
This article highlights the diagnostic workup and novel clinical presentation for intramuscular myxoma.
Dr. Keith T Aziz, Department of Orthopedic Surgery, Mayo Clinic Florida, Jacksonville, Florida. E-mail: nicolas.giusti@jax.ufl.edu
Introduction: Intramuscular myxomas are rare, benign mesenchymal tumors which commonly arise in muscle of the upper limb, pelvis, abdominal tissue, spine, or facial muscle. There are few case reports of intramuscular myxomas, and none of these describe intramuscular myxoma as a cause of compressive neuropathy.
Case Report: We describe the case of a 67-year-old woman who presented to us with a 1-year history of progressive enlargement of a painless right elbow mass. She gradually developed increasing numbness and tingling in her right small finger, which was worse at night. She underwent cubital tunnel release with concurrent right elbow mass excision of the flexor carpi ulnaris muscle. Histology showed intramuscular myxoma. Postoperatively, she had a complete resolution of her symptoms with a good functional outcome.
Conclusion: This is the first known case of intramuscular myxoma within the flexor carpi ulnaris causing compressive neuropathy of the ulnar nerve at the elbow.
Keywords: Intramuscular myxoma, ulnar neuropathy, compressive neuropathy, cubital tunnel, benign.
Intramuscular myxomas are rare, benign mesenchymal soft-tissue tumors that are believed to arise from fibroblasts which are unable to synthesize collagen fibers, leading to the creation of myxoid tissue [1]. They most commonly occur in women between the ages of 40 and 70 and usually present as a painless, slow-growing mass in the thigh or buttocks. Intramuscular myxomas have also been described in the upper limb, pelvis, abdominal wall, spine, or temporalis muscle [2, 3]. The occurrence of myxomas in muscle is rare and has an incidence of about 1:1,000,000 of population per year [4]. When imaged, myxomas usually do not appear on plain radiographs however computed tomography (CT) shows a well-defined, hypointense, homogenous mass without matrix. Magnetic resonance imaging (MRI) shows the signal as hypointense and homogenous on T1, and hyperintense and homogenous on T2 with moderate enhancement after injection of gadolinium [3]. Histologically, intramuscular myxomas are typically hypocellular, and hypovascular, and consist of an abundance of non-collagenous mucinous stroma. Despite having a seemingly encapsulated look and well-defined borders, the lesion microscopically infiltrates the muscle [5]. Cubital tunnel syndrome is the second most common peripheral nerve compression mononeuropathy after carpal tunnel syndrome, and the most common ulnar nerve compression neuropathy overall [6, 7]. In the general population, symptoms of cubital tunnel syndrome are estimated to appear in up to 5.9% of individuals, compared to 6.8% of those experiencing symptoms of carpal tunnel syndrome [7]. Symptoms typically develop following prolonged flexion through dynamic or static forces placed on the nerve (inflammatory, traumatic, iatrogenic, etc.) as it travels through the cubital tunnel [8, 9]. While there have been some case reports of masses such as ganglion cysts or giant cell tumors causing cubital tunnel syndrome, these reports are rare [6]. Cubital tunnel syndrome frequently presents with sensory deficits in the 4th and 5th digits, and motor changes often manifest as loss of pinch grip strength or dexterity due to diminishing intrinsic muscle function [8]. Cubital tunnel syndrome can be diagnosed clinically with provocative maneuvers such as a positive Tinel’s sign or symptoms with a flexion-compression test, and with the assistance of imaging studies such as ultrasound or electrodiagnostic studies [9]. Despite intramuscular myxomas being well documented and studied, to the author’s knowledge there are no reported cases of intramuscular myxomas causing cubital tunnel syndrome as a result of mass effect in the elbow or forearm. Here we report a case of a woman with a right elbow mass and symptoms of cubital tunnel syndrome who was formally diagnosed with intramuscular myxoma after mass excision and cubital tunnel release.
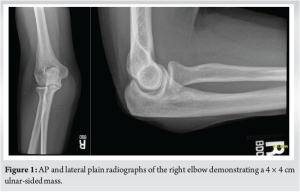
The patient is a 67-year-old left-hand-dominant female who presented to our institution in March 2023 for evaluation of a chronic right elbow mass. The patient first noticed the mass 8 months prior during a routine outpatient visit at an outside institution. She reported elbow swelling for approximately 1 year and sought orthopedic evaluation once she began experiencing numbness and tingling in an ulnar nerve distribution of her right hand. She denied any pain or weakness at that time. Plain radiographs and CT of the right elbow revealed a well-defined cyst-like mass measuring approximately 4 × 4 cm (Fig. 1).
