
This article discusses a novel method of correcting tibial eminence fractures resulting from ACL avulsion injuries in the pediatric population without the need for intra-articular screws. Instead, the bony fragment is secured to the tibial eminence using thick non-absorbable sutures. This all-arthroscopic approach is less invasive while still providing excellent visualization of the surgical site. We hope this procedure will be further explored as an alternative approach to managing this injury.
Mr. Ethan Kosco, University of Toledo College of Medicine and Life Sciences, 3000 Arlington Ave, Toledo, Ohio. E-mail: ekosco@rockets.utoledo.edu
Abstract
Introduction: Tibial eminence fractures resulting from the avulsion of the anterior cruciate ligament (ACL) insertion are a common knee injury in the pediatric population. This injury is traditionally corrected through internal fixation using a guide pin and a cannulated screw. Due to the reported consequences of cannulated screws impinging on the joint space, we explored an alternative procedure to address this injury without the use of cannulated screws. We believe this is the first report of an alternate and improved procedure for repairing a tibial eminence fracture caused by ACL avulsion using non-absorbable sutures to secure the bony fragment back onto the tibial eminence.
Case Report: We report the diagnosis, treatment, and follow-up of a 15-year-old Caucasian male who suffered a tibial eminence fracture associated with an ACL avulsion following a tackle football injury. We utilized a new all-arthroscopic procedure that involved securing the bony fragment of the tibial eminence using sutures that were passed through the ACL and proximal tibial using interosseous bone tunnels.
Conclusion: This novel procedure successfully eliminates the need for intra-articular screws in the adolescent knee while treating tibial avulsion fractures - as supported by the patient’s marked radiographical and symptomatic improvement at the 2, 6, and 12-week follow-up visits.
Keywords: Anterior cruciate ligament, tibial eminence, pediatrics.
Tibial eminence fractures result from an avulsion fracture of the anterior cruciate ligament (ACL) insertion [1]. They are most common in the pediatric population, comprising nearly 5% of knee injuries in children between the ages of eight and 14 years [2,3]. Tibial eminence fractures are often caused by competitive sports, such as cycling and skiing when the knee is subject to stress that causes the immature subchondral bone to fail before the ACL [4-6]. This injury is extremely rare in adults due to their increased bone density compared to adolescents. However, there have been infrequent reports of this condition being caused by high-velocity motor vehicle trauma in that demographic [5]. Once radiographic imaging and magnetic resonance imaging (MRI) confirm the diagnosis of a tibial eminence fracture, treatment depends on the extent of the avulsion. In low-grade injuries, the knee can be treated non-operatively via immobilization for 6–12 weeks [4]. High-grade avulsions require surgical intervention through open reduction and internal fixation [4]. Regardless of the intervention, it is essential to treat tibial eminence fractures to ensure proper development of the knee and reduce progression to non-union, malunion, and arthrofibrosis [7]. In this paper, we report a case of a pediatric tibial eminence fracture following a contact sports injury, corrected via all-arthroscopic reduction and fixation.
A 15-year-old male with a non-significant health or social history presented for an office visit with left knee pain, swelling, and inability to bear weight after being tackled from the rear while playing football. X-rays (Fig. 1a and b) were negative, but the patient could not extend his knee past 30 degrees.

Subsequent MRI revealed a distal neurovascular injury and an avulsion of the tibial plateau involving both tibial eminences. There was approximately 6 mm of proximal retraction along the anterior osseous margin. Because the fracture protruded over the medial meniscus and intrameniscal ligament, closed reduction was determined to be ineffective (Fig. 2a-c).

