
Diagnosis and treatment of a pelvic rib keeping in mind all the differential diagnosis.
Dr. Bibhudutta Malla, Department of Orthopaedic Oncology, Apollo Cancer Centres, Jubilee Hills, Hyderabad, Telangana, India. E-mail: bibhuduttamall_013@live.com
Abstract
Introduction: A elvic rib or pelvic finger is a benign and unusual congenital entity of hip with a finger or rib like bone formation in soft tissues around pelvis. It is generally asymptomatic and incidentally discovered in a plain radiograph. This is a very rare but not unknown entity.
Case Report: A 25-year-old male reported to our institution with dull aching pain over right hip and abduction gait, then followed up the radiograph and magnetic resonance imaging, in which there was a osteochondroma like lesion in medial aspect of lesser trochanter of right proximal femur was seen. Surgical excision of the lesion was done and sent for histopathological study in which pelvic rib was confirmed.
Conclusion: The real challenge is diagnosis of this condition with its differentials i.e. heterotrophic ossifications around hip, osteochondroma, post-traumatic ossification, or avulsion injuries in and around hip joint This entity should be in mind of radiologists, orthopedic surgeons, and orthopedic onco-surgeons for differential diagnosis of chronic hip pain to avoid unnecessary investigations and procedures.
Keywords: Pelvic rib, hip pain, pelvic finger.
Pelvic rib a.k.a pelvic finger most commonly found on iliac bone, it may be associated with one or more pseudo-articulations. This rare anomaly but it is benign in nature and usually asymptomatic so we detect it incidentally in major cases. It has no pathological significance but it may manifest as a dull aching pain or shooting type of pain around groin or lower back. Plain radiographs show a bony structure with a clear cortex and medulla arising from pelvis similar to a rib or a finger. Radiologists, orthopedic surgeons and orthopedic onco-surgeons should be aware with their typical and atypical forms and important features to achieve appropriate diagnosis. Establishment of correct diagnosis will help us in proper management and improve life style of symptomatic patients.
A 25-year-old male, who was a student as profession presented with dull aching pain in right groin region for 6 months. The pain was insidious in onset, gradually progressive, non-radiating associated with abduction gait and restriction of hip movements, aggravated by walking, squatting and relieved by rest and medications. No H/O trauma or any type of injury to groin.

On physical examination, skin was normal with no scars, sinus and no abnormal swelling present around the medial aspect of right groin region. There was palpable mass felt at right perineal region. There was restriction of movements with adduction of right hip limited to 20°, external rotation to 25°, internal rotation to 10° and 5° of hip extension. Patient had abduction gait. Muscle wasting of right thigh was about 2 cm. However, there was no restriction of movement and muscle wasting at left hip. Blood investigations including complete blood picture, serum calcium, phosphate, serum parathyroid, and alkaline phosphatase was within normal limits.
Radiograph (Fig. 1) was showing a bony protuberance arising from right ischium to right lesser trochanter, measuring few centimeters with no signs of joint degeneration. Suspecting it as an osteochondroma, we performed magnetic resonance imaging (MRI) and computed tomography (CT) scan (Fig. 2 and 3).

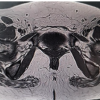
MRI report (Fig. 4) said that there was a large bone formation extending from right lesser Trochanter to the ischial tuberosity measuring 5.2 × 2.0 cm with surrounding edema. However, there was no cartilage cap which was differentiating from osteochondroma. With these investigations, we could establish a provisional diagnosis of pelvic rib instead of osteochondroma.

He was treated medically with NSAIDs and anti-inflammatory medications, but there was no symptomatic relief. Hence, surgical excision of the pelvic rib was planned with proper written consent of the patient.
Under C-arm guidance in radiolucent table, patient was placed in lithotomy position (Fig. 5), 5 cm incision given on medial aspect of thigh (Fig. 6) after proper surgical marking though C-arm guidance. We went in though hip adductor muscle intervals and reached lesser trochanter. From lesser trochanter we traced the pelvic rib and thoroughly excised the pelvic rib (Fig. 7) and then sent to histopathology.