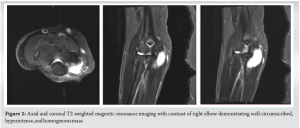
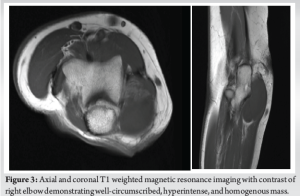
Upon initial evaluation at our institution, she described increasing pain and discomfort described as a “dullness” around the mass, specifically in the posterior medial aspect of her right elbow with radiation into her right fifth digit. She reported increased numbness during certain tasks such as driving. Interval enlargement of the mass was also reported, and she began waking up at night daily due to symptoms. No fevers, chills, weight loss, or intrinsic hand weakness were noted on her initial evaluation. Repeat radiographs and CT demonstrated no significant changes when compared to outside imaging. MRI with and without contrast was obtained which showed a predominantly cystic structure along the dorsal/ulnar aspect of the elbow with evidence of only thin peripheral enhancement with volar displacement of the traversing ulnar nerve, with no evidence of encasement (Fig. 2 and 3).
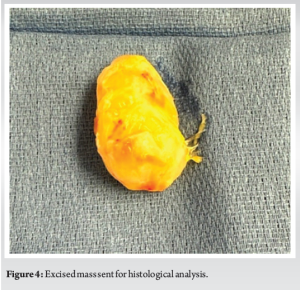
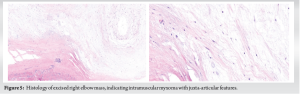
The patient was then referred to our hand and upper extremity service in April 2023. On examination, she had a mass about the medial elbow, a positive Tinel’s, and a flexion compression test at the elbow but normal motor examination findings. She was formally diagnosed with cubital tunnel syndrome and underwent in situ cubital tunnel decompression and mass excision in July 2023. A large firm mass approximately 4 × 5 cm was removed from deep to the fascia of the flexor carpi ulnaris which was causing a mass effect on the ulnar nerve and surrounding muscle (Fig. 4). The mass was sent for histologic analysis which showed intramuscular myxoma with features of juxta-articular myxoma (Fig. 5). Postoperatively there were no complications and she has had complete resolution of her symptoms.
We present a case of a 67-year-old left-hand dominant female who presents 8 months after noticing a mass on her right elbow which expanded in size and caused numbness and tingling in her right small finger. She was subsequently diagnosed with cubital tunnel syndrome and during cubital tunnel release the mass was excised and found to be an intramuscular myxoma on histologic evaluation. This offers several intriguing points of discussion. Intramuscular myxoma is a rare tumor with an incidence of about 1:1,000,000 [4]. To our knowledge, this is the first case report of intramuscular myxoma causing mass effect at the elbow resulting in cubital tunnel syndrome. There has been one prior case report by Valer et al. which describes a case of intramuscular myxoma causing paralysis of the posterior interosseous nerve (PIN) [10]. The patient presented with a 5-month history of inability to extend the digits of their right hand. The electromyogram demonstrated findings consistent with a right PIN neuropathy. During surgical release, a mass was found to be constricting the deep radial nerve at the level of the arcade of Frohse. The mass was removed and a histologic examination showed an intramuscular myxoma. The patient subsequently had a return of function 12 months after surgery. Primohamadi et al. describe a case of intramuscular myxoma within the anterior forearm. The patient they described had symptoms of pain as a result of the mass however did not have any symptoms of compressive neuropathy secondary to the mass [1]. Our experience mirrors that of Primohamadi et al. in that removal is associated with a good prognosis. Furthermore, our case demonstrates alleviation of the compressive neuropathy secondary to the surrounding mass effect of the tumor. Nisi et al. describe an example of intramuscular myxoma within the buccal mucosa [11]. The patient had pain surrounding the mass however did not exhibit any symptoms of neuropathy or limitations in motor function of the peri-oral region. The patient underwent mass excision and subsequently experienced improvement of symptoms similar to other cases presented in literature including the patient presented in this study. Although there are no known studies of intramuscular myxoma causing cubital tunnel syndrome, there are studies and case reports which describe cubital tunnel syndrome being caused by the mass effect of ganglion cysts, hemangiomas thromboses, tendon sheath tumors, or other tumors/masses. In a study by Chang et al., they discuss intraneural ganglions as a cause of cubital tunnel syndrome. Intraneural ganglions are rare cysts that originate within the epineurium of peripheral nerves [6]. The incidence of ganglion cyst causing cubital tunnel was found to be 3–8%, however, occasional reports describe the incidence as rarer. There is no mention however of intramuscular myxoma as a cause of cubital tunnel. Despite intramuscular myxoma being identified as a rare tumor in isolation, it has been associated with being a part of McCune–Albright syndrome and Mazabraud syndrome which are caused by mutations in the GNAS gene [12]. If patients are diagnosed with intramuscular myxoma it could be considered to screen patients for other tumors or conditions including GNAS gene mutations. While our patient had none of the typical features of McCune-Albright or Mazabraud, our experience that intramuscular myxomas may cause compressive neuropathy should encourage clinicians caring for patients with McCune-Albright or Mazabraud to carefully screen for compressive neuropathy during routine follow-up.
