
This article describes an injury which can easily be misdiagnosed as initially we had done as well. Management of these injuries needs to be planned out well.
Dr. Parth Parasnis, Department of Orthopaedics, MGM Medical College, Navi Mumbai, Maharashtra, India. E-mail: parasnisparth2@gmail.com
Introduction: Hip dislocations are mainly high-energy injuries which generally occur posteriorly. The anterior dislocations of the hip are rare and this dislocation coupled with a neck of femur fracture is very less likely. .
Case Report: This article presents a rare and challenging case of a 43-year-old chronic alcoholic man with an anterior hip dislocation and ipsilateral neck of femur fracture. The patient’s history revealed a seemingly trivial domestic fall, but on examination, he exhibited severe pain, limb shortening, and external rotation in the left hip joint. Radiographic assessments initially suggested a posterior femoral head dislocation, but a subsequent computed tomography scan revealed an unusual scenario – the fractured femoral head had displaced anteriorly, traversing over the iliac wing, and settling in the pelvic cavity. Discussion of this unique case explores the infrequent association of anterior traumatic hip dislocations with femoral neck fractures. Prognosis in such cases is generally poor, with considerations for factors such as time to surgery, surgical findings, and patient age playing a crucial role in determining the optimal treatment strategy. The article delves into the challenges posed by the presented case, emphasizing the importance of appropriate diagnosis and surgical planning in managing these complex injuries.
Conclusion: The rarity of the presented injury, coupled with the unexpected clinical course following surgery, underscores the importance of maintaining a high index of suspicion for unusual presentations, even in seemingly minor traumas. This article contributes valuable insights into the diagnosis, surgical management, and challenges associated with the rare combination of anterior hip dislocation and ipsilateral neck of femur fracture.
Keywords: Neck of femur fracture, anterior hip dislocation, Girdlestone excision arthroplasty
Hip dislocations are typically high-energy injuries, most commonly occurring posteriorly (90%), typically with axial load on the femur with hip flexed and adducted. They are commonly associated with posterior acetabular wall fractures, femoral head fractures (5–15%) [1-3], and ipsilateral knee injuries, then known as complex fracture-dislocations of the hip, requiring early diagnosis and surgical intervention. Delayed complications include avascular necrosis and secondary osteoarthrosis resulting in significant morbidity [4,5]. Anterior hip dislocations are caused by forcible abduction, where in this position, the neck or trochanter impinges on the rim of the acetabulum and forces the femoral head forward through the anterior capsule. In a concomitant position of hip flexion, an obturator-type dislocation may occur whereas in an extended hip, pubic type results. If the force is not dissipated, then it causes a complete break in the continuity of the neck [6,7]. Traumatic dislocation of hip with ipsilateral femoral neck fracture in the absence of an acetabular fracture is a rare and challenging injury with only a few cases is reported in literature. Prosthetic replacement and surgical fixation are the two main methods of surgical management in this case. However, due to the paucity of such cases in literature, it yet remains ambiguous as to which is better [4,5]. There have been reports of neck of femur fracture associated with hip dislocations (anterior or posterior) in which the head of femur has been displaced [8, 9]. Here, we describe a case of anterior hip dislocation with ipsilateral neck of femur fracture with the fractured head displaced anteriorly passing over the iliac wing and lying in the pelvic cavity.
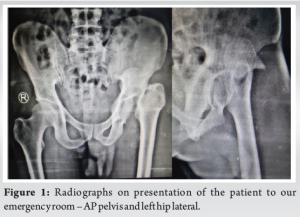
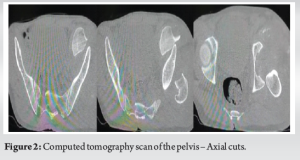
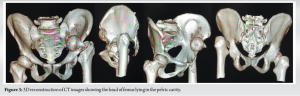
A 43-year-old chronic alcoholic man presented to our orthopedic emergency department with an alleged history of trivial trauma – domestic fall – which he sustained 10 days ago after which he was able to ambulate with support and pain. Since 1 day, he had been having severe pain at the left hip joint which was radiating to the groin. He also presented with 2 cm shortening of the left lower limb which was externally rotated. After initial stabilization, the patient was taken for radiographs of the pelvis with both hips anteroposterior and cross table lateral views. The patient was diagnosed with a left-sided neck of femur fracture with a femoral head dislocation which appeared to be posterior. However, the head was not palpable in the gluteal region and the patient was taken for a computed tomography (CT) scan of the pelvis. The CT demonstrated a neck of femur fracture with an intact pelvis and acetabulum however with the head of the femur lying anteriorly in the pelvic cavity retroperitoneally. The patient underwent a contrast-enhanced CT scan to rule out any missed injury to the pelvis or visceral organs. All vital structures were intact and the patient was shifted to the minor theater and underwent a proximal tibial skeletal traction pin insertion and was shifted to the ward with 7 kg of weight applied as traction (Fig. 1-3).