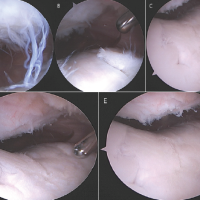
There was no discrete ACL fiber disruption nor other ligament or meniscus damage noted on the MRI. Regarding the extensor mechanism, there was no significant tendinosis or discrete tear. The patella was uninjured and positioned within the femoral groove. There was a large joint effusion with internal complexity and synovial thickening. Following appropriate clearances, the patient was taken to the operating room for an all-arthroscopic reduction and internal fixation. Pre-operative antibiotics were administered within 1 h of incision. Venous thrombosis prophylaxis was ordered including a unilateral sequential compression device. The leg was positioned in extension and blocked at 30 degrees. Once diagnostic arthroscopy began, the eminence fracture was observed to be displaced and involving the anterior half of the medial tibial plateau (Fig. 3a). As noted in the MRI, the fracture was overlying the anterior horn of the medial meniscus and intrameniscal ligament. In addition, the hematoma was visualized above the tibial plateau (Fig. 3a). Arthroscopic repair of the fracture began with removing the early fracture callus and fracture hematoma (Fig. 3b). A probe was used to guide the eminence fracture underneath the intrameniscal ligament and anterior horn of the medial meniscus (Fig. 3c). The fragment was sutured into place using heavy non-absorbable sutures that were passed through the ACL and proximal tibia using interosseous bone tunnels and ACL tibial guides (Fig. 3d and e). The sutures were tied over a bone bridge for secure fixation and the range of motion was tested to ensure proper extension. Further diagnostic arthroscopy was performed to assess the medial and lateral meniscus, ACL, posterior cruciate ligament, and additional chondral injury before draining the knee and locking it into extension using a hinged knee brace (Fig. 3f and g).

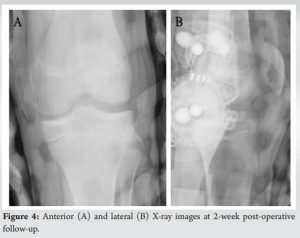
Two-week follow-up X-rays showed a reduction of the eminence fracture (Fig. 4). A brace and crutches were used until 6 weeks post-operation, at which physical therapy was started to improve the range of motion.
Tibial eminence fractures represent avulsion fractures resulting from underdeveloped subchondral bone failing under the tension of the ACL. Because these fractures often occur due to immature subchondral bone, children between the ages of eight and fourteen are at high risk [8]. This injury is usually caused by a sudden contraction of the quadriceps muscle that puts significant strain on the patellar tendon, explaining the propensity of this injury for children who also play competitive or contact sports [9]. Tibial eminence fractures make up 2–5% of knee injuries in the pediatric population and 14% of ACL injuries in that demographic – leading to an overall prevalence of three per 100,000 children per year [2,3,10]. The signs of a tibial eminence fracture are non-specific, such as knee pain, swelling, restricted motion, and inability to bear weight. However, radiographic imaging will present an avulsion of the tibial eminence. Further computed tomography/MRI imaging will characterize the extent of the injury and show soft-tissue damage. Specifically, the ACL will be unanchored and displaced from the tibial plateau. In addition, tibial eminence fractures are associated with meniscal, capsular, and collateral ligament tears, so it is important to obtain proper imaging to ensure appropriate treatment and recovery of the knee [4]. Tibial eminence fractures and associated ACL avulsion fractures are classified into four types based on the extent of bone damage: non-displaced (Type I), partially displaced or hinged (Type II), completely displaced (Type III), or displaced and comminuted (Type IV). Type III fractures are subdivided into “rotated” and “non-rotated” [1]. The type of injury dictates the need for surgical intervention. In a Type I fracture, the knee is occasionally drained of hemarthrosis for symptomatic relief and immobilized in a cast for 6–12 weeks. There remains controversy about whether Type 2 fractures require surgery. However, reduction and internal fixation are the most common treatments for this type of fracture, as residual displacement following closed reduction can lead to an impingement in the femoral notch and follow-up surgery [4]. Types 3 and 4 fractures, and those that feature intra-articular extension, require surgery to prevent disruption of proper knee development in the adolescent patient. The reduction and internal fixation procedure to repair a tibial eminence fracture traditionally involves inspecting the meniscus for any collateral damage, determining the extent of chondral injury, and removing free fragments [11]. Reduction is then performed using a reduction clamp to return the bony fragment to its original position, and internal fixation is achieved using a guide pin and a cannulated screw to secure the fragment back into position. Stability and range of motion tests are carried out before wound closure to ensure recovery of correct knee anatomical structure [11]. We report an alternate and improved procedure for repairing a tibial eminence fracture caused by ACL avulsion. After a thorough literature review, we could not find any reported cases that utilized this surgical procedure. Because this procedure eliminates the need for intra-articular screws in the adolescent knee, we believe this is an improved method for treating tibial avulsion fractures – as supported by the patient’s marked radiographical and symptomatic improvement at the 2, 6, and 12-week follow-up visits. Therefore, this all-arthroscopic surgical approach demonstrates a new and less-invasive method of fracture reduction and addressing tibial eminence fractures attributed to ACL avulsions while still providing excellent visualization of the surgical site. We hope this procedure can be further applied in the treatment of adolescent athletes who suffer from this injury.