Intramuscular myxoma is a rare mesenchymal tumor which can occur in multiple different locations. Despite multiple case reports describing upper extremity intramuscular myxomas, there have been none which describe them as causing compressive neuropathy. We present a case of a 67-year-old woman with intramuscular myxoma within the flexor carpi ulnaris causing compressive neuropathy of the ulnar nerve at the elbow, who had complete resolution of her symptoms with surgical excision.
This case highlights a novel presentation of intramuscular myxomas, as it is the first case of compressive neuropathy secondary to intramuscular myxoma in the upper extremities. It also demonstrates the importance of adherence to fundamental soft-tissue tumor principles for surgical management to decrease the likelihood of recurrent compressive neuropathy.
References
- 1.Primohamadi H, Begloo MJ, Rahimi M, Akbaribazm M. Rare forearm intramuscular myxoma: A case report. Clin Case Rep 2023;11:e7467. [Google Scholar]
- 2.Sukpanichyingyong S, Matsumoto S, Ae K, Tanizawa T, Hayakawa K, Funauchi Y, et al. Surgical treatment of intramuscular myxoma. Indian J Orhtop 2021;55:892-7. [Google Scholar]
- 3.Prado MA, Miro RL, Leal IM, Vargas J, Dorrego EJ. Intramuscular myxoma: Differential diagnosis and review of the literature. Orthopedics 2013;25:1297-9. [Google Scholar]
- 4.Hashimoto H, Tsuneyoshi M, Daimaru Y, Enjoji M, Shinohara N. Intramuscular myxoma. A clinicopathologic, immunohistochemical, and electron microscopic study. Cancer 1986;58:740-7. [Google Scholar]
- 5.Yaligod V, Ajoy S. Intramuscular myxoma - A rare tumor. J Orthop Case Rep 2013;3:38-41. [Google Scholar]
- 6.Chang WK, Li YP, Zhang DF, Liang BS. The cubital tunnel syndrome caused by the intraneural or extraneural ganglion cysts: Case report and review of the literature. J Plast Reconstr Aesthet Surg 2017;70:1404-8. [Google Scholar]
- 7.Anderson D, Woods B, Abubakar T, Koontz C, Li N, Hasoon J, et al. A comprehensive review of cubital tunnel syndrome. Orthop Rev (Pavia) 2022;14:38239. [Google Scholar]
- 8.Burahee AS, Sanders AD, Shirley C, Power DM. Cubital tunnel syndrome. EFORT Open Rev 2021;6:743-50. [Google Scholar]
- 9.Palmer BA, Hughers TB. Cubital tunnel syndrome. J Hand Surg Am 2010;35:153-63. [Google Scholar]
- 10.Valer A, Carrera L, Ramirez G. Myxoma causing paralysis of the posterior interosseous nerve. Acta Orthop Belg 1993;59:423-5. [Google Scholar]
- 11.Nisi M, Izzetti R, Gabrielle M, Pucci A. Oral intramuscular myxoma: Case report and brief review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol 2020;131:e52-8. [Google Scholar]
- 12.Manoharan SR, Shaw AB, Arnold CA, Farhadi HF. Infiltrative intramuscular myxoma of the cervical spine: A case report. J Spine 2015;15:e1-4. [Google Scholar]