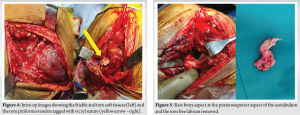
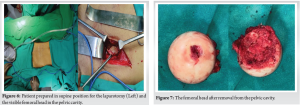
The patient was worked up for preanesthetic fitness for surgery and was incidentally found to have hemoglobin level of 6 mg/dL. The patient was transfused and fitness for surgery was given. The patient was planned for an uncemented total hip replacement with the backup of a constrained lip liner. The patient was unable to afford a dual mobility cup. An opinion was taken of the Department of General Surgery and a combined surgical plan was formed. The patient was to be taken up for a standard laparotomy and the head of the femur would be removed by careful dissection and reflection of the peritoneum followed by a standard posterior Southern-Moores approach to the hip for the total hip replacement. The patient was taken up for surgery and with the patient in supine position a 6 cm laparotomy incision was taken at the left flank just medial to the anterior superior iliac spine and the soft tissue was dissected. The peritoneum was reflected medially to reveal the fractured femoral head which was removed with the help of a curved osteotome. Behind the head was a few fibers of the hip joint capsule. The incision was closed over a negative pressure drain and the patient was repositioned into a lateral decubitus and re-draped for the THR. The standard posterior approach incision was taken 15 cm in length and gluteus maximus muscle and tensor fascia lata were split. After reflecting the trochanteric bursa, we found the torn Piriformis; short external rotators (superior and inferior gemelli along with the obturator internus tendon) and Gluteus Medius muscle. The acetabulum labrum was avulsed from the superior portion of the acetabulum and lay free in the acetabulum which was removed. There appeared to be an defect at the superolateral aspect of the acetabulum. There were torn fibers of the hip capsule visualized. The patient desaturated intraoperative and became unstable. The oxygen saturation fell to 84%. The procedure was abandoned and the patient was left with a Girdlestone excision arthroplasty and skeletal traction was reapplied. Postoperatively, the patient was kept in the high-dependency unit for 2 days but was shifted back to the normal ward once he stabilized and was maintaining oxygen saturation without any supports. Pulmonary embolism, deep vein thrombosis, and respiratory causes were ruled out. The anesthetic team along with the psychiatric team suspected severe alcohol withdrawal as one of the probable causes. The patient had however refused further operative treatment and a psychiatric opinion was taken and was diagnosed with alcohol withdrawal syndrome. The patient was kept on skeletal traction with a proximal tibial pin for 6 weeks. The patients and relatives were counseled regarding the need for a total hip arthroplasty in the near future and to return once the patient recovers. The patient presented 6 months later with a successful total hip replacement done elsewhere at a rural center. No details of the surgery were available. The patient claimed that he had an abduction pillow in between his legs for 6 weeks and was kept nil weight-bearing for the same duration after which gradual weight-bearing was allowed. A radiograph of the left hip was taken showing a stable total hip replacement implant in situ (Fig. 4-7).
Reports of anterior traumatic hip dislocations are uncommon, and their association with fractures of the femoral neck is even more infrequent; only a few cases have been reported [10,11]. In a review study that analyzed hip dislocations with femoral neck fractures in 30 patients, only eight were found to be anterior [12]. The mechanism of injury is usually a high-energy trauma and an externally rotated lower extremity in abduction. Depending on the degree of hip flexion, the superior or inferior (obturator) dislocation takes place. In case of femoral head dislocation, a continuing force will result in complete break of the femoral neck, thus displacing the fragments and compromising the vascular supply of the femoral head [13]. Strangely, in our case, the patient gave an alleged history of trivial trauma – a domestic fall, after which he was able to ambulate for 10 days. Prognosis in cases of anterior hip dislocation with femoral neck fractures is poor. In 8 such patients who were initially treated with open reduction internal fixation, avascular necrosis developed [12]. Some of the factors to be taken into consideration while choosing the treatment for a patient are as follows – time to surgery, surgical findings, technique used to reduce, and fix the fracture and patient’s age. In adults or middle-aged patients, we would prefer to preserve the hip joint unless a clear predictable bad prognosis is suspected (increased time to surgery and loss of viability of the head). Here, the main goals are to preserve femoral head, avoid avascular necrosis and non-union [9]. Sendtner et al. [14] stated that osteosynthesis with preservation of the head of femur is an emergency procedure that needs to be performed within 6 h. The pressure resulting from bleeding within the articular capsule will increase after this point in time. Manninger et al. [15] reviewed 494 cases retrospectively with fracture neck femur who were treated by open reduction and internal fixation and categorized the timing of surgery into three groups: those who were operated on in the first 6 h, between 6 and 24 h and after 24 h. There was a significant difference between the first group and the other groups in the incidence of non-union and femoral head collapse with better results in the first group and with no difference in the incidence of complications between the second and third groups. In older patients with changes of hip osteoarthritis, total hip arthroplasty is the first choice of treatment [13]. In the case of anterior hip dislocation with ipsilateral basicervical fracture reported by Sadler and DiStefano, fracture was reduced and fixed with a hip screw and plate. The patient eventually developed avascular necrosis which was treated with muscle pedicle grafting [7]. McClelland reported a case with dislocation of the obturator type with ipsilateral femoral head and neck fracture, which was treated with a collarless press-fit bipolar prosthesis. Dümmer and Sanzana reported a similar case which was treated by an uncemented total hip arthroplasty [16,17]. Recently, with the advances in technology and implants available for a total hip replacement, there can be an argument to use a dual mobility system or a constrained liner due to the unavailability of the external rotators and a high risk of dislocation of the freshly implanted total hip replacement system. Newer 3D printing methods can be used in the management of this case as this would allow us to appreciate the bony anatomy to be dealt with intraoperative. In our case, not only was the interval between trauma and operation about 15 days, but the head had also skipped over the ilium and was lying in the pelvic cavity for that duration due to which the head was nearly certain to be unviable, and hence, osteosynthesis was not considered and a total hip replacement was the initial plan of surgery. The rarity of finding this presentation with such a trivial injury is what makes this case an interesting presentation and should be kept in the mind as a possible diagnosis of a treating surgeon (Fig. 8, 9).


