
Fibrolipomatous hamartoma is a rare congenital benign tumor that needs to be histopathologically confirmed. Surgical debulking under a microscope using high magnification is the treatment for symptomatic cases and prevents complications.
Dr. Mantu Jain, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar - 751 019, Odisha, India. E-mail: montu_jn@yahoo.com
Abstract
Introduction: Fibrolipomatous hamartomas are rare congenital benign tumors that can affect the nerves. The symptoms arise due to compression and may require surgical excision.
Case Report: A man in his mid-20s suffered swelling over the volar aspect of the left forearm and hand for 4 months. He was symptomatic. A soft, non-tender swelling of size 6 × 4 cm was present over the flexor aspect of the left forearm and palm, with features suggestive of median nerve compression. Magnetic resonance imaging and electromyography were performed. Decompression of the carpal tunnel was performed with debulking of fibrofatty elements and fine dissection of the neural elements.
Conclusion: This case report demonstrates a rare fibrolipomatous hamartoma encompassing the median nerve, which required surgical excision.
Keywords: Fibrolipomatous hamartoma, median nerve, surgical excision.
Fibrolipomatous hamartoma (FLH) is a rare congenital benign tumor that can present in childhood or adulthood [1]. Although infrequent, there are reports of affection of the median nerve, the radial or ulnar nerves of the upper limb, and the sciatic or plantar nerves of the lower limb [2-6]. The degree and length of the nerve affected determine the symptoms.
A male patient in his mid-20s presented to the outpatient department with 4 months of swelling over the volar aspect of the left forearm and hand. The swelling was insidious in onset, which initially started as a forearm swelling and slowly progressed into the palm with a gradual increase in size. The patient complained of tingling and numbness over the palm and radial 3½ fingers (middle, index, and thumb fingers) with pain on excessive limb use. There was no history of fever or trauma preceding the onset of the swelling. No other swellings are present elsewhere. A continuous, soft, non-tender, non-compressible, immobile, smooth swelling measuring 6 × 4 cm was evident over the flexor aspect of the left forearm extending from the distal third of the forearm to the proximal palmar crease (figure 1a, b). Along the course of the median nerve, Tinel’s sign was positive at the wrist and radial three and a half fingers. Both Phalen’s and Durkan’s tests came back positive, pointing to possible median nerve compression at the carpal tunnel level. The wrist and fingers were moving usually.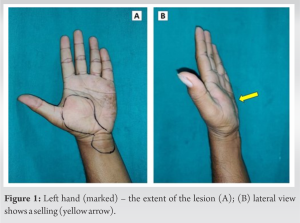
On electromyography, there was a delay in nerve conduction. Magnetic resonance imaging (MRI) was suggestive of the swelling arising from the median nerve abutting the flexor musculature passing through the carpal tunnel and involving the palmar cutaneous branch (figure 2a, b). The patient was counseled for surgical excision.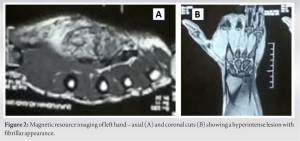
Intraoperatively, the tumor encapsulated the median nerve and the nerve was edematous (figure 3a). Under microscope, the capsule was opened, revealing the grayish to bluish–white substance dispersed around and involving the fascicles. The tumor could not be removed separately from the nerve substance. A segment of a cutaneous branch of the median nerve was sent for histopathological examination. Decompression of the carpal tunnel was performed with debulking of fibrofatty elements and fine dissection of the neural elements (figure 3b).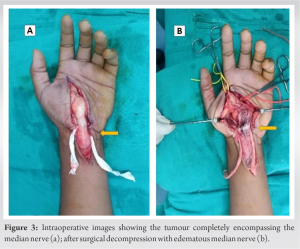
Histopathology revealed lobules of adipocytes and bland fibrosis with ropy collagen deposition entrapping the nerve. The fibromatous or lipomatous component did not show any nuclear atypia or other features of malignancy suggestive of FLH (figure 4a, b).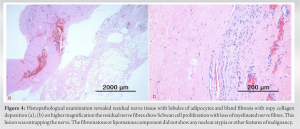
Postoperatively, the patient was on temporary splintage for a week and physiotherapy was performed for 3 months. At 6-month follow-up, the patient was completely free of symptoms. There was no weakness or loss of sensation in the involved limb.
