
Mohs paste, containing zinc chloride, coagulates tissue and prevents intraoperative neoplastic bleeding, reducing tumor recurrence rate by the preoperative usage.
Dr. Akio Sakamoto, Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, 54 Shogoin, Kawahara-cho, Sakyo-ku, Kyoto 606-8507, Japan. E-mail: akiosaka@kuhp.kyoto-u.ac.jp
Abstract
Introduction: Mohs paste has a zinc chloride component and the ability to coagulate tissue. Mohs chemosurgery or surgery is a method by which coagulated tissue is removed and can be repeated until the tumor disappears. The palliative purpose of Mohs chemosurgery or surgery is to control bleeding or exudate from a malignancy with a skin ulcer. In the current report, a single application of Mohs paste as a pre-operative treatment for a superficial sarcoma with a skin ulcer prevented intra-operative bleeding.
Case Report: Two metastatic sarcomas are described: one in the scalp originating from a rectoperineal dedifferentiated liposarcoma and one in the elbow originating from a humeral telangiectatic osteosarcoma. Mohs paste treatment was performed the day before surgical resection. The Mohs paste procedure successfully prevented intra-operative bleeding from the tumor, leading to easy removal of the tumors with appropriate tumor-free margins.
Conclusion: Preoperative Mohs paste treatment is a simple and reliable method. Intra-operative neoplastic bleeding may contaminate the tumor cells within the surgical field; thus the prevention of bleeding with Mohs paste treatment may lead to a decrease in the tumor recurrence rate.
Keywords: Mohs surgery, metastasis, sarcomas, skin ulcer, preoperative.
Mohs paste treatment is known as Mohs chemosurgery, as first described by Mohs in the 1930s [1,2]. The main component of Mohs paste is zinc chloride, which has an ability to coagulate tissue. Mohs chemosurgery is a method with curative intent, in which the repeated resection of coagulated tissue by Mohs paste is performed until the tumor disappears. The method is widely applied in patients with skin cancer [3,4,5]. In contrast, the palliative purpose of Mohs paste treatment is to stop bleeding or exudate from skin and breast cancer ulcers to improve the quality of life [6,7]. Mohs paste treatment is used mainly for palliative purposes in superficial ulcerated lesions with bleeding, such as angiosarcomas [8]. Mohs paste treatment can be used as neoadjuvant therapy with curative intent. Mohs paste treatment has a role in pre-operative volume reduction in the treatment of pleomorphic sarcomas involving the chest wall [9]. In the current report, Mohs paste treatment was used to prevent intra-operative bleeding from a subcutaneous sarcoma with a skin ulcer.
Mohs paste consists of zinc chloride (50 g), zinc oxide starch (25 g), and purified water (25 mL) in our institute. Glycerin is used to adjust the viscosity. White petroleum is used to protect healthy skin around the ulcer. The paste is applied to the surface of the ulcer. When the ulcerated lesion is fragile, a small gauze soaked with Mohs paste is used. The duration of Mohs paste fixation is 30 min; then, the excessive paste is removed. The Mohs paste soaked gauze is not removed to avoid rebleeding. A 72-year-old woman was treated for a rectoperineal dedifferentiated liposarcoma over a 3-year-period. Multiple lung metastases and a subsequent resection were performed over a 2.5-year period. She noticed a tumor in the scalp with bleeding from the tumor. On physical examination, a protuberant, immobile elastic mass appeared to be attached to the fascia and was palpable on the scalp. Magnetic resonance imaging (MRI) revealed a 2-cm subcutaneous tumor. The tumor had a homogeneous low-signal intensity on the T1-weighted image and high-signal intensity on the T2-weighted image (Fig. 1a). Pre-operative Mohs paste treatment was performed (Fig. 1b). The tumor was resected with the surrounding skin and subcutaneous tissue, leaving a 5-cm defect in the maximum diameter (Fig. 1c).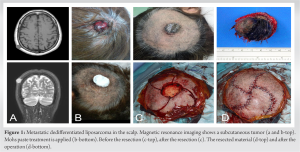 The defect was reconstructed with a flap (Fig. 1d). The resected material was a spindle cell sarcoma, compatible with a dedifferentiated component of dedifferentiated liposarcoma. After the resection, post-operative chemotherapy with doxorubicin was administered. 19 months later, which was 4 years 3 months after the initial treatment, the patient died of dyspnea due to spread of the lung lesions. No recurrence was noted at the scalp lesion. A 17-year-old man was treated for a telangiectatic osteosarcoma in the humerus over a 2-year period. Multiple drug chemotherapy regimens were administered. Multiple lung metastases occurred over the ensuing year. The soft-tissue metastasis to the elbow grew and a skin ulcer developed (Fig. 2a). In addition to multiple lung metastases, a 3-cm ulcerated mass in the elbow developed with bleeding. The surface of the tumor was fragile and bleeding. Computed tomography revealed a subcutaneous tumor (6 cm in diameter) invading the muscle (Fig. 2b). Mohs paste treatment was applied to the surface of the lesion. The tumor was fragile; thus small gauze soaked with Mohs paste was used. The duration of Mohs paste fixation was about 12 h (Fig. 2c). The tumor was resected with the surrounding skin, and a skin graft was transplanted (Fig. 2d and e). The resected material was a telangiectatic osteosarcoma. 3 months later die of the disease. 3 months later, which was 2 years 3 months after the initial treatment, the patient died of dyspnea due to spread of the lung lesions.
The defect was reconstructed with a flap (Fig. 1d). The resected material was a spindle cell sarcoma, compatible with a dedifferentiated component of dedifferentiated liposarcoma. After the resection, post-operative chemotherapy with doxorubicin was administered. 19 months later, which was 4 years 3 months after the initial treatment, the patient died of dyspnea due to spread of the lung lesions. No recurrence was noted at the scalp lesion. A 17-year-old man was treated for a telangiectatic osteosarcoma in the humerus over a 2-year period. Multiple drug chemotherapy regimens were administered. Multiple lung metastases occurred over the ensuing year. The soft-tissue metastasis to the elbow grew and a skin ulcer developed (Fig. 2a). In addition to multiple lung metastases, a 3-cm ulcerated mass in the elbow developed with bleeding. The surface of the tumor was fragile and bleeding. Computed tomography revealed a subcutaneous tumor (6 cm in diameter) invading the muscle (Fig. 2b). Mohs paste treatment was applied to the surface of the lesion. The tumor was fragile; thus small gauze soaked with Mohs paste was used. The duration of Mohs paste fixation was about 12 h (Fig. 2c). The tumor was resected with the surrounding skin, and a skin graft was transplanted (Fig. 2d and e). The resected material was a telangiectatic osteosarcoma. 3 months later die of the disease. 3 months later, which was 2 years 3 months after the initial treatment, the patient died of dyspnea due to spread of the lung lesions.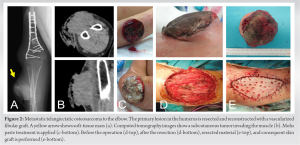
Subcutaneous sarcomas invade the overlaying skin, leading to ulcer formation. Malignant tumor tissue is fragile because of the neoplastic cells, necrotic tissue, and abnormal vessels. The ulcerated skin bleeds and produces an exudate. In the current report, Mohs paste treatment was used preoperatively for a subcutaneous sarcoma and a skin ulcer to prevent intraoperative bleeding. Zinc chloride is the main component in Mohs paste; the zinc ions have a role in tissue coagulation [7]. The extent of coagulation is correlated to the duration of Mohs paste application. It has been reported that the coagulation depth is up to 5 mm at 48 h and 10 mm at 72 using a 1-mm thick Mohs paste application [10]. Mohs paste is not systemically toxic [11]; however, Mohs paste should not be applied to healthy skin so that Mohs paste will not injure the skin. In our cases, white petroleum was used to protect healthy skin around the ulcer. Mohs paste was applied for 30 min in one case. In the other case, Mohs paste soaked in gauze was used and remained on the tumor surface 1 day before surgery. The duration of Mohs paste fixation was about 12 h. The application time of 12 h could have been extended to 24 h, when the tumor was large. Mohs paste treatment is used not only for local control of advanced cancers, such as skin or breast cancer, but also with curative intent in skin cancers [3,6,7]. Mohs paste treatment has become an option of multidisciplinary treatment in locally advanced cancers [12]. For soft-tissue sarcomas, Mohs paste treatment is used mainly for palliative purposes in superficial ulcerated lesions with bleeding, such as angiosarcomas [8]. In contrast, Mohs paste treatment can also be used for tumor volume reduction as neoadjuvant therapy for resection in superficial soft-tissue sarcomas [9,10,13]. The current method of pre-operative Mohs paste use is a simple and definitive method; the method serves as another treatment option.
In the current report, Mohs paste was used to stop bleeding intraoperatively. Mohs paste treatment is an effective and reliable treatment option for the prevention of bleeding intraoperatively. Intra-operative neoplastic bleeding may contaminate the tumor cells within the surgical field, and the prevention of bleeding with Mohs paste may lead to a decrease in the tumor recurrence rate.
