
Retrograde humerus nail-plate combination is a novel fixation technique that can be utilized in this complex fracture pattern and has not been previously discussed in the literature.
Dr. Mark LaGreca, Department of Orthopedic Surgery, Philadelphia College of Osteopathic Medicine, 4170 City Avenue, Suite 101. Philadelphia, Pennsylvania. E-mail: ml194690@pcom.edu
Introduction: Humeral shaft and distal humerus fractures have several different treatment options, including plate fixation and intramedullary nailing. Each has its own benefits, but typically, they are not used in conjunction. While nail-plate combinations (NPCs) have become more common in the lower extremity, literature on their use in upper extremity fractures remains scarce.
Case Report: A 74-year-old right-hand dominant male presented after a fall with a closed left transverse midshaft humerus fracture and an associated supracondylar distal humerus fracture with intercondylar extension through a medial column. Due to the segmental nature of his injury, medial column plating was used in conjunction with a retrograde intramedullary nail to obtain anatomic reduction and fixation of the articular injury while stabilizing the midshaft humerus fracture with minimal soft tissue disruption. The patient was recommended non-weight bearing through his left arm for 6 weeks, at which point he returned to weight bearing as tolerated. He was allowed to range his left elbow after 2 weeks. His left elbow range of motion at the 4-month follow-up was 20-135 degrees, and he reported minimal pain.
Conclusion: The retrograde NPC should be considered in segmental humeral fractures involving the distal articular surface and midshaft humerus fractures as it limits violation of the soft tissue while avoiding iatrogenic disruption of the articular surface at the shoulder or elbow.
Keywords: Trauma, complex fracture, humerus fracture, nail-plate combination.
The surgical approach and treatment choice for humeral shaft and distal humerus fractures can be challenging, depending on the fracture location and pattern. Open reduction and internal fixation (ORIF) of distal humerus fractures with plate and screw constructs have become the predominant treatment option, particularly in younger patients or those with normal functional status [1]. Humeral shaft fractures can be treated either with ORIF or intramedullary nailing (IMN). Antegrade humeral IMN is typically used for proximal third and mid-humeral shaft fractures but carries the risk of rotator cuff injuries, radial nerve impingement, and injury to the musculocutaneous nerve with the anterior-posterior distal interlock screw placement [2, 3]. The less common approach of retrograde humeral IM nailing attempts to avoid such complications and can effectively treat distal third humeral shaft and midshaft fractures, but elbow stiffness, comminution of the posterior cortex due to the shape of the distal humerus, and increased difficulty of the procedure are noted as complications of this approach [2, 3]. While the choice between IMN and ORIF for humeral shaft fractures remains controversial, theoretically, an intramedullary device allows for greater preservation of soft tissue [4]. In recent years, the combination of IMN and ORIF constructs has gained popularity for both femur fractures and tibia fractures [5, 6]. These constructs offer several advantages by conferring both the benefits of intramedullary fixation, such as increased stability for immediate weight-bearing, and plate fixation, such as allowing for improved control of proximal or distal fragments. While the use of this concept has been well established in the lower extremity, the literature on the use of nail-plate combinations (NPC) is scarce with regard to the humerus [7, 8]. This case report details the use of an NPC involving a retrograde IMN and medial plate fixation for a comminuted midshaft humerus fracture with a supracondylar distal humerus fracture with intercondylar extension through a medial column split.
Initial presentation
A 74-year-old right-hand dominant male presented after a fall with a closed left transverse midshaft humerus fracture with an associated supracondylar distal humerus fracture with intercondylar extension through a medial column (Fig. 1 and 2). The patient had no other injuries and was neurovascularly intact on presentation. He was an independent ambulator who lived alone. The patient was treated with a splint in the emergency room, with plans for operative fixation the next day.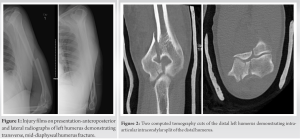
Surgical procedure
After administration of general anesthesia, the patient was placed in a lateral position with the arm hanging over a radiolucent paint roller positioner. A posterior incision was made, followed by a triceps split between the long and lateral heads of the triceps. The fracture sites over the articular surface were irrigated and cleaned. The intra-articular medial condyle fragment was reduced using multiple Weber clamps and compression was achieved with a 2.4-mm screw proximally and a 4.0-mm cannulated screw at the level of the joint. With the olecranon fossa of the distal humerus exposed at this stage, attention was turned to the humeral shaft fracture. The dorsal cortex of the humerus was perforated using a drill bit just proximal to the olecranon fossa to create a window for the reamer. Following sequential reaming, a 7 mm × 240 mm nail was inserted into the intramedullary canal, and subsequent interlocking screw fixation was performed. Finally, with the humeral shaft and articular elbow surface stabilized, a four-hole medial distal humerus plate was applied to the medial distal humerus in antiglide mode (Fig. 3). Following closure, the patient was placed in a long arm splint with a non-weight-bearing (NWB) status of his left upper extremity (LUE) (Fig. 4). The patient had an uneventful post-operative course and was discharged on post-operative day 1.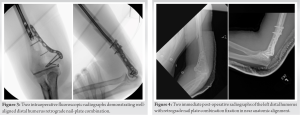
Follow-up
The patient was in a splint for 2 weeks and then began range-of-motion exercises. He was NWB for 6 weeks after surgery and advanced to progressive weight bearing as tolerated. He was admitted to the hospital for a mechanical fall approximately 1 month after surgery and was evaluated by the orthopedic team. He reported some pain control issues with his LUE, but the incision was well healed and the patient remained neurovascularly intact. The patient was then seen in the office 1 month later and reported significant improvement in pain. Despite his residual swelling of the LUE, his elbow range of motion was 20–135°. At his 4-month post-operative follow-up, the patient reported minimal pain at 2/10 intensity, and radiographs demonstrated appropriate callus formation (Fig. 5 and 6).

