
Thus, our screw removal technique can help in implant removal in revision spine surgeries in peripheral centers or small cities where there are limited facilities in terms of instrumentation and availability of implants.
Dr. Pranav Gupta, Department of Orthopaedics, Guru Gobind Singh Medical College and Hospital, Faridkot - 151 203, Punjab, India. E-mail: pranavchd88@gmail.com
Introduction: As the number of patients undergoing spine fixation has increased, the requirement for revision surgery has also increased. Difficulty faced while doing revision surgery is mostly in removing polyaxial pedicle screws, especially if we do not have the desired instrumentation.
Case Report: A 55-year-old patient previously operated for D12 fracture presented to us with implant failure due to backing out of pedicle screws. Compatible instrumentation to remove the implant was not available as even the cap screw could not be removed due to screwdriver mismatch. Hence, we had to design our own method to address the problem which we did successfully. At present, the patient is on our regular follow-up, is pain free, is able to walk without support, and has not reported any new complaints.
Conclusion: Method used in our case simplifies and accelerates the screw removal process and provides guidance to any surgeon who faces a similar problem.
Keywords: Implant failure, jumbo cutter, pedicle screw.
Nowadays, more people are opting for spine surgery rather than bearing pain and taking medications. In the 1930s, the implant material was not that good due to which a large number of cases ended in implant failure [1]. After the 1940s, the implant material and implant techniques have gone through considerable changes due to which they can resist the continuous stress of weight-bearing, flexion, and extension until fusion occurs. The most common reason for implant failure is unsuccessful fusion [2]. There is a race between implant failure and union and if union does not occur, there are high chance that patient will land up in implant failure which can be in the form of hardware fracture, loosening of screws, and screw pullout [3]. Hardware loosening can be caused by osseous resorption surrounding screws and implants. Loosening in turn allows for movement which causes further osseous resorption, increased mobility, and eventually screw pullout or vertebral fracture [4, 5]. Diameter of cap screw head varies from one implant to another due to the lack of standardization of implants, especially in developing countries like India. Therefore, it is necessary to have the same instrumentation which was used in the previous surgery. This is not always possible as most of the time information about previous implant is not known and sometimes even if it is known may still not be available due to various reasons, like company no more working, or patient undergoing revision surgery in a city where that implant may not be available. Revision surgery always takes more time which in turn also leads to the risk of increased blood loss as well as infection. Innovative method used in our case simplifies and accelerates the polyaxial screw removal process; thus, shortening the operating time.
A 55-year-old female came to us on wheelchair with back pain radiating to bilateral lower limbs for 6 months and being able to walk few steps inside house only to attend her basic daily toilet routine. The patient was operated elsewhere for D12 fracture 6 months back in which pedicle screw fixation was done, 2 each in D11 and L1 vertebra. The patient only had pre-operative MRI (Fig. 1) when she came to us in OPD.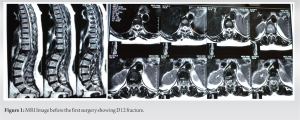 According to the patient, pain persisted even after the surgery. On examination, there was no sensory or motor deficit in lower limbs. In X-ray, it was seen that one pedicle screw in D11 vertebra had backed out and there was localized kyphosis at D12 vertebra (Fig. 2). The patient was planned for surgery. Instrumentation was not known. Hence, we had kept all possible instrumentation including Allen key. Removal of pedicle screw requires the removal of cap screw first followed by rod and pedicle screw. In our case, cap screw was of 4.5-mm size, however, size of screwdriver available was of 6.5 mm. We also tried locking screw driver which did not work.
According to the patient, pain persisted even after the surgery. On examination, there was no sensory or motor deficit in lower limbs. In X-ray, it was seen that one pedicle screw in D11 vertebra had backed out and there was localized kyphosis at D12 vertebra (Fig. 2). The patient was planned for surgery. Instrumentation was not known. Hence, we had kept all possible instrumentation including Allen key. Removal of pedicle screw requires the removal of cap screw first followed by rod and pedicle screw. In our case, cap screw was of 4.5-mm size, however, size of screwdriver available was of 6.5 mm. We also tried locking screw driver which did not work. We then tried different 4.5-mm screwdrivers, but they were also not compatible with the cap screw head. Hence, we used jumbo cutter as a final modality to cut the rods close to the head of the screws (Fig. 3) due to which polyaxial screw along with small piece of rods on their head behaved like a single unit. These rods acted as levers with which pedicle screws were removed (Fig. 4).
We then tried different 4.5-mm screwdrivers, but they were also not compatible with the cap screw head. Hence, we used jumbo cutter as a final modality to cut the rods close to the head of the screws (Fig. 3) due to which polyaxial screw along with small piece of rods on their head behaved like a single unit. These rods acted as levers with which pedicle screws were removed (Fig. 4).  Following implant removal, 6.5-mm screws 2 each were inserted in D10, D11, L1, and L2 vertebra while a single pedicle screw was inserted in fractured D12 vertebra (Fig. 5). On post-operative day 3, the patient was allowed to walk with the support of walker. Patient’s general condition was fine and was pain free except for the operative site pain. The patient was started on antiosteoporotic treatment at the time of discharge. At present, i.e., 2 years after the revision surgery, the patient is pain free, is able to walk without support, and has not reported any new complaint.
