
The vacuum-assisted bone harvester presents a novel approach for biopsy and curettage of bone lesions like osteofibrous dysplasia, offering advantages such as simultaneous suction and curettage, potentially reducing local recurrence rates and minimizing contamination of surrounding tissues.
Mr. Kevin A Wu, Department of Orthopedic Surgery, Duke University Medical Center, 2927 40 Duke Medicine Circle 124 Davison Building, Durham - 27710, North Carolina, United States. E-mail: kevin.a.wu@duke.edu
Abstract
Introduction: Osteofibrous dysplasia (OFD) is a rare benign bone lesion primarily affecting the tibia, characterized by fibrous tissue proliferation with varying osseous involvement. Diagnosis involves clinical evaluation, imaging, and histopathological analysis. Traditional bone biopsies for OFD can be challenging due to the lesion’s nature.
Case Report: We present a case report of a young patient presenting with pain concerning for OFD and describe a novel technique for biopsy and curettage using a vacuum-assisted bone harvester.
Conclusion: The vacuum-assisted bone harvester allows the surgeon to effectively obtain a biopsy and curettage.
Keywords: Osteofibrous dysplasia, biopsy, bone harvester.
Osteofibrous dysplasia (OFD) is a benign bone lesion predominantly affecting the tibia, characterized by the proliferation of bland fibrous tissue with varying degrees of osseous involvement [1]. OFD is a rare condition, usually found in children under the age of 10 [2]. Diagnosis of OFD typically involves clinical examination, radiographic imaging, and histopathological analysis of biopsy specimens [3]. Bone biopsies are typically obtained using either an image-guided core needle biopsy (IGCBN) technique or a mini-open technique in which tissue is removed with curettes. However, obtaining adequate biopsy samples for definitive diagnosis can be challenging due to the small size of the needle (in the case of IGCBN), the lesion’s heterogeneous nature, and the presence of reactive bone surrounding the true lesion [3]. Recently, we have started using a vacuum-assisted bone harvester designed for harvesting bone grafts and marrow. Bone grafts are commonly harvested for orthopedic procedures such as fusions, nonunion repair, fracture repair, and treatment of bone defects [4,5]. While bone graft harvesting has historically relied on manual techniques, new technologies have been developed to streamline the process. We present a case report and describe a novel application of a vacuum-assisted bone harvester for obtaining biopsy specimens in a patient with suspected OFD. The patient’s parents were informed that data concerning the case would be submitted for publication, and they provided consent.
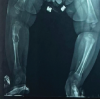
A previously healthy 7-year-old female without any relevant medical, surgical, or family history presented with 1 year of left anterior leg pain accompanied by antalgic limping. There was no inciting trauma or pain at rest. However, pain persisted during activities such as basketball and martial arts. Family reported notable swelling over the left shin. Physical examination of the left lower extremity revealed swelling over the anterior proximal tibial diaphysis and tenderness to palpation. She had a full and painless range of motion of the left hip, knee, and ankle. Anterior-posterior and lateral radiographic views of the left leg demonstrated a lytic lesion in the anterior tibial diaphyseal cortex (Fig. 1). The lesion demonstrated a geographic appearance with a sclerotic border, multiple chambers, and mild cortex expansion. Biopsy was recommended for a definitive diagnosis of OFD versus adamantinoma.

The patient was placed supine on a radiolucent table. She received an adductor canal peripheral block for post-operative pain management and general anesthesia for the operation. Standard antibiotic treatments were given, and the left leg was prepared and draped in standard fashion. A tourniquet was placed and inflated. A 3 cm incision was made longitudinally over the palpable location of the tumor over the anteromedial shin. The incision was taken just through dermis and then cautery was used to dissect down through the periosteum and to the bone.

