
Floating knee injuries require intramedullary nailing for femoral and tibial fractures, with careful consideration of post-operative fat embolism.
Dr. Pon Aravindhan A Sugumar, Department of Orthopedics, All India Institute of Medical Sciences, New Delhi, India. E-mail: madhan.ponra@gmail.com
Introduction: Floating knee injuries were first described in 1975 by McBryde as concurrent femur and tibial fractures in an ipsilateral limb. They usually occurred in a polytrauma setting and presented with poor functional outcomes with frequent post-operative complications. Management of this injury was based on patient and fracture characteristics and can be done by external fixators, plating, and nailing.
Case Report: A 24-year-old female presented with bilateral floating knees. She was operated on for a left femoral fracture with retrograde nailing when she developed tachycardia and underwent external fixation of the remaining fractures. She later developed a fat embolism which was managed accordingly for the same. After adequate stabilization, her right femur and tibia fractures were fixed by intramedullary nailing through a single percutaneous approach along with nailing for the left tibial fracture. She has satisfactory clinical outcomes on follow-up.
Conclusion: Bilateral floating knee injuries are extremely rare injuries and should be managed on an emergency basis. Intraoperative and post-operative complications should be anticipated and managed accordingly. Good functional outcomes can be obtained by intramedullary nailing.
Keywords: Floating knee, retrograde femoral nailing, and fat embolism.
In the modern industrialized world, every advancement in science has its pros and cons. With the increasingly motorized world with its heavily trafficked roads, the injury patterns in trauma have also been changing. One such traumatic injury pattern that has been increasingly observed in the modern world is the “floating knee”. A floating knee is described as a simultaneous disruption of skeletal integrity on either side of the knee, usually after a high-energy impact, likely in a polytrauma patient. The term “floating knee” was first introduced by Blake and Mcbryde in 1975 [1]. They are also mostly associated with other life-threatening injuries of the head, chest, and abdomen. They are more common in men and can lead to complications such as infection, blood loss, fat embolism, malunion, delayed union, and prolonged hospitalization. Bilateral floating knee is a very rare entity and has been reported in literature only once to date. We report a case of a patient with multiple lower-limb fractures treated surgically with intramedullary nailing in different operative sessions.
The patient, a 24-year-old female, was brought to the emergency department after a road traffic accident with multiple injuries to the body. She did not have any loss of consciousness or any symptoms significant for intracranial bleeding. She was assessed as per Advanced Trauma Life Support protocol as soon as she was received in the trauma bay by the trauma surgeon, neurosurgeon, and orthopedic surgeon. Thomas’s splint was applied to both limbs. Her chest compression test was negative, and she did not have any signs of head or spinal injury. She had tenderness on the pelvic tenderness test signifying some injury to the pelvic ring. On examination of her lower limbs, there was significant swelling with tenderness on her bilateral thighs and legs with a lacerated wound on her left thigh without any neurovascular deficit. She was started on intravenous fluids and analgesics. Antibiotics and TT injections were given as per open injury management protocol. Radiographs of her chest, pelvis, and bilateral lower limb from pelvis to feet were done. The basic trauma series views of different sites were taken, and they revealed fractures of bilateral femoral shafts with bilateral both bone leg fractures (Fig. 1). There was also a closed fracture of the left suprapubic ramus. All fractures were closed except the left femoral shaft fracture which was associated with a Grade 2 open injury. A Focused Assessment with Sonography for Trauma scan was also done to rule out any associated chest or abdominal injury which turned out to be negative. The coronal computed tomography (CT) image is shown in Fig. 2. A full-body CT scan confirmed the absence of any pulmonary or abdominal injury.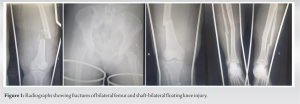
The injury severity score was 21. After initial stabilization, assessment, and routine laboratory workup, the patient was immediately shifted to the operation theater at 1.30 am. She was assessed by an anesthetist and induced under combined spinal epidural anesthesia. No pneumatic tourniquets were applied. Surgery was performed after 2.30 h of the primary injury and locking retrograde intramedullary nailing of the left femur was done under fluoroscopic guidance (AO femoral nail with 1 proximal and 3 distal locking bolts). During surgery, 5 L of Ringer Lactate solution and 500 mL of 5% glucose solution were used for volume expansion. The patient developed tachycardia intraoperatively and further procedures were abandoned. External fixators were applied for the right femoral shaft and bilateral legs as a temporary measure and the patient was shifted to intensive care for stabilization.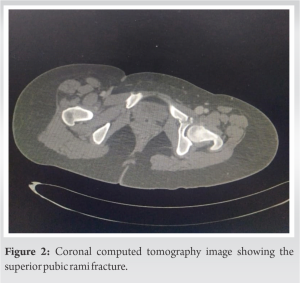
After adequate fluid resuscitation, the patient stabilized and was planned for definitive fixation at a later date. One unit of packed cell blood transfusion was done to tackle post-operative anemia. Postoperatively, the patient developed a fat embolism and her further procedures were deferred for a few days to manage the same. The patient stabilized after adequate monitoring and intensive care. Five days later, the patient was shifted to operation theatre again and definitive fixation of right femoral shaft and leg fractures were done with right retrograde femoral intramedullary nailing (AO femoral nail with 1 proximal and 3 distal locking bolts) and tibial intramedullary nailing (AO expert tibia nail) done through a single midline incision over the ipsilateral knee. The left tibia was also fixed with an intramedullary nail (AO expert tibia nail). There were no intraoperative complications and the patient was shifted to the post-operative ward for monitoring and post-operative care. Blood loss was around 300 mL in total. It was decided to manage the suprapubic ramus fracture conservatively as per protocol (Fig. 3).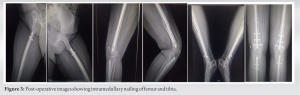
In the post-operative period, the patient was given antibiotics to cover both Gram-positive and Gram-negative organisms with adequate analgesics. Antithrombotic prophylaxis was started with low-molecular-weight heparin. Rehabilitation was started on the immediate post-operative day by a designated physiotherapist. Range of motion exercises was started, and the patient was made to mobilize in bed. Her range of motion in bilateral knees and hips also improved significantly and the patient was discharged on oral analgesics. On her regular post-operative follow-up, she had a satisfactory range of motion in bilateral limbs with good bony union on radiographs. Partial weight-bearing mobilization with the help of a walker was started on the 3rd week and the patient was able to mobilize by herself with little pain. By around the 5th week, she could mobilize with full weight bearing on both limbs with the assistance of a walker. The patient was satisfied with the outcomes and was able to resume her daily routine activities. There were no post-operative complications on follow-up (Fig. 4).
Fraser et al. classified the anatomic lesion in the floating knee in 1978 and our patient had a bilateral Type 1 pattern according to this classification [2]. It subdivides fractures based on intra-articular involvement or not as this defines operative planning. Since our patient had type 1 injury, there was no intra-articular fracture on either side and we proceeded with intramedullary nailing for the diaphyseal fractures. Floating knee is an injury that requires immediate management as it can lead to complications such as ischemia, blood loss, compartment syndrome, and embolism. There have been only a few articles on floating knee injuries in literature with around 30 series published to date with different treatment strategies [3]. The biggest study on this injury pattern was done by Piétu et al. under the GERTRAUM study including 172 subjects [4]. Piétu et al. did a retrospective multicentric observational study on floating knee injuries with a total of 172 patients [4]. He found out that the most preferred procedure for this injury was intramedullary nailing for both the femur and tibia followed by external fixation. They said that the factors determining a bad functional outcome are age, a Type II Fraser pattern, a distal third fracture of the femur, and an open fracture. Single incision reduced operative time though it did not affect the results significantly according to his study [4]. In our study, we did not have any of these bad prognostic factors and we went for a single incision surgery for the right side with multiple incisions for the left side due to the different operative procedures done at two different times. Intramedullary nailing has shown better results than external fixation except in the case of Grade 3 open injuries [3]. Different studies advocate different management options in this type of injury though intramedullary fixation has been most frequently found as the better option. External fixation was found to be the best definitive procedure in case of most fractures, especially when they are open [5-7]. Some advocated nailing for the femur and external fixator for the tibia [6, 8] while few others advocated intramedullary fixation for both [9-13]. Till 1996 antegrade femoral nailing was the method of nailing for femur fracture until Gregory et al. recommended retrograde nailing to be a better option for the injury [10]. Ever since this has been the surgical method of choice for femur fractures in floating knees. A single percutaneous approach for both fractures was later introduced by Ostrum [14]. The absence of a universally validated protocol concerning the timing of definitive surgery is noted in the literature. Nonetheless, guidelines based on patient severity have been suggested, as evidenced by the work of Raju et al. [15]. Accordingly, the decision to perform the surgery at a specific time was made based on these guidelines and tailored to the patient’s individual circumstances, as deemed appropriate by the authors. Surgical stabilization of both fractures is the current recommendation for this type of injury; however, there is no single ideal technique. The implants and surgeries are chosen based on patient and fracture characteristics. Complications such as infections, meniscal injuries, and fat embolism with floating knees are common and have been reported in many studies. Floating knee injuries involving isolation of the knee joint from the ipsilateral limb are very rare injuries that occur in a polytrauma setting. They are managed as an emergency condition and usually present with poor functional outcomes. We hereby present an extremely rare case of bilateral floating knee injuries operated on two different settings with a satisfactory functional outcome. Bilateral floating knee injuries are underreported in our literature.