Following implant removal, 6.5-mm screws 2 each were inserted in D10, D11, L1, and L2 vertebra while a single pedicle screw was inserted in fractured D12 vertebra (Fig. 5). On post-operative day 3, the patient was allowed to walk with the support of walker. Patient’s general condition was fine and was pain free except for the operative site pain. The patient was started on antiosteoporotic treatment at the time of discharge. At present, i.e., 2 years after the revision surgery, the patient is pain free, is able to walk without support, and has not reported any new complaint.
The most common procedure done in the spine is pedicle screw fixation [6]. Post-fixation, the most common reasons for a second surgery are implant breakage, loosening, and pseudoarthrosis [7]. Among the many types of implant failure, removal of broken screw is the most difficult. Even if screws are intact, their removal can become tough when patient’s medical records are not available, because of which instrumentation set to go toward cannot be marked out. Even if we have the instrument set of the concerned implant, screwdriver may not engage with the screw head because of a damaged cap screw head occurring in the last surgery. When literature was surveyed, they was barely any information related to removing intact screws and whatever information was there required proper instruments. In U-rod technique described by Kose et al., surgeon used Allen key to remove cap screws and the screw is placed in the U-shaped rod after removing the rods [8]. Uvaraj and Bosco in his study first removed cap screw followed by connecting rod and after cutting rod to 25-mm length reapplied it over polyaxial screw head converting it into single system and then removed pedicle screw using counter torque wrench and appropriate size screwdriver [9]. However, the above methods will work only if cap screw holding the rod with the screw can be removed. In our case, even the cap screw could not be removed due to screwdriver mismatch. Hence, we modified the technique in which we cut the rods near the pedicle screw head and then removed the screws. The same method has been mentioned by Ulus et al. using speed drill or circular saw [10]. However, in our case, we used a jumbo cutter to cut the rods which is easily available. Our screw remover design reduces the time and effort of surgery and also takes away the need to remove the fibrous tissue covering the cap screw heads and pedicle screw heads to engage the screwdriver.
Our screw removal technique which is useful and cost effective can help overcome the problem faced by surgeons during implant removal in revision surgeries working in peripheral centers or small cities where there are limited facilities in terms of instrumentation and availability of implants.
Our technique of removing pedicle screws reduces the time and effort of surgery and also takes away the need to remove the fibrous tissue covering the cap screw heads and pedicle screw heads to engage the screwdriver.
References
- 1.Gruber P, Boeni T. History of spinal disorders. In: Spinal Disorders. Germany: Springer; 2008. p. 3-41. [Google Scholar]
- 2.Gupta A, Das K, Bansal K, Chhabra HS, Arora M. Should implant breakage be always considered as implant “Failure” in spine surgery: Analysis of two cases and literature review. Cureus 2021;13:e15233. [Google Scholar]
- 3.Heller JG, Whitecloud TS 3rd, Butler JC, Abitbol JJ, Garfin SR, Wilkinson HA, et al. Complications of spinal surgery. In: Herkowitz HN, Garfin SR, Balderston RA editors. The Spine. Philadelphia, PA. B. Saunders Co.; 1992. p. 1817-98. [Google Scholar]
- 4.Kim PE, Zee CS. Imaging of the postoperative spine: Cages, prostheses and instrumentation. Spinal Imaging Med Radiol 2007;6:397-413. [Google Scholar]
- 5.Tehranzadeh J, Ton JD, Rosen CD. Advances in spinal fusion. Semin Ultrasound CT MR 2005;26:103-13. [Google Scholar]
- 6.Tian W, Liu YJ, Liu B, He D, Wu JY, Han XG, et al. Guideline for thoracolumbar pedicle screw placement assisted by orthopaedic surgical robot. Orthop Surg 2019;11:153-9. [Google Scholar]
- 7.Elmadag M, Guzel Y, Uzer G, Acar MA. An innovative universal screw removal instrument. Korean J Spine 2015;12:1-4. [Google Scholar]
- 8.Kose KC, Isik C, Altinel L, Ates A, Ozdemir M. Easy retrieval of polyaxial tulip-head pedicle screws by “U” rod technique. Eur Spine J 2009;19:144-6. [Google Scholar]
- 9.Uvaraj NR, Bosco A. A simple versatile technique to retrieve polyaxial tulip-head spinal pedicle screws following failed pedicle screw removal. A technical note with analysis of efficacy and outcomes. Tech Orthop 2021; Aprint of head. [Google Scholar]
- 10.Ulus A, Kaya AH, Bayri Y, Dagcinar A, Sataloglu H, Senel A. Poly-axial screw removal. Cent Eur Neurosurg 2010;71:108-9. [Google Scholar]