Histopathology (Fig. 8) -Microscopic description showed bony tissue with outer cortical bone and central medullary bone having bony trabeculae. Marrow spaces show adipose tissue. The outer cortical bone is covered by fibrous periosteum with no cartilage cap and no evidence of malignancy. Features consistent with normal bony tissue. Corelating with imaging findings, features are consistent with pelvic rib.
The pain gradually decreased post-surgery, and after 1-year follow-up, he was asymptomatic, with improvement in all range of movements of hip and there is no signs of recurrence in 1-year follow-up.
In orthopedic literature, few cases of pelvic rib or pelvic digit have been reported. The pelvic finger is a benign lesion of bone development in which bone forms in the soft tissues adjacent to normal skeletal bone [1]. This lesion was reported in 1974 by Sullivan and Cornwell [2] in a 15-year-old girl child. This lesion can be located at any level of pelvic bone, ribs, and sometimes in anterior abdominal wall. It may or may not form pseudo articulation with axial skeleton [3,4]. Histologically, it is similar to a rib which has a normal medullary cavity surrounded by well-formed cortex [3,4]. Although, there was no clear picture about its etiology, These authors hypothesized during First 6 weeks of embryonic development, where the primordial costal cartilage of the first coccygeal vertebrae does not fuse as it should, a rudimentary rib is then formed in adjacent soft tissues, in which the segmentation of these cartilaginous centers gives the appearance of ‘phalanx’ [5] of finger so described as “the eleventh finger” [4]. Later few other authors hypothesized that it could have been arisen from displacement of rib or ossification center of anterior superior iliac spine. Recently, it is believed to be a failure of mesenchymal apoptosis for the anterior and lateral costal process. In the 3rd week of embryological development cells of mesoderm [6] capable of bone formation migrate through the cloacal membrane to the coccygeal region, that is, the future coccyx, pelvis, and abdominal wall. Normally, in development of a rib, the posterior zone creates costal process attaching the vertebral body, but in pelvis due to apoptosis the costal process mesenchyme degenerates. This failure of apoptosis would make the formation of bone possible in these areas, developing a shape of a rib. The most common location is soft tissues near to iliac bone or the hip joint. However, it can be located around the sacrum, coccyx, pubic symphysis, even abdominal wall [7]. Usually it is single and unilateral, but some cases of bilateral and multiple pelvic finger have been reported [5-12]. Majority of the cases are asymptomatic and this is an incidental finding [8]. But there are few reported cases who presented with lower back pain, chronic hip pain with difficulty in walking or restriction of movements around hip joint [3,4]. In radiograph, it appears as a linear bone structure similar to rib or phalanx with a well-defined cortex and a medullary cavity. CT is the imaging of choice for confirming the lesion, as it clearly identifies cortex and marrow and also implies relationship of lesion to adjacent bony structures [1,8,10]. MRI is helpful in symptomatic patients as it can demonstrate marrow edema in the pelvic finger and in pseudo articulation as it reported in few cases in literature. MRI can also give a soft tissue and neurovascular relationship around the benign lesion [1,8,9]. Differential diagnosis of pelvic rib comprises osteochondroma, myositis ossificans or heterotrophic bone formation, fong disease (Nail-patella Syndrome) [11], post-traumatic calcifications, and bony avulsion fractures of pelvis [9]. Osteochondroma has a cartilaginous cap and is continuous with underlying bone. Myositis ossificans and heterotrophic ossification is related to history of trauma and radiological examination will show heterogenous density without well corticated structure. Finally, fongs disease is a rare autosomal dominant disease, with nail and skeletal abnormalities, where we come across bilateral “Iliac horns” which is pathognomic for the disease [2,10].
