
Trend toward unicompartmental knee replacement being offered as a treatment modality for isolated medial compartmental osteoarthritis in India compared to global numbers.
Dr. Haemanath Pandian, Department of Orthopaedics, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India. E-mail: haemanath@gmail.com
Introduction: The purpose of this study is to analyze the trend of unicompartmental knee replacement (UKR) in India, based on the data obtained from the Indian joint registry, in comparison with the global trends.
Materials and Methods: This study is a retrospective analysis of data from an Indian joint registry for cases performed between 2016 and 2021. A total of 1086 UKRs were identified and the following information was analyzed: demographic data, diagnosis leading to primary UKR, year-wise surgeon inclination toward UKR, implant preference, regions where UKR was preferred, and the effect of robotics in UKR. UKR registry data were compared with the registry data from the UK (NJR), Sweden (SKAR), Australia (AOJR), and the USA (AJRR).
Results: One thousand eighty-six UKRs were included in the study: The vast majority of them (97%) were implanted due to primary osteoarthritis followed by deformity (2%), as in accordance with other registries. Since 2016, though very minimal, there has been a gradual increase in the numbers and the percentage of cases contributed by UKR, of all knee replacements with the maximum of 2.85% reported in 2019. The same has been observed in the global trends as well. Oxford knees (60%) are the most preferred implants followed by journey uni knee (20%) in India. The cities where more unicompartmental knee are performed are in the order of Mumbai (32.78%), Faridabad (9.39%), Pune (7.92%), and Hyderabad (6.35%). Surgeon preference for robotic assisted UKR is increasing, accounting for 34% of UKR in 2020, which is in coherence with AOJR.
Conclusion: The percentage of knee replacements contributed by UKR is increasing globally and the same trend can be observed in India. Oxford phase III prosthesis are the most preferred UKR prosthesis. UKRs are mostly performed in selected pockets of India, with Mumbai almost contributing to one-third of all the cases. The use of robotics in UKR is increasing and is expected to give better results in the future.
Keywords: Unicompartmental knee replacement, Indian joint registry, National joint registry, Australian Orthopaedic Association National Joint Replacement Registry, Swedish knee arthroplasty register.
Unicompartmental knee replacement (UKR) gives good to excellent functional outcomes and improved knee scores [1]. Studies have reported excellent survivorship and better knee kinematics, following this procedure [1, 2]. Burn et al. in his study in 2018 concluded that UKR is a highly successful and cost-effective treatment option for medial compartment osteoarthritis of the knee. Unicompartmental knee continues to contribute 10–15% of the total replacement surgeries worldwide as per registry data, with an increasing trend. The trends in the National joint registry of England, Wales, Northern Ireland, and the Isle of Man (NJR) suggest a steady growth in the total percentage of patients receiving UKA compared to the total number of patients receiving joint replacements from 8.5% in 2004 to 11.1% in 2018 [3]. In Australia and Sweden, the trend was in a declining phase up until 2014 [4, 5]; however, there has been a constant increase in numbers since then, with AOANJR reporting 5.8% of total joints in 2019 compared to 4.4% in 2014 [3]. According to the Swedish knee arthroplasty registry, UKR accounted for almost 11% of total joints operated in 2019 [5]. UKR attracts the surgeon community worldwide for its bone preservation, as evidenced by its increasing trends in various joint registries all over the world [1]. However, most joint registries consider early revision to be one of the common complications observed. It has been observed that converting UKR into total knee replacement (TKR) is not an easy task to perform and has a steep learning curve [2]. Malhotra et al. in his study concluded that unicompartmental knee arthroplasty along with newer instrumentation has improved the precision of component positioning and has improved the results [6]. AOANJR has reported lower revision rates while using robotics [3]. Authors wanted to look into UKR scenarios in India based on the Indian joint registry data, compare where we stand globally, and also the effect of robotics.
All UKR s registered with the Indian Joint Registry from 2016 to 2021 were included in the study. Retrospective analysis of demographic data, diagnosis leading to primary UKR, year-wise surgeon inclination toward UKR, implant preference, regions where UKR was preferred, and the effect of robotics in UKR was done. All the data from the Indian joint registry were compared to the registry data from the UK (NJR), Sweden (SKAR), Australia (AOJR), and the USA (AJRR).