Mohs paste has a zinc chloride component and the ability to coagulate tissue. Intra-operative neoplastic bleeding may contaminate the tumor cells within the surgical field; thus, the prevention of bleeding with Mohs paste treatment may lead to a decrease in the tumor recurrence rate.
References
- 1.Mohs FE. Chemosurgery. Clin Plast Surg 1980;7:349-60. [Google Scholar | PubMed]
- 2.Mosterd K, Krekels GA, Nieman FH, Ostertag JU, Essers BA, Dirksen CD, et al. Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: A prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol 2008;9:1149-56. [Google Scholar | PubMed]
- 3.Turner RJ, Leonard N, Malcolm AJ, Lawrence CM, Dahl MG. A retrospective study of outcome of Mohs’ micrographic surgery for cutaneous squamous cell carcinoma using formalin fixed sections. Br J Dermatol 2000;142:752-7. [Google Scholar | PubMed]
- 4.Skelton LA. The effective treatment of basal cell carcinoma. Br J Nurs 2009;18:346, 348-50. [Google Scholar | PubMed]
- 5.Feldman S, Pearce DJ, Williford PM. Surgical decision making for basal-cell carcinoma of the face. Lancet Oncol 2008;9:1119-20. [Google Scholar | PubMed]
- 6.Bowen GM, White GL Jr., Gerwels JW. Mohs micrographic surgery. Am Fam Physician 2005;72:845-8. [Google Scholar | PubMed]
- 7.Yanazume S, Douzono H, Yanazume Y, Iio K, Douchi T. New hemostatic method using Mohs’ paste for fatal genital bleeding in advanced cervical cancer. Gynecol Oncol Case Rep 2013;4:47-9. [Google Scholar | PubMed]
- 8.Uno H, Sasaki M, Osamura K, Ohtoshi S, Nakada T, Iijima M. Angiosarcoma (Stewart-Treves syndrome): Palliative role of Mohs’ ointment. J Dermatol 2010;37:852-3. [Google Scholar | PubMed]
- 9.Hoshi M, Iwai T, Oebisu N, Nakamura H. Successful pre-operative local control of skin exposure by sarcoma using combination of systemic chemotherapy and Mohs’ chemosurgery. World J Surg Oncol 2020;18:36. [Google Scholar | PubMed]
- 10.Nemoto K, Okamoto M, Kito M, Aoki K, Suzuki S, Takazawa A, et al. Combined treatment using Mohs’ paste and neoadjuvant chemotherapy for giant gluteal soft tissue sarcoma with malignant fungating wound: A case report. J Surg Case Rep 2019;2019:rjz137. [Google Scholar | PubMed]
- 11.Trost LB, Bailin PL. History of Mohs surgery. Dermatol Clin 2011;29:135-9, vii. [Google Scholar | PubMed]
- 12.Gradishar WJ, Anderson BO, Balassanian R, Blair SL, Burstein HJ, Cyr A, et al. Breast cancer, version 4.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2018;16:310-20. [Google Scholar | PubMed]
- 13.Chiller K, Parker D, Washington C. Myofibrosarcoma treated with Mohs micrographic surgery. Dermatol Surg 2004;30:1565-7. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 Total En Bloc Spondylectomy for Thoracic (T8) Spinal Metastasis of Renal Cell Carcinoma – A Case Report and Review of Literature
July 1, 2025 Total En Bloc Spondylectomy for Thoracic (T8) Spinal Metastasis of Renal Cell Carcinoma – A Case Report and Review of Literature June 1, 2025 Idiopathic Focal Osteonecrosis of T9 Vertebral Body Mimicking a Malignant Tumor: A Case Report
June 1, 2025 Idiopathic Focal Osteonecrosis of T9 Vertebral Body Mimicking a Malignant Tumor: A Case Report April 1, 2025 Pathological Clavicle Fracture Secondary to Breast Carcinoma After a Minor Trauma and Fixed with Open Reduction and Internal Fixation: A Case Report
April 1, 2025 Pathological Clavicle Fracture Secondary to Breast Carcinoma After a Minor Trauma and Fixed with Open Reduction and Internal Fixation: A Case Report July 10, 2024 A Rare Outcome of a Case of Medullary Osteosarcoma of the Femur in Ghana
July 10, 2024 A Rare Outcome of a Case of Medullary Osteosarcoma of the Femur in Ghana