
This study investigated an innovative technique using K-nail reamers to safely extract a broken femoral nail fragment without opening the fracture site, demonstrating successful fragment removal and the potential to mitigate complications while achieving proper healing
Dr. Adnan Anwer, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.adnan.amu@gmail.com
Introduction: Intramedullary nail placement is a preferred method for femoral shaft fractures due to biomechanical advantages. Despite its simplicity and efficacy, complications, such as pseudoarthrosis and nail fracture, pose challenges. Removing the distal fragment presents a vexing issue, often requiring specialized instruments. Current retrograde techniques may not be universally accessible, potentially leading to non-union site opening and tissue damage. While intramedullary nailing benefits fracture treatment, addressing its removal complications is crucial for further advancements. In this case, universal zig and K-nail reamers are used to extract the broken nail.
Case Report: A 42-year-old male suffered an injury to his left thigh in a bike collision. Radiological examination revealed an oblique fracture in the proximal 1/3rd and distal 2/3rd junction of the left femur shaft. Closed reduction and internal fixation were initially performed, but delayed union occurred. Nine months post-surgery, a broken femoral nail and non-united fracture were observed. The patient underwent successful removal and replacement of the broken nail with a wider intramedullary nail. The procedure involved using a universal zig for removal of the proximal fragment and K-nail reamers to remove the distal fragment of the broken nail, and inserting a wider proximal femoral nail. The patient was discharged in satisfactory condition with tolerable weight-bearing.
Conclusion: Broken femoral nail presents a unique challenge to the operating surgeon. It requires diligent planning with appropriate instruments and techniques. There have been many techniques devised to tackle this problem and the use of K-nail reamers as described in this case is another innovative method in this regard.
Keywords: Broken femoral nail, vintage technique, K-nail reamer.
Intramedullary nail placement has emerged as the preferred treatment for femoral shaft fractures, offering notable biomechanical advantages over internal fixation with plates. With a consolidation rate of 97–100% [1], it is a technique praised for its simplicity and reproducibility, primarily employing a closed-focus insertion method to safeguard surrounding soft tissues. However, despite its merits, intramedullary nailing is not without complications, and one particularly vexing issue is pseudoarthrosis accompanied by nail fracture. This infrequent occurrence is attributed to the cyclic stress that synthetic intramedullary nails endure at the non-union focus. The real challenge arises when dealing with the removal of the distal fragment of these intramedullary nails. Most literature outlines retrograde techniques utilizing specialized instruments such as hooks, olive wires, or other tailored devices [2-4]. Unfortunately, these methods often necessitate specific materials that may not be readily accessible to general orthopedicians. Furthermore, the inherent difficulty in using these approaches may lead to the need for opening the non-union site or causing damage to the surrounding tissue. The extraction of broken distal segment femoral nails in the context of femoral fracture non-union is, undeniably, a procedure that demands careful consideration and the exploration of various methods. While intramedullary nailing offers remarkable benefits in fracture treatment, the complications associated with removal underscore the importance of continued research and the development of accessible solutions.
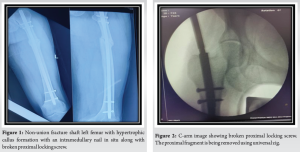
A 42Y/M came to emergency in 2020 with an injury to the left thigh when the bike he was riding collided with an oncoming bike. On examination, he had diffuse tenderness and swelling over his left thigh. On radiological examination, X-ray left thigh shows an oblique fracture shaft left femur junction of proximal 1/3rd and distal 2/3rd. The patient was managed by closed reduction and internal fixation with femur interlocking nail. The patient was followed up regularly and on serial X-rays, the fracture showed some signs of delayed union. Then, about 9 months from the day of surgery when the X-ray was done it showed a broken femoral nail with non-united fracture shaft femur (Fig. 1). For this, he was admitted and was planned for implant removal followed by internal fixation with a femoral interlocking nail.
Technique
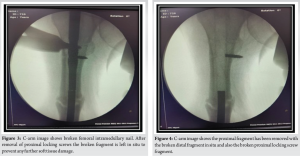
On a supine traction bed, two incisions are made over the subtrochanteric region and the greater trochanter over the original scars to allow the removal of the two locking screws.The distal locking screws were removed. After extraction of the proximal portion (Fig. 2), the distal portion was planned to be removed using ball tip wire but the wire did not pass through the broken nail and we were left with no option to proceed further. The proximal broken segment of the nail was removed using the zig of the nailing set (Fig. 3). In this case, the nail in situ was a MADURA cannulated IM 34 cm × 11 mm nail. The proximal locking screw was also broken and was left in situ (Fig. 4).
Traditional K-nail sets are still available at our institution, so the set was taken out and reamers of the K-nail (Fig. 5) were used to extract the distal portion of the broken nail. Then, a guide wire was inserted in the distal fragment under C-arm guidance and buried in the subchondral region at the distal end. Reamer was passed in the canal (Fig. 6) and the extent of press-fitting was assessed in the broken nail. Once, we were sure about the press fitting of the K-nail reamer, the reamer was hammered back to take the broken nail out along with the reamer. Then, K-nail reamers were used of size just above the internal diameter of the distal fragment. The distal fragment was pulled out with the K-nail reamer (Fig. 7-9). Then, a wider proximal femoral nail was inserted (Fig. 10) while reducing the fracture by closed manipulation under C-arm guidance. Proximal and distal locking was done. The patient was discharged under satisfactory condition with tolerable weight-bearing.