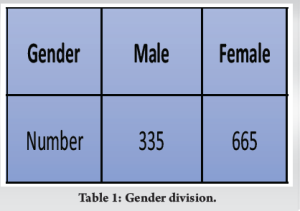
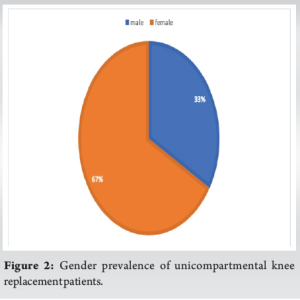
One thousand and eighty-six UKR s recorded in IJR from 2016 to 2022, 86 patients did not give consent to share details, of the others who gave consent, 335 were male and 665 were female (Table 1).
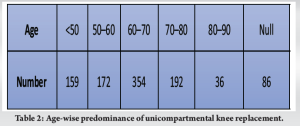
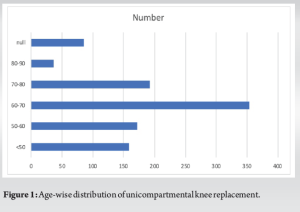
The mean age of the patients who underwent UKR was 62.44. A maximum of 354 patients were between the age group of 60 and 70 years, with 159 patients below 50 years,172 patients between 50 and 60 years,192 patients between 70 and 80 years, and 36 patients between 80 and 90 years (Table 2).
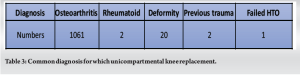
Osteoarthritis was the principal diagnosis for which UKR was done with 1061 cases followed by 20 cases for deformity and 2 for each rheumatoid and previous trauma (Table 3).
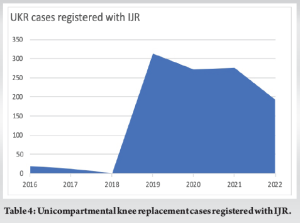
The use of UKR increased from 0.20% in 2017 to 2.85% of all knee procedures in 2020. There has been a gradual increase in the number of UKR for the past 5 years (Table 4).
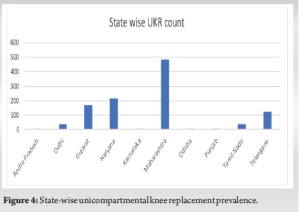
The cities where more unicompartmental knee is performed are in the order of Mumbai (32.78%), Faridabad (9.39%), Pune (7.92%), and Hyderabad (6.35%) (Table 5).
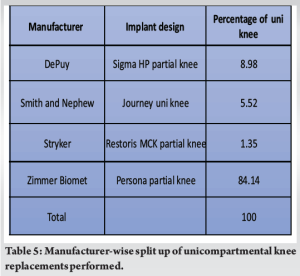
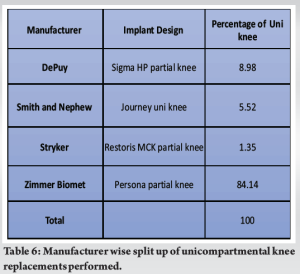
Zimmer Biomet’s persona partial knee is the most preferred iplant with 84.14% followed by Depuy’s Sigma HP partial knee (8.98%) (Table 6).
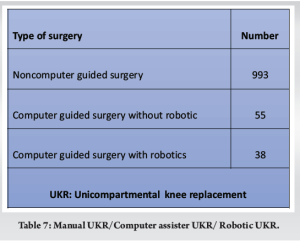
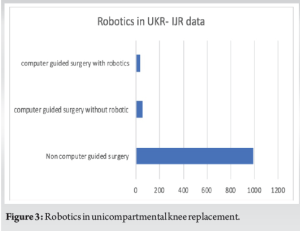
The proportion of UKRs using computer assistance is 93 cases out of 1086 surgeries, of which 38 utilized computer assistance (Table 7). However, the follow-up of these patients and how each group performed were not evaluated.