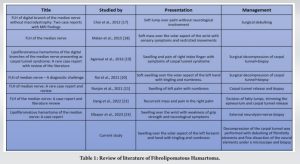
FLH is a relatively rare but benign condition. The exact etiology is unknown, but the hypertrophy of mature fat and fibroblasts in the epineurium has been postulated [7]. FLH of the median nerve presents as a fusiform swelling of the nerve itself rather than a clearly defined swelling coming from the nerve [8]. Opening the epineurium revealed no obvious edema. We found that fascicles were enlarged, suggestive of a tumor, and the nerve material appeared gray to bluish. The swelling, which was palpable and well-defined swelling was not seen intraoperatively but rather fibrofatty tissue merging with the fascicles, giving the nerve a fusiform look. FLH can have neuropathy symptoms as it is attached to the nerve and increases in size [9]. The intraneural spread of the tumor itself is not the cause of these symptoms but depends on the severity of the compression. Involvement of the median nerve will give rise to carpal tunnel syndrome (CTS), and there are cases of macrodactyly also reported [10]. When it affects other parts body, such as the neck, and lower limb, it can give brachialgia or sciatica. Few reports involving the radial or ulnar nerves have also been described [11,12]. The gold standard of investigation is MRI [5]. The MRI findings are quite pathognomonic, which helps to differentiate from other benign tumors [13]. On T1-weighted images, it appears as low-signal nerve bundles encircled by high-signal fibrolipomatous tissue [14]. A conspicuous increase in adipose tissue in a fibrous network that involves the nerve sheath, muscles, and subcutaneous tissue is characteristic. Adding a diffusion-weighted imaging sequence in association with conventional MRI improves the diagnosis [15]. FLH can be managed conservatively, and few require surgical exploration [16]. The characteristic MRI findings do not make the biopsy prudent before surgery [10]. Medications such as pain relievers or anti-inflammatory drugs may be prescribed to manage pain and inflammation associated with FLH. Surgery is indicated for symptomatic benign lesions [11]. Often, the FLH is seen to encompass the nerve root, and therefore, complete enblock excision may not be possible without grafting. Piecemeal decompression should suffice. Sarp and Pekcevik have reported internal neurolysis for a case report of giant lipomatosis of the sciatic nerve [6]. The details of reported cases and their management are elaborated in Table 1. Debulking of the lesion is possible, but extensive intraneural dissection runs the risk of ischemic consequences. Some authors recommend complete excision of the mass along with nerve repair, however, this can cause significant neurological damage [24]. Therefore, we advocate precise and careful intraneural dissection under a microscope with higher magnification.
It’s crucial to note that treatment decisions should be individualized based on the specific characteristics of the FLH and the patient’s overall health. Extensive intraneural dissection has a risk of ischemic complications. Some authors recommend complete excision of the mass along with nerve repair; however, this can cause significant neurological damage. Microsurgical separation of the neural components under the microscope with higher magnification, followed by carpal tunnel release, was sufficient in our case of FLH encompassing the median nerve and producing symptoms of CTS.
FHL is a benign condition. The presentation is usually asymptomatic until there is a compression of the nerve rather than intraneural involvement by the tumor. A thorough clinical and radiographic assessment is required to diagnose this uncommon lesion. Lipomatosis of the nerve is not precisely or consistently treated. Microsurgical dissection of the neural components under a microscope and post-operative care and physical therapy can produce positive outcomes when decompression is not an option.
References
- 1.Silverman TA, Enzinger FM. Fibrolipomatous hamartoma of nerve. A clinicopathologic analysis of 26 cases. Am J Surg Pathol 1985;9:7-14. [Google Scholar | PubMed]
- 2.Gouldesbrough DR, Kinny SJ. Lipofibromatous hamartoma of the ulnar nerve at the elbow: Brief report. J Bone Joint Surg Br 1989;71:331-2. [Google Scholar | PubMed]
- 3.Herrick RT, Godsil RD Jr., Widener JH. Lipofibromatous hamartoma of the radial nerve: A case report. J Hand Surg Am 1980;5:211-3. [Google Scholar | PubMed]