Bilateral floating knee injuries are extremely rare injuries and should be managed on an emergency basis. Intraoperative and post-operative complications should be anticipated and managed accordingly. Good functional outcomes can be obtained by intramedullary nailing.
Floating knee injuries should be treated as an emergency and intramedullary nailing is a very good option for both femur and tibial fractures in a stable patient. Fat embolism is a possible complication due to femoral fracture and should be anticipated in the post-operative period and managed accordingly.
References
- 1.Blake R, McBryde A Jr. The floating knee: Ipsilateral fractures of the tibia and femur. South Med J 1975;68:13-6. [Google Scholar]
- 2.Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br 1978;60-B:510-5. [Google Scholar]
- 3.Theodoratos G, Papanikolaou A, Apergis E, Maris J. Simultaneous ipsilateral diaphyseal fractures of the femur and tibia: Treatment and complications. Injury 2001;32:313-5. [Google Scholar]
- 4.Piétu G, Jacquot F, Féron JM, et les membres du GETRAUM. Le genou flottant: Étude rétrospective de 172 cas [The floating knee: A retrospective analysis of 172 cases]. Rev Chir Orthop Reparatrice Appar Mot 2007;93:627-34. [Google Scholar]
- 5.Alonso J, Geissler W, Hughes JL. External fixation of femoral fractures. Indications and limitations. Clin Orthop Relat Res 1989;241:83-8. [Google Scholar]
- 6.Anastopoulos G, Assimakopoulos A, Exarchou E, Pantazopoulos T. Ipsilateral fractures of the femur and tibia. Injury 1992;23:439-41. [Google Scholar]
- 7.Barquet A, Massafero J, Durba A, Nin F. Ipsilateral open fracture of the femur and tibia treated using the dynamic ASIF-BM tubular external fixator: Case reports. J Trauma 1991;31:1312-5. [Google Scholar]
- 8.Rooser B, Hansson P. External fixation of ipsilateral fractures of the femur and tibia. Injury 1985;16:371-3. [Google Scholar]
- 9.Behr JT, Apel DM, Pinzur MS, Dobozi WR, Behr MJ. Flexible intramedullary nails for ipsilateral femoral and tibial fractures. J Trauma 1987;27:1354-7. [Google Scholar]
- 10.Gregory P, DiCicco J, Karpik K, DiPasquale T, Herscovici D, Sanders R. Ipsilateral fractures of the femur and tibia: Treatment with retrograde femoral nailing and unreamed tibial nailing. J Orthop Trauma 1996;10:309-16. [Google Scholar]
- 11.Paul GR, Sawka MW, Whitelaw GP. Fractures of the ipsilateral femur and tibia: Emphasis of intra-articular and soft tissue injury. J Orthop Trauma 1990;4:309-14. [Google Scholar]
- 12.Bansal VP, Singhal V, Mam MK, Gill SS. The floating knee. 40 cases of ipsilateral fractures of the femur and the tibia. Int Orthop 1984;8:183-7. [Google Scholar]
- 13.Hee HT, Wong HP, Low YP, Myers L. Predictors of outcome of floating knee injuries in adults: 89 patients followed for 2-12 years. Acta Orthop Scand 2001;72:385-94. [Google Scholar]
- 14.Ostrum RF. Treatment of floating knee injuries through a single percutaneous approach. Clin Orthop Relat Res 2000;375:43-50. [Google Scholar]
- 15.Raju S, Singhi PK, Chidambaram M, Somashekar V, Shanmugasundaram V, Singhi PK. Floating knee injuries-an analytical study using a conglomerated comprehensive classification. Injury 2021;52:3091-8. [Google Scholar]