UKRs were practiced as a treatment option for medial compartment osteoarthritis even before total joint arthroplasty was introduced [1]. In the last 5 years, the proportion of UKRs has increased all over the world. This trend is reflected in the various joint registries across the world. The proportion of the increase in 2020 was 11.60% in the UK, 6.80% in Australia, 11.20% in Sweden, and 4.20% in the USA according to their respective joint registries [2,3,7]. India is a late enterant in making a centralized registry for joint replacement data. Indian Joint registry came into functioning with its launch in 2016 [1]. The first index case of UKR registered with IJR was done on December 19th, 2016 in the poilet study. Until now a total of 1086 UKRs have been reported in India whereas, the US registry has reported 61207 unicompartmental knees from 2012 to 2020, the National joint registry of the UK has reported 31306 UKR done from 2012 to 2020 [2], and Australia has reported 56628 cases until 2019 [7]. The numbers in India are less compared to the international data. IJR states that patients between the age group of 60 years and 70 years received UKR more compared to others. A similar pattern was observed in the National Joint registry of the UK, with the median age being 64 years, 6–12 years younger than the mean age for TKR. In Australia too, the average age group was 55–74 years with a mean age of 65.4 years. The primary diagnosis as an indication for UKR has been osteoarthritis globally and the same has been observed in India too with osteoarthritis of the knee being the primary diagnosis in almost 98% of the cases (Fig. 1 and 2).
In India, since the index case, the percentage of cases contributed by UKR, compared to all the knee replacements has increased and accounted for 2.85% in 2019, 1.67% in 2020, 1.58% in 2021, and 1.64% in 2022. Neglecting the impact of COVID-19, this is a slow but progressive increase in the numbers. When compared to the TKRs registered with IJR, this increase in the numbers can be considered insignificant. The number of total joint replacements has increased from 10988 in 2019 to 16308 in 2020 and 17440 in 2021, whereas the UKR numbers are 313 in 2019, 272 in 2020, and 276 in 2021 (Table 8). 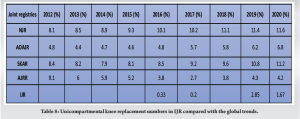
Kozinn and Scott proposed almost 47% of the patients suffering from medial compartment osteoarthritis are ideal candidates for unicompartmental knee arthroplasty (UKA). However, many surgeons prefer total joint replacement compared to UKR. The reason for this disparity may be due to a staggering three times the rate of revision, compared to TKR, as in accordance with contemporary reports from registers in other countries such as Sweden, Australia, and England and Wales [7]. The cumulative revision rate for primary UKR for Osteoarthritis is 7.9% at 5 years and 27.3% at 18 years [3]. These factors lead to surgeons preferring TKRs in place of UKR, even when indicated. A conservative estimate from previous studies suggests, at present 21% of patients undergoing TKR meet the criterion for UKR. If these 21% of the patients in NHS, currently undergoing TKR, underwent UKR instead, a potential annual savings of 169 deaths, at a cost of 405 additional revisions may result [5]. Many authors have suggested revision rates, although traditionally used, are not a suitable yardstick to compare different prosthesis. J.W. Goodfellow and D.W. Murray in their article “A critique of revision rate as an outcome measure” have said the higher revision rate of UKR was because it was easier and safer to revise than compared to TKR. Most revisions of UKR are conversion to primary TKR, whereas most revisions of TKR are more complex procedures requiring larger components and an increased level of constraint. In a study based on the NJR data between 2006 and 2010, James A. Kennedy, Hemant G. Pandit, David W. Murray et al suggested most UKR revisions can be avoided and inappropriate indications for primary and revision surgery are responsible for the high rates of revision seen in registries. As IJR data are limited only for a short duration, we were not able to study the revision pattern in India. The Australian Joint Registry has given cumulative percent revision for primary UKR for OA is 7.9% at 5 years and 27.3% at 18 years. Of the 866 revisions reported in 2019, most of them were revised to TKR (87.5%).(3) The reasons for revisions were commonly loosening (38.4%), progression of disease (33.5%), pain (8.1%), infection (4.8%), bearing dislocation (3.3%), fracture (2.8%), lysis (2.3%), instability (1.5%), wear tibial insert (1.5%), and malalignment (1.3%) [7]. Unicompartmental knee procedures using robotics assistance have a lower rate of revision between 9 months and 1.5 years, as per AAJR reports [7]. While using robotics, there was lower revision for loosening, progression of disease, fractures, and pain but more revisions for infections. The cumulative present revision of primary UKR since 2015 has been less by robotic assistance [6]. Malhotra et al. in his study, on newer instrumentation for unicondylar knee replacement, have said newer instrumentation improves patient satisfaction and component positioning, thereby the long-term outcomes are expected to improve [8] (Fig. 3).
In India, the proportion of knee replacements contributed by UKR is only 2–3% and only a few centers in India are offering UKR as a treatment option. More number of UKRs (479) are done in the western part of the country compared to the rest of India. The cities where more UKRs are performed are in increasing order of Mumbai (32.78%), Faridabad (9.39%), Pune (7.92%), and Hyderabad (6.35%). Maharastra alone, as a single state has contributed to almost 45% of the UKR cases done so far with 22 surgeons performing these surgeries (Fig. 4).
Some studies have suggested lesser revision rates with surgeons performing a higher volume of surgeries; yet, in our country except for selected pockets, most surgeons perform on an average of 1 or 2 cases per year [9]. This difference in the numbers is due to the surgeon’s preference and the surgeon’s experience with the procedure. For example, one of the successful high volume surgeons in Mumbai has told us that 50–60% of his practice is contributed by UKR. This is in accordance with Liddle et al., who in his study have concluded optimal results are achieved with UKR usage between 40% and 60% [10]. Since we can observe a growing trend in the patients undergoing UKR, it is safe to assume the majority of the patients had good outcomes following the procedure. Thus, it is safe to say, though UKR is a great tool in the armamentarium of a good surgeon, it is learning curve is steep, and better results are obtained only in trained hands.
- The percentage of knee replacements contributed by UKR, is increasing globally and the same trend can be observed in some selected pockets of India
- Persona partial knee(Zimmer Biomet) prosthesis is the most preferred UKR prosthesis
- The use of robotics in UKR is increasing and is expected to give better results in the future.
Although unicompartmental knee replacement numbers are limited compared TKRs currently, but in the near future, with more and more surgeons developing interest in this procedure, UKR will become a popular tool in the armamentarium of any knee surgeon.
References
- 1.Vaidya SV, Jogani AD, Pachore JA, Armstrong R, Vaidya CS. India joining the world of hip and knee registries: Present status-a leap forward. Indian J Orthop 2020;55 Suppl 1:46-55. [Google Scholar]
- 2.Ben-Shlomo Y, Blom A, Boulton C, Brittain R, Clark E, Craig R, et al. The National Joint Registry 16th Annual Report 2019. London: National Joint Registry; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559972 [Last accessed on 2022 Aug 27]. [Google Scholar]
- 3.Annual Report 2020-English Version-Svenska Knäprotesregistret. Available from: https://www.myknee.se/en/start/207-annual-report-2020-english-version [Last accessed on 2022 Aug 27]. [Google Scholar]
- 4.The National Joint Registry Annual Report; 2014. Available from: https://www.researchgate.net/publication/272504688_the_national_joint_registry_annual_report_2014 [Last accessed on 2022 Aug 21]. [Google Scholar]
- 5.Liddle AD, Judge A, Pandit H, Murray DW. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: A study of data from the National joint registry for England and Wales. Lancet 2014;384:1437-45. [Google Scholar]
- 6.Ofa SA, Ross BJ, Flick TR, Patel AH, Sherman WF. Robotic total knee arthroplasty vs conventional total knee arthroplasty: A nationwide database study. Arthroplast Today 2020;6:1001-8.e3. [Google Scholar]
- 7.2019-AOANJRR. Available from: https://aoanjrr.sahmri.com/annual-reports-2019 [Last accessed on 2022 Aug 27]. [Google Scholar]
- 8.Malhotra R, Kumar V, Wahal N, Clavé A, Kennedy JA, Murray DW, et al. New instrumentation improves patient satisfaction and component positioning for mobile-bearing medial unicompartmental knee replacement. Indian J Orthop 2019;53:289-96. [Google Scholar]
- 9.Wilson HA, Middleton R, Abram SG, Smith S, Alvand A, Jackson WF, et al. Patient relevant outcomes of unicompartmental versus total knee replacement: Systematic review and meta-analysis. BMJ 2019;364:1352. [Google Scholar]
- 10.Liddle AD, Pandit H, Judge A, Murray DW. Optimal usage of unicompartmental knee arthroplasty: A study of 41, 986 cases from the National joint registry for England and Wales. Bone Jt J 2015;97-B:1506-11. [Google Scholar]