Tibial eminence fractures are a relatively common knee injury in the pediatric population resulting from competitive and contact sports. They present with severe knee pain, swelling, and reduced mobility in the affected knee. The diagnosis is confirmed through a radiograph, and MRI is used for further characterization of the injury. Although non-invasive treatments are available for low-grade injuries, avulsion fractures often must be stabilized via all-arthroscopic reduction and internal fixation to ensure proper growth and development of the knee. As far as we know, this is the first case that utilized non-absorbable sutures to secure the bony fragment to the tibial eminence without the use of screws.
We present a novel technique for correcting tibial eminence fractures resulting from ACL avulsion injuries in the pediatric population. This procedure eliminates the need for screws and instead stabilizes the bony fragment with thick, non-dissolvable sutures. We believe further data collection regarding this procedure will demonstrate reduced long-term complications observed in screw insertion into the intercondylar notch.
References
- 1.Coyle C, Jagernauth S, Ramachandran M. Tibial eminence fractures in the paediatric population: A systematic review. J Child Orthop 2014;8:149-59. [Google Scholar | PubMed]
- 2.Luhmann SJ. Acute traumatic knee effusions in children and adolescents. J Pediatr Orthop 2003;23:199-202. [Google Scholar | PubMed]
- 3.Eiskjaer S, Larsen ST, Schmidt MB. The significance of hemarthrosis of the knee in children. Arch Orthop Trauma Surg (1978) 1988;107:96-8. [Google Scholar | PubMed]
- 4.Meyers, A. L., Tiwari, V., & Nelson, R. (2024, January 7). Tibial eminence fractures. StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK556008 [Google Scholar | PubMed]
- 5.Patterson SP, Christiansen GB, Daffner RH. Avulsion fracture of the tibial eminence in an adult with a unique mechanism of injury. Radiol Case Rep 2018;13:843-7. [Google Scholar | PubMed]
- 6.Skak SV, Jensen TT, Poulsen TD, Stürup J. Epidemiology of knee injuries in children. Acta Orthop Scand 1987;58:78-81. [Google Scholar | PubMed]
- 7.Kendall NS, Hsu SY, Chan KM. Fracture of the tibial spine in adults and children. A review of 31 cases. J Bone Joint Surg Br 1992;74:848-52. [Google Scholar | PubMed]
- 8.Anderson CN, Anderson AF. Tibial eminence fractures. Clin Sports Med 2011;30:727-42. [Google Scholar | PubMed]
- 9.Carius BM, Long B. Osgood-schlatter disease as a possible cause of tibial tuberosity avulsion. Cureus 2021;13:e13256. [Google Scholar | PubMed]
- 10.Elsaid A, Zein AM, Elshafie M, Said NS, Mahmoud AE. Arthroscopic single-tunnel pullout suture fixation for tibial eminence avulsion fracture. Arthrosc Tech 2018;7:e443-52. [Google Scholar | PubMed]
- 11.Chawda R, Patel V, Ninama DM, Patel H. Anterior tibial spine (ACL avulsion) fracture treated with open reduction and fixation with screw: Surgical technique, functional and clinico-radiological outcomes. Int J Res Orthop 2019;5:340. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report
December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report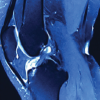 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide