
Bifocal periprosthetic fractures above and below knee with total knee prosthesis can be treated with spanning Ilizarov external fixator.
Dr. Ruta Jakusonoka, Department of Orthopaedics, Riga Stradins University, Riga, Latvia. E-mail: ruta.jakusonoka@rsu.lv
Introduction: Multiple treatment options and internal and external devices have been recommended for periprosthetic fractures management around total knee arthroplasty.
Case Report: We present the case of the high-energy bifocal periprosthetic fractures of the femur and the tibia after total knee prosthesis following excision of a tumor. One of the fractures was an open tibial fracture Gustilo Type IIIB and the other – comminuted subtrochanteric fracture of the femur with extrusion of periprosthetic cement pieces out from the bone defect. The Ilizarov circular external fixator was used for the skeletal stabilization and early functional treatment in this compound case.
Conclusion: The use of Ilizarov external fixator for patients with complex periprosthetic fractures, who present severe technical difficulties in bone stabilization, especially by concomitant severe soft-tissue damage after high-energy injuries, is a good surgical alternative.
Keywords: Periprosthetic fracture, total knee replacement, tumor prosthesis, open fracture, Ilizarov external fixator.
Periprosthetic femoral shaft fractures represent an increasingly common and potential devastating complication associated with total joint arthroplasty [1]. There is the likelihood of an increased incidence of the periprosthetic femoral fractures due to the increasing number of primary arthroplasties being performed on a more active, ageing population [2]. Management of these fractures remains a challenge due to variety of factors, including those related to the fracture location, the quality of the bone and fixation of the prosthesis. Complications of the treatment are not uncommon and include malunion, non-union, and high rates of late loosening of the femoral component [3]. Periprosthetic fractures of the tibia are less commonly encountered and received less attention than periprosthetic fractures of the patella and distal femur, but they often require simultaneous revision knee surgery due to the loose prosthesis, peculiarity of the fracture, and any associated bone deficiencies [4, 5, 6]. Multiple treatment options are available for periprosthetic fractures around total knee arthroplasty. Many internal and external devices have been recommended including locking plates with cables, proximal and distal monocortical and\or bicortical screws or femoral intramedullary locked nails [7, 8, 9, 10, 11, 12]. McLauchlan et al. analyzed results of operative treatment of 45 patients with periprosthetic femoral fractures [13]. The results of an operative protocol compared well with the results of conservative management and avoided the problems of long-term immobilization. For patients with fractures associated with loose stems, new long stems implants were used to avoid large exposure and resultant complications [14]. Merkel and Johnson used a Hoffmann external fixator for the treatment of supracondylar fractures of the femur with good clinical result [15]. Simon and Brinker reported about treatment of the patient with supracondylar femur fracture above a total knee replacement using an Ilizarov external fixator [16]. Most of the publications concluded that periprosthetic fractures result from relatively minor trauma (low-energy injuries), and there were only one-focal femoral or tibial fracture, without significant soft-tissue damage [17, 18]. We could not find any report concerning bifocal periprosthetic fractures of femur and tibia after total knee replacement, and after revision of tumor prosthesis and particularly by high-energy mechanism of injury. To the best of our knowledge, this is the first report case of a bifocal periprosthetic fractures after total knee replacement having a previous medical history of an osteosarcoma of the distal femur.
The patient is a 27-year-old male who had been admitted to the emergency room after a road traffic accident. He suffered from a severe pain in his right thigh and ankle. He had a previous medical history of an osteosarcoma of the right distal femur 5 years ago. A wide resection of the tumor had been performed followed by cemented total knee tumor prosthesis replacement. Six months later, he was operated due to a deep wound infection and a revision knee arthroplasty was done. Five years later, he was free from metastases, knee extension 0° and flexion 50°. On examination and imaging studies in the emergency room, a bifocal periprosthetic fractures around both femoral and tibial stems components were found. There were closed comminuted subtrochanteric fracture of femur adjusted at the tip of the prosthesis in the presence of extruded bone cement at the fracture site (Fig. 1a), and open Gustilo Type IIIB fracture of middle and distal third of the tibia and fibula with bone and soft-tissue loss (Fig. 1b). The high suspicion of prosthetic loosening was presented too. In the operating room under general anesthesia, massive irrigation and surgical debridement of open fracture of the right leg with reduction and spanning external fixation by Ilizarov frame were performed (Fig. 2a). Closed reduction of the subtrochanteric femoral fracture was achieved by expansion of the external hybrid Ilizarov frame to the hip (Fig. 2b). For fixation of proximal fragment, an external fixation arch with three threaded 6 mm half-pins (two of them inserted through femoral neck and one-through lesser trochanter) was used. The Ilizarov fixator of the tibia in combination with additional mid-femoral ring with small wires was used as a distal segment of the external fixation frame for stabilization of the femoral fracture. The temporary bridging of the knee joint was performed (Fig. 2c).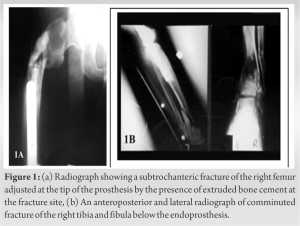 The healing of soft-tissue wound of the right leg occurred without any complications using method of negative pressure wound therapy followed by skin grafting. The physiotherapeutic treatment, which included muscle strength exercises, active and passive motions of the ankle joint, walking with partial weight bearing on right lower limb, was started on the 3rd post-operative day. Six weeks later, the patient walked with full weight bearing with two crutches. Eight months after operation, in the presence of radiological signs of bone consolidation, clinical test of full weight bearing on the right lower limb by unscrewing the nuts of the threaded rods of external fixation frame was performed – the walking remained painless. Thirty-eight weeks after surgery, the hybrid Ilizarov device was removed and support with long leg brace was continued for additional 3 months. There was no evidence of prosthetic loosening (Fig. 3a, b, c).
The healing of soft-tissue wound of the right leg occurred without any complications using method of negative pressure wound therapy followed by skin grafting. The physiotherapeutic treatment, which included muscle strength exercises, active and passive motions of the ankle joint, walking with partial weight bearing on right lower limb, was started on the 3rd post-operative day. Six weeks later, the patient walked with full weight bearing with two crutches. Eight months after operation, in the presence of radiological signs of bone consolidation, clinical test of full weight bearing on the right lower limb by unscrewing the nuts of the threaded rods of external fixation frame was performed – the walking remained painless. Thirty-eight weeks after surgery, the hybrid Ilizarov device was removed and support with long leg brace was continued for additional 3 months. There was no evidence of prosthetic loosening (Fig. 3a, b, c).  Five months later, the patient returned to his previous activities. By follow-up at 24 months, he had full knee extension 0° and flexion 40°, which corresponded to the ranges of pre-traumatic motions, and he walked without support.
Five months later, the patient returned to his previous activities. By follow-up at 24 months, he had full knee extension 0° and flexion 40°, which corresponded to the ranges of pre-traumatic motions, and he walked without support.
Total joint arthroplasty has become a common surgery in recent years; hence, periprosthetic fractures have become an increasingly important surgical challenge. These fractures usually occur in elderly patients with osteoporosis who has had total joint replacement of the hip or knee and not associated with soft-tissue trauma. Various solutions include conservative methods, internal fixation with plate and screws, intramedullary fixation; specially that designed revision prosthesis with long intramedullary stems has been reported. Because the medullar canal is occupied by the prosthesis, stable internal fixation becomes a major difficulty. Extruded cement should be removed [19]. The most publications concerning periprosthetic fractures are related to conditions, which are not associated with soft-tissue trauma [20, 21, 22]. We could not find either any report about principles of treatment by bifocal periprosthetic fractures of femur and tibia in patients after total knee arthroplasties. By treating the patient with bifocal periprosthetic fractures of femur and tibia (the proximal – with loosed bone cement, and distal – open Gustilo IIIB fracture with bone and soft-tissue loss), we performed bone stabilization with hybrid Ilizarov external fixation frame. The fixation of open high-energy tibial fracture was fulfilled after meticulous debridement by small wire Ilizarov device. For stabilization of subtrochanteric femoral fracture, adjacent to the prosthetic stem, the circular frame was extended until the hip with fixation of proximal fragment by transcervical half-pins. This allowed achieving the skeletal stabilization effective enough for early functional treatment and sufficient bone healing of both complicated high-energy fractures [23]. It is remarkable that subtrochanteric fracture was healed even in presence of relatively big cement piece; loosen out from the bone canal. The patient returned to his previous level of activity. Our case study has the limitation. Patient moved to another city and he was lost to follow-up after last visit.
We recommend the use of Ilizarov external fixator for patients with complex periprosthetic fractures, who present severe technical difficulties in bone stabilization, especially by concomitant severe soft-tissue damage after high-energy injuries.
Ilizarov external fixator for patients with complex periprosthetic fractures is a good surgical alternative for stable bone fixation and functional treating and can be used as a salvage solution in these difficult situations.