This case was rare symptomatic case with gross restriction of movements of hip, as majority of reported cases were asymptomatic or an incidental finding where surgery was not an indication, so surgical excision of the lesion was needed for this case. Hence, the pelvic digit is a rare unusual congenital benign bony entity which has rib a-like histopathological picture is important for orthopedic surgeons, orthopedic onco-surgeons and radiologist to identify and diagnose the condition carefully. Symptomatology should be adequately correlated and differentiated from other conditions in order to avoid unnecessary surgical intervention or procedures.
As pelvic rib is rare and benign entity which is generally asymptomatic but symptomatic in few cases. Pelvic rib will be very confusing when it comes to confirmation of the diagnosis because of various differential which can mimic the lesion. MRI finding of the lesion without cartilaginous cap can be indication in the diagnosis of the lesion. As it is a benign lesion (osteochondroma like lesion) biopsy before excision may not be required which is generally followed in bone lesions. Excision followed by histopathology study will be helpful for confirmation of this rare entity. This lesion should be kept in mind when radiologists, orthopedic surgeons and orthopedic oncosurgeons come across lesions around hip with chronic hip pain.
References
- 1.Nguyen VD, Matthes JD, Wunderlich CC. The pelvic digit: CT correlation and review of the literature. Comput Med Imaging Graph 1990;14:127-31. [Google Scholar | PubMed]
- 2.Sullivan D, Cornwell WS. Pelvic rib. Report of a case. Radiology 1974;110:355-7. [Google Scholar | PubMed]
- 3.Khatri K, Goyal D, Paul R, Sandhu HS. Two pelvic digits on same side: Double trouble? J Clin Diagn Res 2015;9:RD04-5. [Google Scholar | PubMed]
- 4.Pandey V, Thakur AS, Acharya KK, Rao PS. The pelvic digit “eleventh finger”. Indian J Orthop 2009;43:97-8. [Google Scholar | PubMed]
- 5.Bouzaïdi K, Daghfous A, Chahbani H, Bouassida M, Jabnoun F, Rezgui Marhoul L. Pelvic digit: A rare lesion. Diagn Interv Imaging 2014;95:1117-20. [Google Scholar | PubMed]
- 6.Maegele M. Pelvic digit as a rare cause of chronic hip pain and functional impairment: A case report and review of the literature. J Med Case Rep 2009;3:139. [Google Scholar | PubMed]
- 7.Van Breuseghem I. The pelvic digit: A harmless “eleventh” finger. Br J Radiol 2006;79:e106-7. [Google Scholar | PubMed]
- 8.Murad V, Torres D, Bedoya N, Morillo A. Pelvic rib or pelvic digit: A series of cases. Rev Colomb Radiol 2019;30:5158-63. [Google Scholar | PubMed]
- 9.Keser S, Bayar A, Savranlar A. Ayirici tanida düşünülmesi gereken bir anomali: Pelvik kaburga [Pelvic digit: A case report with reference to the differential diagnosis of pelvis abnormalities]. Acta Orthop Traumatol Turc 2003;37:414-6. [Google Scholar | PubMed]
- 10.Granieri GF, Bacarini L. The pelvic digit: Five new examples of an unusual anomaly. Skeletal Radiol 1996;25:723-6. [Google Scholar | PubMed]
- 11.Das CJ, Debnath J. Nail patella syndrome. Indian J Pediatr 2009;76:1077. [Google Scholar | PubMed]
- 12.Rijal L, Nepal P. Multiple pelvic digits: A rare congenital anomaly. Eur J Orthop Surg Traumatol 2010;20:411-3. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective
February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective January 1, 2025 Uncommon Presentation of Hip Pain Due to Calcific Tendonitis in the Rectus Femoris
January 1, 2025 Uncommon Presentation of Hip Pain Due to Calcific Tendonitis in the Rectus Femoris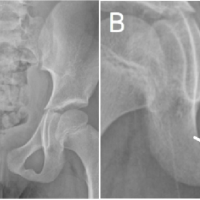 March 10, 2024 Van Neck-Odelberg Disease: A Rare Cause of Pediatric Hip Pain
March 10, 2024 Van Neck-Odelberg Disease: A Rare Cause of Pediatric Hip Pain