marmor M, Liddle K, Pekmezci M, Buckley J, Matityahu A. The effect of fracture pattern stability on implant loading in OTA Type 31-A2 proximal femur fractures. J Orthop Trauma 2013;27:683-9. [Google Scholar]
- 5.Eberle S, Bauer C, Gerber C, von Oldenburg G, Augat P. The stability of a hip fracture determines the fatigue of an intramedullary nail. Proc Inst Mech Eng H 2010;224:577-84. [Google Scholar]
- 6.Parry JA, Sapp T, Langford JR, Koval KJ, Haidukewych GJ. Variables associated with lag screw sliding after single-screw cephalomedullary nail fixation of intertrochanteric fractures. J Orthop Trauma 2020;34:356-8. [Google Scholar]
- 7.Ciufo DJ, Zaruta DA, Lipof JS, Judd KT, Gorczyca JT, Ketz JP. Risk factors associated with cephalomedullary nail cutout in the treatment of trochanteric hip fractures. J Orthop Trauma 2017;31:583-8. [Google Scholar]
- 8.Miettinen SS, Mäkinen TJ, Kostensalo I, Mäkelä K, Huhtala H, Kettunen JS, et al. Risk factors for intraoperative calcar fracture in cementless total hip arthroplasty. Acta Orthop 2016;87:113-9. [Google Scholar]
- 9.Jethanandani RG, Nwankwo C, Wolinsky PR, Giordani M, Amanatullah DF. Proximal femoral reconstruction for failed internal fixation of a bisphosphonate-related femur fracture. Arthroplast Today 2016;2:153-6. [Google Scholar]
- 10.Celiktas M, Togrul E, Kose O. Calcar preservation arthroplasty for unstable intertrochanteric femoral fractures in elderly. Clin Orthop Surg 2015;7:436-42. [Google Scholar]
- 11.Thakkar CJ, Thakkar S, Kathalgere RT, Kumar MN. Calcar femorale grafting in the hemiarthroplasty of the hip for unstable inter trochanteric fractures. Indian J Orthop 2015;49:602-9. [Google Scholar]
- 12.Iwase T, Kouyama A, Matsushita N. Complete bone remodeling after calcar reconstruction with metal wire mesh and impaction bone grafting: A case report. Nagoya J Med Sci 2013;75:287-93. [Google Scholar]
- 13.Zha GC, Liu J, Wang Y, Feng S. Cementless distal fixation modular stem without reconstruction of femoral calcar for unstable intertrochanteric fracture in patients aged 75 years or more. Orthop Traumatol Surg Res 2019;105:35-9. [Google Scholar]
- 14.Durgut F, Şahin E, Çiftçi S, Kerem BA. Proximal femoral nail antirotation versus cemented calcar-replacement hemiarthroplasty for unstable intertrochanteric fracture in elderly: An overall survival study. Turk J Med Sci 2022;52:463-6. [Google Scholar]







