
Open reduction and internal fixation seem to be an effective and safe way for the treatment of bicondylar tibial plateau fracture in a patient with an amputation below the knee.
Dr. Timothée Helmstetter, Department of Orthopedic Surgery, Hôpital Pourtalès, Rue de la Maladière 45, 2000 Neuchâtel, Switzerland. Email: timothee.helmstetter@gmail.com
Abstract
Introduction: With current prostheses, below-knee amputees have sufficient mobility to perform activities with a risk of trauma and therefore fracture. However, bicondylar fractures of the tibial plateau are rare in this population and we found no recent literature or consensus regarding the management of these fractures. The aim of this study is to report a case with its surgical management, post-operative follow-up, and the specificities inherent in transtibial amputees.
Case Report: This is a case of 33-year-old below-the-knee amputee male who sustained an ipsilateral tibial plateau fracture after an electric scooter accident. The patient underwent open reduction and internal fixation with posteromedial and anterolateral plate using dual incision. We followed the patient for 1 year with good clinical and functional outcomes.
Conclusion: Bicondylar fractures of the proximal tibia in below-knee amputees are rare injuries with potentially severe consequences. Nevertheless, appropriate surgical management and multidisciplinary collaboration with physiotherapists and orthopedic technicians allow the patient to regain mobility and autonomy without compromising prosthesis fitting in the long term.
Keywords: Below-the-knee amputee, stump, osteosynthesis, tibial plateau fracture.
Technological advances in the field of prostheses are now enabling many patients with lower-limb amputation to regain motor function, allowing them to return to demanding professional and sporting activities [1]. Subsequently, accidents and fractures are likely to increase over the next few years in these populations. The incidence of ipsilateral fractures rates 3% in the population of lower-limb amputees [2]. According to the literature, the encountered fractures are mainly those around the hip, as well as fractures of the distal femur, for which conservative treatment appears to provide satisfactory results [3]. To our knowledge, there is no recent literature or consensus on the management of proximal tibial fractures in transtibial amputees. We present the case of a transtibial amputee who underwent an osteosynthesis of a bicondylar fracture of the tibial plateau.
A 33-year-old patient who had undergone a right knee amputation 15 years earlier after a train platform accident presented to our emergency department for knee pain after an electric scooter accident. The patient was known to have a “bony” stump and a history of furunculosis, which made fitting sleeves and prostheses difficult. However, the patient reported a satisfactory function before the fall.

Biplanar radiography of the knee revealed an isolated bicondylar tibial plateau fracture with a valgus deformity, classified as Schatzker [4] (Fig. 1). As described in the 3-column classification of Luo et al., the computed tomography scan shows a split depression of the lateral column associated with a posteromedial fragment [5] (Fig. 2 and 3). No skin lesions were noted and neurovascular status was normal. Weight-bearing was not possible due to pain. We performed surgical treatment with plate osteosynthesis after obtaining the patient’s consent.
Surgical procedure
The patient was positioned supine, and 1.5 g cefuroxime was administrated before induction of general anesthesia. As previously described in the literature, we performed a dual incision with an anterolateral and a posteromedial skin incision [6].

The reduction of the fracture was temporarily secured with a K-wire, and we confirmed the alignment of the articular surface by a lateral sub-meniscal arthrotomy. No meniscal lesion was found. The fracture was stabilized using two plates. The posteromedial plateau was first reduced and then fixed with a posteromedial 3.5-mm third tubular buttress plate.
The lateral column fixation was achieved with a 3.5-mm locking compression plate. Long subchondral screws were used to support the articular surface.