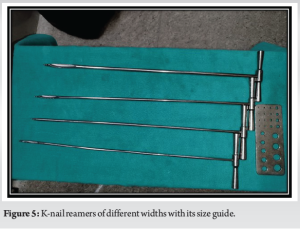



The extraction of the distal portion of a fractured femoral nail poses a challenge for orthopedic surgeons, and various surgical techniques have been previously outlined for this procedure. Franklin et al. [3] shared their experience treating 60 cases of broken femoral or tibial nails, extracting 20 distal fragments without additional surgical methods, and removing 28 nail fragments using long hooks resembling Ender pin extractors. Brewster et al. [4] and Hahn et al. [5] also advocated using long hooks for reamed nail removal but highlighted the risk of slipping, sticking, bending, or breaking inside the nail, causing complications. Giannoudis et al. [2] described a method involving special tools such as long graspers and hooks, utilizing long trephines, hooks, and auxiliary pins. While this technique is costly and labor-intensive, it serves as a viable alternative, particularly for fractures involving rigid and unreamed tibial pins. Levy et al. [6]. proposed a different approach, impacting a smaller-diameter nail into the distal fragment of a broken reamed femoral nail to ease local impaction and anterograde extraction. Middleton et al. [7] suggested filling the internal space of a reamed nail with guide wires for anterograde extraction of the distal fragment. Maini et al. [8] recommended passing an olive guide wire through the distal fragment of a reamed femoral nail and filling the nail with long Steinmann wires for removal. Marwan and Ibrahim [9] described passing a metallic wire through the middle of the fractured nail and its distal hole, securing it to the distal fragment through a small incision. Unreamed nails, increasingly used, particularly in polytrauma patients, pose different challenges. Hellemondt and Haeff [10] proposed a technique involving the extraction of the solid distal fragment of a tibial nail using a reamed nail with a larger diameter and the assistance of pins and long hooks. However, this method is not applicable when the fractured fragment matches the medullary canal’s diameter. Franklin et al. [3] mentioned using a long grasper-type instrument for removing distal fragments of broken solid nails but acknowledged its technical difficulty. Krettek et al. [11] detailed a technique for creating an opening near the fixation hole of the proximal screw, inserting a Hohmann-type lever to impel the fragment toward the fracture focus. Khan [12] described a method involving the opening of the non-union focus, resection of the bone flute, and traction with a hook for fractured nail removal. Gregory [13] proposed a different approach, extracting the distal fragment through a new incision in the pyriform fossa, creating an auxiliary opening in the femoral canal for clamping when specialized instruments are unavailable. These approaches are aggressive but necessary when appropriate instruments are not at hand. In our technique, K-nail reamers are used to extract the distal fragment. This novel use of K-nail reamers is unique and makes the procedure simple and efficient. The tips of K-nail reamers are tapered and the width comes in different sizes. Hence, these can be easily used to extract different types of cannulated nails. A major benefit is that this technique neither requires opening of the fracture site nor is there a requirement of any other incision. Hence, the operative time is significantly reduced and so is the risk of infection and other complications. A major disadvantage of this technique is that surgeons must have these different-sized K-nail reamers, and with the K-nails now being obsolete, these reamers are not usually available in every surgical setup.
A broken femoral nail presents a unique challenge to the operating surgeon. It requires diligent planning with appropriate instruments and techniques. There have been many techniques devised to tackle this problem and the use of K-nail reamers as described in this case is another innovative method in this regard.
Broken femoral nail presents as a challenging situation for orthopedic surgeons. Various techniques have been described to overcome this issue. In this case study, the distal fragment of the broken femoral nail was difficult to extract using guide wire. Instead of opening the fracture site, which would entail its own wide set of complication, the broken fragment could be removed using innovative approach with K-nail reamers.
References
- 1.Brumback RJ, Virkus WW. Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90. [Google Scholar]
- 2.Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury 2001;32:407-10. [Google Scholar]
- 3.Franklin JL, Winquist RA, Benirschke SK, Hansen ST Jr. Broken intramedullary nails. J Bone Joint Surg Am 1988;70:1463-71. [Google Scholar]
- 4.Brewster NT, Ashcroft GP, Scotland TR. Extraction of broken intramedullary nails--an improvement in technique. Injury 1995;26:286. [Google Scholar]
- 5.Hahn D, Bradbury N, Hartley R, Radford PJ. Intramedullary nail breakage in distal fractures of the tibia. Injury 1996;27:323-7. [Google Scholar]
- 6.Levy O, Amit Y, Velkes S, Horoszowski H. A simple method for removal of a fractured intramedullary nail. J Bone Joint Surg Br 1994;76:502. [Google Scholar]
- 7.Middleton RG, McNab IS, Hashemi-Nejad A, Noordeen MH. Multiple guide wire technique for removal of the short distal fragment of a fractured intramedullary nail. Injury 1995;26:531-2. [Google Scholar]
- 8.Maini L, Upadhyay A, Aggarwal A, Dhaon BK. A new method of removing a fractured interlocked nail. Injury 2002;33:261-2. [Google Scholar]
- 9.Marwan M, Ibrahim M. Simple method for retrieval of distal segment of the broken interlocking intramedullary nail. Injury 1999;30:333-5. [Google Scholar]
- 10.Hellemondt FJ, Haeff MJ. Removal of a broken solid intramedullary interlocking nail. A technical note. Acta Orthop Scand 1996;67:512. [Google Scholar]
- 11.Krettek C, Schandelmaier P, Tscherne H. Removal of a broken solid femoral nail: A simple push-out technique. A case report. J Bone Joint Surg Am 1997;79:247-51. [Google Scholar]
- 12.Khan FA. Retrieval of a broken intramedullary femoral nail. Injury 1992;23:129-30. [Google Scholar]
- 13.Gregory PR Jr. Removal of a broken solid-core intramedullary femoral nail using both antegrade and retrograde starting points. Orthopedics 1997;20:1087-9. [Google Scholar]