This case report describes a comminuted humeral shaft fracture with an associated distal humerus fracture involving intercondylar extension that was treated with retrograde IMN and plate fixation. While there is an ongoing debate over the use of IMN versus ORIF for midshaft humerus fractures, segmental fractures such as the one presented in this case pose a more challenging and complicated issue. The construct chosen for this case provided absolute stability of the articular surface at the distal humerus fracture site while allowing preservation of the soft tissue around the midshaft humerus fracture, providing a good environment for secondary bone healing by utilizing intramedullary stabilization. The use of NPCs in the lower extremity has become commonplace as it provides greater resistance against torsional forces from plate fixation while also placing an intramedullary device that allows for earlier tolerance of axial loading [5, 9]. In this case, the segmental nature of the humerus injury allowed for this construct to take advantage of both fixation methods, as previously described. Furthermore, applying the distal humerus plate in antiglide mode above the end of the humeral nail decreased the stress riser between the two constructs (Fig. 4 and 6). In comparison to anterograde nailing, the retrograde approach avoids joint disruption and damage to any articular cartilage as it is inserted through the olecranon fossa. One of the primary concerns remains the risk of iatrogenic fracture due to the angle of entry and strength of the posterior cortex; however, innovative techniques such as creating drill holes in a rhomboid configuration and connecting them through burring have been developed to decrease this risk [10]. The triceps split approach utilized in this case exposed the start point for the retrograde humeral nail as the distal posterior surface of the distal humerus was exposed for the articular reduction. The triceps are commonly split to access the entry point, so it is important to monitor triceps function and elbow stiffness during follow-up visits [2]. In this case, the patient maintained excellent range of motion at the 2 and 4-month follow-up visits. Bi et al. described a case involving the use of an NPC for a complex proximal humerus fracture with an associated proximal third humeral shaft fracture [7]. After obtaining provisional reduction with K-wire fixation, an antegrade humeral nail was used to provide intramedullary support of the fracture site and better control of the distal segment without creating an extensive injury to the soft tissue. An anteromedial locking plate was then applied to provide anatomic fixation and support at the medial aspect of the humerus to prevent varus collapse [7]. Ganta et al. published a case series of three humerus NPCs, including one for increased stability in the setting of an induced membrane technique for non-union, a complex proximal humerus fracture with metadiaphyseal extension, and a segmental fracture involving a four-part proximal humerus fracture with an associated midshaft humerus fracture [8]. While these case reports describe several situations in which an NPC may be advantageous, they all involve more proximal fractures. In addition, all of the described cases involved an antegrade nail with adjunctive plate fixation. The current study’s use of a retrograde humeral nail is uniquely situated within the described segmental fracture pattern.
The retrograde NPC should be considered in segmental humeral fractures involving the distal articular surface and midshaft humerus fractures, as it limits violation of the soft tissue while avoiding iatrogenic disruption of the articular surface at the shoulder or elbow. Although encouraging, long-term studies and biomechanical optimization of the retrograde NPCs should be investigated.
Distal humerus nail plate combination treatment for complex humerus fractures should be further studied as it allows for the preservation of soft tissue for the humeral shaft segment and allows anatomic reduction at the articular surface. This case report demonstrates a patient who did very well postoperatively.
References
- 1.Amir S, Jannis S, Daniel R. Distal humerus fractures: A review of current therapy concepts. Curr Rev Musculoskelet Med 2016;9:199-206. [Google Scholar]
- 2.Sharma GM, Bhardwaj AR, Shah S. Antegrade versus retrograde nailing in humeral shaft fractures: A prospective study. J Clin Orthop Trauma 2020;11:S37-41. [Google Scholar]
- 3.Yi JW, Lee JS, Cho HJ. Retrograde intramedullary nailing for humerus fracture in a supine position: Performing an unfamiliar procedure in a familiar position. Clin Orthop Surg 2017;9:392-5. [Google Scholar]
- 4.Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop 2010;81:216-23. [Google Scholar]
- 5.Kontakis MG, Giannoudis PV. Nail plate combination in fractures of the distal femur in the elderly: A new paradigm for optimum fixation and early mobilization? Injury 2023;54:288-91. [Google Scholar]
- 6.Garala K, Ramoutar D, Li J, Syed F, Arastu M, Ward J, et al. Distal femoral fractures: A comparison between single lateral plate fixation and a combined femoral nail and plate fixation. Injury 2022;53:634-9. [Google Scholar]
- 7.Bi C, Wu J, Wu X. Clinical application of nail-plate fixation in the treatment of complex proximal third humeral fracture: A case report and literature review. Orthop Surg 2023;15:2187-92. [Google Scholar]
- 8.Ganta A, Wang C, Konda SR, Egol KA. Nail plate combination in the upper extremity: Surgical technique and clinical application. Eur J Orthop Surg Traumatol 2022;32:443-8. [Google Scholar]
- 9.Yoon RS, Bible J, Marcus MS, Donegan DJ, Bergmann KA, Siebler JC, et al. Outcomes following combined intramedullary nail and plate fixation for complex tibia fractures: A multi-centre study. Injury 2015;46:1097-101. [Google Scholar]
- 10.Biber R, Zirngibl B, Bail HJ, Stedtfeld HW. An innovative technique of rear entry creation for retrograde humeral nailing: How to avoid iatrogenic comminution. Injury 2013;44:514-7. [Google Scholar]








