
In femoral neck osteochondroma, resection may destabilise the neck, and prophylactic DHS fixation can prevent postoperative fracture in selected high-risk cases.
Dr. Mohamed Cherif El Amraoui, Centre hospitalier de Sens, Sens, France. E-mail : cherifamraoui@yahoo.fr
Abstract
Introduction: Osteochondromas of the femoral neck are rare in adults and may cause mechanical hip pain or impingement. Surgical resection may weaken the femoral neck, exposing patients to fracture risk. Prophylactic fixation remains debated.
Case Report: A 26-year-old woman presented with chronic posterior hip pain. Imaging revealed a posterior femoral neck osteochondroma. Open resection resulted in significant cortical weakening, leading to prophylactic dynamic hip screw fixation. Functional outcome was favourable with stable radiological findings at follow-up.
Conclusion: In selected cases, prophylactic fixation after femoral neck osteochondroma resection may reduce post-operative fracture risk.
Keywords: Osteochondroma, femoral neck, dynamic hip screw, hip pain, prophylactic fixation.
Osteochondromas are the most common benign bone tumours and are typically asymptomatic. Femoral neck involvement is uncommon and may lead to femoroacetabular impingement or mechanical hip pain [1-5]. Imaging plays a crucial role in diagnosis, demonstrating continuity of the cortex and medullary canal and excluding malignant transformation [6]. (Figs. 1-6) Surgical excision is indicated in symptomatic cases. However, resection of femoral neck lesions may compromise structural integrity and increase fracture risk [7,8]. Prophylactic fixation is well established in the management of impending pathological fractures and may be extrapolated to this setting [9-13].
A 26-year-old woman (body mass index 33 kg/m²) presented with chronic left posterior hip pain exacerbated by activity. Physical examination revealed pain during internal rotation and flexion without neurological deficit.
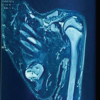
Radiographs and a computed tomography scan demonstrated a well-defined posterior femoral neck osteochondroma measuring approximately 13.5 × 28.5 mm (Figs. 1-6). Bone scintigraphy showed moderate hyperfixation. Magnetic resonance imaging confirmed the benign appearance of the lesion without features of malignant transformation (Figs. 1-6) [6].

Figure 1: Anteroposterior radiograph of the pelvis demonstrating a pedunculated osseous lesion arising from the proximal left femur, consistent with an osteochondroma.
Figure 1: Anteroposterior radiograph of the pelvis demonstrating a pedunculated osseous lesion arising from the proximal left femur, consistent with an osteochondroma.

Figure 2: Dunn lateral radiograph of the hip obtained with the hip flexed and abducted. The bony prominence is visible along the posterosuperior aspect of the femoral neck. The projection is particularly useful in assessing morphological abnormalities associated with femoroacetabular impingement.

Figure 3: Second Anteroposterior view of the pelvis demonstrating a pedunculated osseous lesion arising from the proximal left femur, consistent with an osteochondroma.
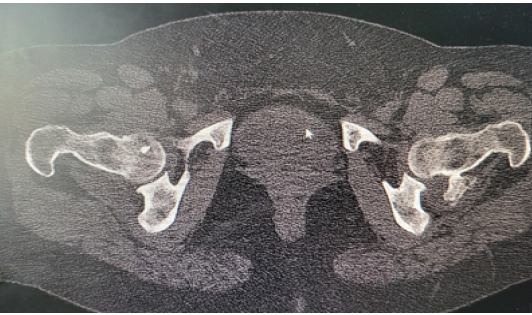
Figure 4: Axial computed tomography scan showing a posterior femoral neck osteochondroma of the left hip. The lesion demonstrates corticomedullary continuity with the proximal femur, a characteristic feature of osteochondroma.
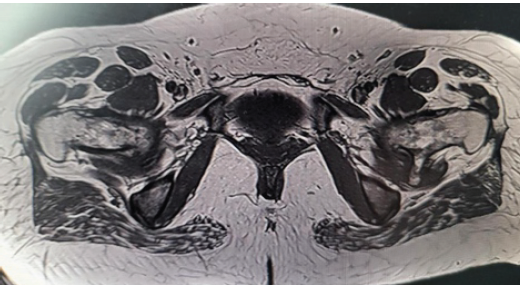
Figure 5: Preoperative axial magnetic resonance imaging demonstrating posterior femoral neck fracture. The lesion arises from the posterior femoral neck with continuity of the cortical and medullary bone, characteristic of osteochondroma, and illustrates its proximity to the adjacent soft-tissue structures.
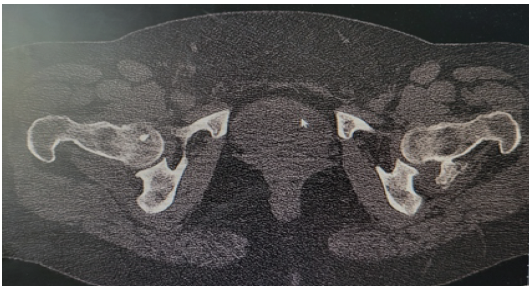
Figure 6: Axial computed tomography scan of the pelvis demonstrating the corticomedullary continuity with the proximal femur and projects posteriorly from the femoral neck, allowing detailed assessment of its osseous anatomy for surgical planning.
Surgical technique:
The patient was positioned in lateral decubitus. A posterior approach allowed direct visualization of the lesion. Complete resection required the removal of a cortical window approximately 1 × 3 cm, resulting in significant weakening of the femoral neck. Considering fracture risk described after similar resections (Fig. 7) [7,8], prophylactic dynamic hip screw (DHS) fixation was performed using a 105 mm lag screw and side plate (Figs. 8 & 9) [9-13].