Neck of femur fractures is common orthopedic injuries, whereas anterior dislocation of the head of the femur is a rare injury. A combination of both with the traversing of the head of the femur with the hip capsule fibers into the pelvic cavity is unheard of. Appropriate diagnosis, planning, and a multidisciplinary approach may be required to manage such cases.
Diagnosing and treating a neck of femur fracture with a an anterior hip dislocation where the head is in the pelvic cavity is a difficult condition to manage and should be treated with proper planning and execution of the surgery. A good knowledge of the available inventory and implant options will also come in handy.
References
- 1.Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res 2000;377:44-56. [Google Scholar]
- 2.Yang RS, Tsuang YH, Hang YS, Liu TK. Traumatic dislocation of the hip. Clin Orthop Relat Res 1991;265:218-27. [Google Scholar]
- 3.McKee MD, Garay ME, Schemitsch EH, Kreder HJ, Stephen DJ. Irreducible fracture-dislocation of the hip: A severe injury with a poor prognosis. J Orthop Trauma 1998;12:223-9. [Google Scholar]
- 4.Pipkin G. Treatment of Grade IV Fracture-dislocation of the hip a review. The J Bone Joint Surg Am 1957;39:1027-97 passim. [Google Scholar]
- 5.Stewart MJ, Milford LW. Fracture-dislocation of the hip. An end-result study. J Bone Joint Surg Am 1954;36:315-42. [Google Scholar]
- 6.Epstein HC, Harvey JP Jr. Traumatic anterior dislocation of the hip: Management and results (an analysis of fifty-five cases). J Bone Joint Surg Am 1972;54:1561-62. [Google Scholar]
- 7.Sadler AH, DiStefano M. Anterior dislocation of the hip with ipsilateral basicervical fracture. A case report. J Bone Joint Surg Am 1985;67:326-9. [Google Scholar]
- 8.Trikha V, Goyal T, Jha RK. Posterior dislocation of the hip with ipsilateral displaced femoral neck fracture. Chin J Traumatol 2011;14:104-6. [Google Scholar]
- 9.El Masry AM. Anterior hip dislocation with ipsilateral displaced fracture neck of femur treated by open reduction and internal fixation: Case report and review of the literature. Strategies Traum Limb Reconstr 2017;12:205-10. [Google Scholar]
- 10.Satadal N, Chawhan V, Bansal V, Lal Anupam. Anterior dislocation of hip with fracture neck femur with migration of head into pelvic cavity-A case report. Indian J Orthop Volume 39, Number 3, 2005, pp. 189-190. [Google Scholar]
- 11.Esenyaka I, Gorgec M. Traumatic anterior dislocation of the hip associated with ipsilateral femoral neck fracture: A case Report. Acta Orthop Traumatol Turc 2002;36:366-8. [Google Scholar]
- 12.Tannast M, Mack PW, Klaeser B, Siebenrock KA. Hip dislocation and femoral neck fracture: Decision-making for head preservation. Injury 2009;40:1118-24. [Google Scholar]
- 13.Morales J, Fernández-Valencia JA, Ríos M, Poggio D, Bori G, Riba J. Simultaneous femoral neck fracture and anterior hip dislocation: A case report. Int J Adv J Reconstr 2014;1:1-3. [Google Scholar]
- 14.Sendtner E, Renkawitz T, Kramny P, Wenzl M, Grifka J. Fractured neck of femur--internal fixation versus arthroplasty. Dtsch Arztebl Int 2010;107:401-7. [Google Scholar]
- 15.Manninger J, Kazar G, Fekete G, Frenyo S, Gyarfas F, Salacz T, et al. Significance of urgent (within 6h) internal fixation in the management of fractures of the neck of the femur. Injury 1989;20:101-5. [Google Scholar]
- 16.Thuan VL, Swiontkowski MF. Management of femoral neck fractures in young adults. Indian J Orthop 2008;42:3-12. [Google Scholar]
- 17.Dümmer RE, Sanzana ES. Hip dislocations associated with ipsilateral femoral neck fracture. Int Orthop 1999;23:353-54. [Google Scholar]