Fracture reduction was assessed by fluoroscopic images revealing no intra-articular material and satisfactory fracture reduction. The knee was stable in both coronal and sagittal planes.
Follow-up
The radio-clinical follow-up was at 6 weeks and 3, 6, and 12 months after the operation. The patient underwent physiotherapy. During the 6 post-operative weeks, only passive and active knee flexion/extension of 90°–0°–0° was permitted. No weight bearing was allowed until bone consolidation. From 7 post-operative weeks, free range of motion was allowed and progressive strengthening with emphasis on knee and hip extensor reinforcement started. The patient’s knee range of motion and mobility level according to amputee single item mobility measure (AMPSIMM) [7] is resumed in Table 1. At the 6-week follow-up, the patient was free from pain and did not require analgesics. The X-rays showed no secondary displacement of the material nor the fracture (Fig. 4). Partial weight-bearing and exercise against resistance were permitted. The scars were not painful. We requested an orthopedic technician to add protective measures on the temporary sleeve and to adapt the pressure points in the prosthesis. At the 3-month follow-up, no pain was reported. The fractures had signs of consolidation on the X-ray (Fig. 5). Full weight-bearing was allowed. The patient tolerated the prosthesis with partial weight-bearing well; however, the pressure points were not fully adapted. At the 6-month follow-up, the X-rays showed complete consolidation of the fracture (Fig. 6). Despite of sleeve and prosthesis adjustments, the patient complained of discomfort related to the pressure point on the lateral side. Full weight-bearing was possible without aid but the patient needed crutches for a long way. At 1-year follow-up, the patient was unable to wear the prosthesis for an entire day due to pressure points on the lateral tibial condyle. Palpation of the lateral plate was sensitive. We proposed the removal of the osteosynthesis material only on the lateral side. The X-rays showed osteoarthritis of the lateral femorotibial compartment (Fig. 7). The anterolateral plate was successfully removed (Fig. 8). At the 6-week follow-up after removal, the patient had no more pain on the lateral side and gave a mobility level of 6 according to AMPSIMM [7]. The patient regained his pre-fracture knee range of motion with no clinical signs of arthrofibrosis.
Tibial plateau fractures represent 1.2% of all fractures within the population. Accounting for 15% of tibial plateau fractures, bicondylar fractures are even rarer, but they have a poor prognosis with a complication rate of up to 30% [8]. In such fractures, the main goals of surgical intervention are to restore the joint articular surface and mechanical alignment, to preserve soft tissue structures, and to stabilize the joint to permit an early mobilization [9]. Achievement of these goals maximizes the return to pre-traumatic level of function and minimizes the occurrence of complications, particularly post-traumatic osteoarthritis. In our case, achieving these goals was even more important because for transtibial amputees fitted with a prosthesis, stability and mobility of the knee as well as maintenance of the knee’s mechanical axis are crucial to ensuring an energy-efficient gait. In a retrospective study with below-the-knee amputees, composed of 27 patients with distal femur fractures and 7 patients with proximal tibia fractures, eighty were conservatively treated [3]. No differences in terms of knee range of motion between conservative and surgical treatment were found, but half of the patients had a mean range of motion loss of 30°. According to the authors, distal femur fractures responded well to conservative treatment because deforming forces are lower in below-the-knee amputees. However, no recommendations were given for fractures of the proximal tibia. In our case, we felt that the benefit of surgery in terms of function was more important than the risk of having a troublesome scar. Moreover, the patient’s fracture met indication criteria of tibia plateau fracture such as loss of joint congruency of the lateral condyle with a joint step of >3 mm, lack of stability in the coronal plane due to damage to the lateral and medial tibial condyle, and valgus deviation of the joint due to the joint impaction. Due to the young age of the patient and the good bone quality, we choose open reduction and internal fixation instead of total knee arthroplasty. Maintaining the functionality of the his and knee extensor muscles plays an essential role for the lower limb amputees, enabling them to stand effectively. Our post-operative protocol allows our patient to regain his pre-fracture knee range of motion and to regain his previous mobility level with a score of 6 according to AMPSIMM [7]. No type of post-operative immobilization was performed besides the prosthesis itself. Van Dreumel et al. observed osteoarthritis in 58% of patients with a bicondylar fracture after 1 year but no relationship was found between osteoarthritis and the functional outcome [10]. Our patient showed characteristics of osteoarthritis in the lateral tibiofemoral compartment but was asymptomatic at 1-year post-operative. Because of implant-related complaints, we decided to remove the plate after 1 post-operative year. Due to bulking of the plate, we think that lateral plate removal is mandatory in patients fitted with a prosthesis and we would advise to warn the patient in a similar case. Due to the pressure point, we had to ask the orthopedic technician to adapt the sleeve and the prosthesis. These modifications helped the patient and allowed him to start to walk. Due to the high cost of a prosthesis, we would advise to do a new prosthesis, if necessary, only after plate removal.
Bicondylar fractures of the proximal tibia in below-knee amputees are rare injuries with potentially severe consequences. Nevertheless, appropriate surgical management and multidisciplinary collaboration with physiotherapists and orthopedic technicians allow the patient to regain mobility and autonomy without compromising prosthesis fitting in the long term. We believe that it is important to inform the patient of the evolution and progression of his/her mobility over 1 year. Return to pre-fracture mobility appears to be possible only after the removal of the osteosynthesis material.
Surgical indications of bicondylar proximal tibial fractures in the main population could be extended to below-the-knee amputees with special attention to post-operative management.
References
- 1.Softness KA, Murray RS, Evans BG. Total knee arthroplasty and fractures of the tibial plateau. World J Orthop 2017;8:107-14. [Google Scholar | PubMed]
- 2.Denton JR, McClelland SJ. Stump fractures in lower extremity amputees. J Trauma 1985;25:1074-8. [Google Scholar | PubMed]
- 3.Bowker JH, Rills BM, Ledbetter CA, Hunter GA, Holliday P. Fractures in lower limbs with prior amputation. A study of ninety cases. J Bone Joint Surg Am 1981;63:915-20. [Google Scholar | PubMed]
- 4.Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968--1975. Clin Orthop Relat Res 1979;138:94-104. [Google Scholar | PubMed]
- 5.Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010;24:683-92. [Google Scholar | PubMed]
- 6.Georgiadis GM. Combined anterior and posterior approaches for complex tibial plateau fractures. J Bone Joint Surg Br 1994;76:285-9. [Google Scholar | PubMed]
- 7.Norvell DC, Williams RM, Turner AP, Czerniecki JM. The development and validation of a novel outcome measure to quantify mobility in the dysvascular lower extremity amputee: The amputee single item mobility measure. Clin Rehabil 2016;30:878-89. [Google Scholar | PubMed]
- 8.Khatri K, Sharma V, Goyal D, Farooque K. Complications in the management of closed high-energy proximal tibial plateau fractures. Chin J Traumatol 2016;19:342-7. [Google Scholar | PubMed]
- 9.Mthethwa J, Chikate A. A review of the management of tibial plateau fractures. Musculoskelet Surg 2018;102:119-27. [Google Scholar | PubMed]
- 10.van Dreumel RL, van Wunnik BP, Janssen L, Simons PC, Janzing HM. Mid-to long-term functional outcome after open reduction and internal fixation of tibial plateau fractures. Injury 2015;46:1608-12. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function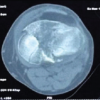 July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery
July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study
June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study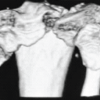 May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study
May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study