Figure 7: Macroscopic appearance of the resected femoral neck osteochondroma showing a cartilage cap overlying mature trabecular bone.
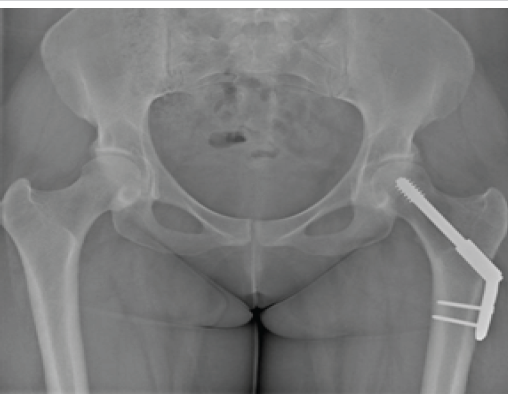
Figure 8: Post-operative anteroposterior view of the pelvis following open resection and prophylactic dynamic hip screw fixation of the proximal femur.

Figure 9: Post-operative Lateral view of the pelvis following open resection and prophylactic dynamic hip screw fixation of the proximal femur. Hardware position is satisfactory, with preservation of the hip joint congruency and no evidence of immediate post-operative complications.
Outcome and follow-up:
Post-operative recovery was uneventful. Progressive weight-bearing was authorised. At 10 months, the patient was pain-free with restored hip mobility. Radiographs demonstrated stable fixation and progressive cortical remodelling, without complications (Figs. 8 & 9) [9-13].
Femoral neck osteochondromas are rare but may cause significant symptoms due to mechanical impingement [2-5]. Posterior localisations are particularly uncommon. Although malignant transformation is exceptional in solitary lesions, imaging assessment is mandatory (Fig. 1-6) [1,6]. Post-operative femoral neck fractures after excision of benign lesions have been reported, highlighting the biomechanical impact of cortical defects [7,8]. Prophylactic fixation follows principles used for impending pathological fractures and aims to prevent catastrophic complications [9-13]. In this case, DHS fixation provided immediate stability and allowed early mobilisation with an excellent clinical outcome (Figs. 8 & 9).
Posterior femoral neck osteochondroma is an uncommon cause of hip pain in adults. When surgical excision results in significant cortical weakening, prophylactic DHS fixation may represent a safe strategy to reduce fracture risk (Figs 8 & 9).
Surgical excision of femoral neck osteochondromas can significantly weaken the femoral neck, and in selected cases, prophylactic fixation should be considered to prevent post-operative fracture.
References
- 1. Kitsoulis P, Galani V, Stefanaki K, Georgios P, Georgios K, Niki J.A., Maria B. Osteochondromas: Review of the clinical, radiological and pathological features. Orthopaedics 2008;31:1018. [Google Scholar] [PubMed]
- 2. Mengnai Li, Timo Luettringhaus, Kevin R. Walker, Peter A. Cole. Operative treatment of femoral neck osteochondroma through a digastric approach in a paediatric patient: a case report and review of the literature. J Pediatr Orthop B. 2012;21(3):230-4. [Google Scholar] [PubMed]
- 3. Fox J, O’Donnell J. Femoral neck exostosis causing femoroacetabular impingement. Hip Int 2016;26:e18-21. [Google Scholar] [PubMed]
- 4. Aldashash F, Elraie M. Solitary osteochondroma of the proximal femur causing sciatic nerve compression. Ann Saudi Med 2017;37:166-9. [Google Scholar] [PubMed]
- 5. Siebenrock KA, Ganz R. Osteochondroma of the femoral neck. Clin Orthop Relat Res 2002;394:211-8. [Google Scholar] [PubMed]
- 6. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar] [PubMed]
- 7. Haviv B, Ganel A, Allon R, Yasin M. Iatrogenic femoral neck fracture after osteochondroma excision. Arch Orthop Trauma Surg 2010;130:1239-43. [Google Scholar] [PubMed]
- 8. Korula RJ, Jebaraj I. Fracture of the femoral neck after excision of osteochondroma. Injury 1995;26:635-6. [Google Scholar] [PubMed]
- 9. Haidukewych GJ. Prophylactic fixation for impending pathological fractures. J Am Acad Orthop Surg 2009;17:493-502. [Google Scholar] [PubMed]
- 10. Li M, Luettringhaus T, Walker KR, Cole PA. Operative treatment of femoral neck osteochondroma through a digastric approach in a paediatric patient: A case report and review of the literature. J Pediatr Orthop B 2012;21:230-4. [Google Scholar] [PubMed]
- 11. Hussain W, Avedian R, Terry M, Peabody T. Solitary osteochondroma of the proximal femur and femoral acetabular impingement. Orthopaedics 2010j;33:51. [Google Scholar] [PubMed]
- 12. Muzaffar N, Bashir N, Baba A, Ahmad A, Ahmad N. Isolated osteochondroma of the femoral neck presenting as hip and leg pain. A case study. Ortop Traumatol Rehabil 2012;14:183-7. [Google Scholar] [PubMed]
- 13. Peterson HA. Multiple hereditary osteochondromata. Clin Orthop Relat Res 1989;239:222-30. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor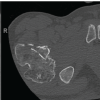 July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review