References
- 1.Benkovich V, Klassov Y, Mazilis B, Bloom S. Periprosthetic fractures of the knee: A comprehensive review. Eur J Orthop Surg Traumatol 2020;30:387-99. [Google Scholar]
- 2.Ruiz AL, Thompson NW, Brown JG. Periprosthetic femoral fractures in Northern Ireland. Ulster Med J 2000;69:118-22. [Google Scholar]
- 3.Konan S, Sandiford N, Unno F, Masri BS, Garbuz DS, Duncan CP. Periprosthetic fractures associated with total knee arthroplasty: An update. Bone Joint J 2016;98-B:1489-96. [Google Scholar]
- 4.Felix NA, Stuart MJ, Hanssen AD. Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin Orthop Relat Res 1997;345:113-24. [Google Scholar]
- 5.Hanssen AD, Stuart MJ. Treatment of periprosthetic tibial fractures. Clin Orthop Relat Res 2000;380:91-8. [Google Scholar]
- 6.Stuart MJ, Hanssen AD. Total knee arthroplasty: Periprosthetic tibial fractures. Orthop Clin North Am 1999;30:279-86. [Google Scholar]
- 7.Wallace SS, Bechtold D, Sassoon A. Periprosthetic fractures of the distal femur after total knee arthroplasty: Plate versus nail fixation. Orthop Traumatol Surg Res 2017;103:257-62. [Google Scholar]
- 8.Tadross TS, Nanu AM, Buchanan MJ, Checketts RG. Dall-Miles plating for periprosthetic B1 fractures of the femur. J Arthroplasty 2000;15:47-51. [Google Scholar]
- 9.Venu KM, Koka R, Garikipati R, Shenava Y, Madhu TS. Dall-Miles cable and plate fixation for the treatment of peri-prosthetic femoral fractures-analysis of results in 13 cases. Injury 2001;32:395-400. [Google Scholar]
- 10.Ochsner PE, Pfister A. Use of the fork plate for internal fixation of periprosthetic fractures and osteotomies in connection with total knee replacement. Orthopedics 1999;22:517-21. [Google Scholar]
- 11.De Ridder VA, De Lange S, Koomen AR, Heatley FW. Partridge ostheosyntesis: A prospective clinical study on the use of nylon cerclage bands and plates in the treatment of periprosthetic femoral shaft fractures. J Orthop Trauma 2001;1:61-5. [Google Scholar]
- 12.Dennis MG, Simon JA, Kummer FJ, Koval KJ, Di Cesare PE. Fixation of periprosthetic femoral shaft fractures: A biomechanical comparison of two techniques. J Orthop Trauma 2001;15:177-80. [Google Scholar]
- 13.McLauchlan GJ, Robinson CM, Singer BR, Christie J. Results of an operative policy in the treatment of periprosthetic femoral fracture. J Orthop Trauma 1997;11:170-9. [Google Scholar]
- 14.Cordeiro EN, Costa RC, Carazzato JG, Silva JS. Periprosthetic fractures in patients with total knee arthroplasties. Clin Orthop Relat Res 1990;252:182-9. [Google Scholar]
- 15.Merkel KD, Johnson EW Jr. Supracondylar fracture of the femur after total knee arthroplasty. J Bone Joint Surg Am 1986;68:29-43. [Google Scholar]
- 16.Simon RG, Brinker MR. Use of Ilizarov external fixation for a periprosthetic supracondylar femur fracture. J Arthroplasty 1999;14:118-21. [Google Scholar]
- 17.Nozaka K, Miyakoshi N, Hongo M, Kasukawa Y, Saito H, Kijima H, et al. Effectiveness of circular external fixator in periprosthetic fractures around the knee. BMC Musculoskelet Disord 2020;21:317. [Google Scholar]
- 18.Nozaka K, Miyakoshi N, Sato T, Shimada Y. Ilizarov external fixation for a periprosthetic tibial fracture in severe osteoporosis: A case report. BMC Musculoskelet Disord 2020;21:145. [Google Scholar]
- 19.Engh GA, Ammeen DJ. Periprosthetic fractures adjacent to total knee implants. J Bone and Joint Surg 1997;79A:1100-13. [Google Scholar]
- 20.Beris AE, Lykissas MG, Sioros V, Mavrodontidis AN, Korompilias AV. Femoral periprosthetic fracture in osteoporotic bone after a total knee replacement: Treatment with Ilizarov external fixation. J Arthroplasty 2010;25:1168.e9-12. [Google Scholar]
- 21.Refaat M, Coleman S, Meehan JP, Jamali AA. Periprosthetic supracondylar femur fracture treated with spanning external fixation. Am J Orthop (Belle Mead NJ) 2015;44:90-3. [Google Scholar]
- 22.Ebraheim NA, Kelley LH, Liu X, Thomas IS, Steiner RB, Liu J. Periprosthetic distal femur fracture after total knee arthroplasty: A systematic review. Orthop Surg 2015;7:297-305. [Google Scholar]
- 23.Lerner A, Jakusonoka R, Jumtins A, Rothem D. Temporary bridging trans-hip external fixation in damage control orthopaedics treatment after severe combat trauma: A clinical case series. Injury 2023;54:991-5. [Google Scholar]