- 4.Johnson RJ, Bonfiglio M. Lipofibromatous hamartoma of the median nerve. J Bone Joint Surg Am 1969;51:984-90. [Google Scholar | PubMed]
- 5.Khadka S, Adhikari P, Regmi PR, Timilsina B, Thapa AS, Panta BR, et al. Lipofibromatous hamartoma of sciatic nerve: A case report. Ann Med Surg (Lond) 2022;81:e104542. [Google Scholar | PubMed]
- 6.Sarp AF, Pekcevik Y. Giant lipomatosis of the sciatic nerve: Unique magnetic resonance imaging findings. Iran J Radiol 2016;13:e20963. [Google Scholar | PubMed]
- 7.Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. From the archives of the AFIP: Benign musculoskeletal lipomatous lesions. Radiographics 2004;24:1433-66. [Google Scholar | PubMed]
- 8.Ha JF, Teh BM, Abeysuriya DT, Luo DY. Fibrolipomatous hamartoma of the median nerve in the elbow: A case report. Ochsner J 2012;12:152-4. [Google Scholar | PubMed]
- 9.Berry MG, Mallucci P, Banwell PE, Heywood AJ. Fibrolipoma of the median nerve. J R Soc Med 1999;92:408-9. [Google Scholar | PubMed]
- 10.Ulrich D, Ulrich F, Schroeder M, Pallua N. Lipofibromatous hamartoma of the median nerve in patients with macrodactyly: Diagnosis and treatment of a rare disease causing carpal tunnel syndrome. Arch Orthop Trauma Surg 2009;129:1219-24. [Google Scholar | PubMed]
- 11.Bibbo C, Warren AM. Fibrolipomatous hamartoma of nerve. J Foot Ankle Surg 1994;33:64-71. [Google Scholar | PubMed]
- 12.Philp L, Naert KA, Ghazarian D. Fibrolipomatous hamartoma of the nerve arising in the neck: A case report with review of the literature and differential diagnosis. Am J Dermatopathol 2015;37:e78-82. [Google Scholar | PubMed]
- 13.Ogose A, Hotta T, Higuchi T, Katsumi N, Koda H, Umezu H. Fibrolipomatous hamartoma in the foot: Magnetic resonance imaging and surgical treatment: A report of two cases. J Bone Joint Surg Am 2002;84:432-6. [Google Scholar | PubMed]
- 14.Al-Qattan MM. Lipofibromatous hamartoma of the median nerve and its associated conditions. J Hand Surg Br 2001;26:368-72. [Google Scholar | PubMed]
- 15.Ly JQ, Bui-Mansfield LT, SanDiego JW, Beaman NA, Ficke JR. Neural fibrolipoma of the foot. J Comput Assist Tomogr 2003;27:639-40. [Google Scholar | PubMed]
- 16.Okubo T, Saito T, Mitomi H, Takagi T, Torigoe T, Suehara Y, et al. Intraneural lipomatous tumor of the median nerve: Three case reports with a review of literature. Int J Surg Case Rep 2012;3:407-11. [Google Scholar | PubMed]
- 17.Choi W, Jung JY, Song IN, Lee JS, Lee TJ, Jung YY. Fibrolipomatous hamartoma of digital branch of the median nerve without macrodystrophy: Two case reports with magnetic resonance imaging findings. J Korean Soc Radiol 2012;67:483-7. [Google Scholar | PubMed]
- 18.Malan L, Bezuidenhout AF, Banderker E. Fibrolipomatous hamartoma of the median nerve. S Afr J Rad 2015;19:886. [Google Scholar | PubMed]
- 19.Agrawal R, Garg C, Agarwal A, Kumar P. Lipofibromatous hamartoma of the digital branches of the median nerve presenting as carpal tunnel syndrome: A rare case report with review of the literature. Indian J Pathol Microbiol 2016;59:96-8. [Google Scholar | PubMed]
- 20.Rai V, Sabhikhi GS, Sircar P, Kumar D, Kundra R, Jeyaraman M. Fibrolipomatous hamartoma of median nerve - a diagnostic challenge. J Orthop Case Rep 2021;11:69-73. [Google Scholar | PubMed]
- 21.Ranjan R, Kumar R, Jeyaraman M, Kumar S. Fibrolipomatous hamartoma (FLH) of median nerve: A rare case report and review. Indian J Orthop 2020;55:267-72. [Google Scholar | PubMed]
- 22.Dang YT, Ou XH, Wang Q, Zhou YP, Wei DK, Xie F, et al. Fibrolipomatous hamartoma of the median nerve: A case report and literature review. Invest Clín 2022;63:400-13. [Google Scholar | PubMed]
- 23.Elbayer AM, Alharami S, Elhessy AH. Lipofibromatous hamartoma of the median nerve: A case report. Cureus 2023;15:e33516. [Google Scholar | PubMed]
- 24.Siqueira MG, Martins RS, Foroni L, de Oliveira AJ, Lordelo G, Heise CO. Fibrolipomatous hamartoma of the median nerve: An unusual cause of carpal tunnel syndrome. Clin Case Rep 2023;11:e7022. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair
June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair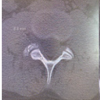 April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report
April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report March 1, 2026 A Rare Case of Calcific Tendinitis of the Elbow Mimicking Lateral Epicondylitis: Diagnostic Challenges and Surgical Management
March 1, 2026 A Rare Case of Calcific Tendinitis of the Elbow Mimicking Lateral Epicondylitis: Diagnostic Challenges and Surgical Management