A bone introducer (Avitus® Pilot Hole Creator, Zimmer Biomet, Warsaw, IN) which is an accompaniment of the vacuum-assisted bone harvesting device (Avitus® Bone Harvester, Zimmer Biomet, Warsaw, IN) was used to core out a small corticotomy to introduce a curette into the medullary canal. An angled curette was used to remove a sample of pathological bone, and the specimen was sent to pathology. The vacuum-assisted bone harvester (Avitus® Bone Harvester, Zimmer Biomet, Warsaw, IN) was used to complete the curettage of lesional bone (Fig. 2). The device was positioned such that its curette-shaped tip was able to be inserted into the corticotomy and was connected to a standard operating room suction (Fig. 3). The device has a suction trap within its handle such that all removed tissue is saved and is not routed directly into the suction canister. To ensure that the lesion was completely removed, the curette end was scraped along the inner cortex of the bone. A separate specimen was sent to compare the slides from using a curette versus the vacuum-assisted bone harvester (Fig. 4). All curetted bone matter (from both the curette and device) was sent for frozen and permanent pathology. Fluoroscopy was used to ensure that all septations were opened and that the entire cavity was thoroughly explored.

The cavity was irrigated with saline and then hydrogen peroxide for 3 min (our typical adjuvant for specific benign or benign-aggressive bone lesions) before re-irrigation with saline. Before filling of the defect and wound closure, intraoperative pathology based on frozen sections was reviewed with the pathologist on duty and was found to be consistent with OFD. Both samples (one from the device and one was the curette) were deemed equally sufficient to make the intraoperative diagnosis of OFD. The cavity was dried, and osteocrete bone graft putty (Bone Solutions Incorporated, Colleyville, TX) was uniformly distributed within the defect, confirmed under fluoroscopy. Subsequently, the wound was irrigated, and the periosteum was reapproximated using 2–0 vicryl. Layered skin closure was performed with 2–0 vicryl, 3–0 biosyn, and skin glue. Finally, the wound was dressed, and a long leg splint was applied in partial knee flexion.
Her post-operative period was complicated by a partial wound dehiscence at 3 weeks, requiring irrigation and debridement and repeat wound closure in the operating room. Despite this complication, she has been doing well since and reported no pain ambulating 3 months after her original surgery. At 4 months, she was cleared to return to normal weight-bearing activities and subsequently returned to all normal activities (Fig. 5). The Patient reported no symptoms at her 1-year follow-up. At the patient’s most recent follow-up at 1.5 years, she reported no issues and has continued her normal activities.
We describe here a novel application for a vacuum-assisted bone harvester for the biopsy and curettage of a benign bone lesion. The bone harvester includes a bone introducer that can be used to penetrate the cortex of the bone to allow the placement of the device within the bone to remove the lesion. Although it was designed initially for use to harvest bone grafts, the bone harvester was adapted in this case for removing a lesion from within the bone [6]. This device has additionally been approved for bone infection debridement and curettage of skeletal lesions. We have used this device both in the fashion shown -to complete a curettage -as well as for percutaneous biopsy of bone lesions in which we wish to obtain more tissue than can be obtained using a core biopsy needle. One advantage of utilizing this technique is the ability to suction and curette simultaneously. With manual curettage, each pass of the curette requires the instrument to be removed and cleaned before re-insertion into the bone. In addition to the increased efficiency that attends to being able to leave the “curette” inside the lesion, one could speculate that repeated introduction and removal of a curette could be responsible for the high local recurrence rates seen in lesions treated with curettage [7]. OFD is an example of a lesion prone to local recurrence and using a suction device may have the added benefit of capturing most of the cells [8] without repeated removal of the curette through the adjacent tissues. The device’s sharp curette end enables bone scraping while simultaneously providing suction, preventing tissue from inadvertently being forced deeper into the bone. OFD is one of several bone lesions for which minimizing contamination of surrounding tissues is essential in other cases to prevent tumor seeding [9]. The device’s handle not only facilitates specimen storage but also ensures the preservation of the sterile field by enabling safe transfer of the specimen inside without exposing other surgical instruments. It is important to note that the patient was kept non-weight-bearing for the 1st few weeks following surgery. This precaution was taken due to the size of the original bone lesion and the risk of fracture post-removal, especially considering the bone defect during the acute phase. We opted to maintain a non-weight-bearing status until there was clear radiographic evidence of bone remodeling and healing. Once the patient demonstrated sufficient radiographic healing, she was promptly able to resume her normal activities. One concern we had discussed when we first began using this device as described was the potential for the tissue within the suction trap to be subject to artifact either due to disruption of the architecture due to suction or the presence of clotted blood. Pathological slide evaluation of the specimens harvested from the device did not demonstrate destroyed architecture compared to the normal curette sample. Histopathological examination of OFD typically reveals fibro-osseous lesions characterized by irregular fragments of woven bone bordered by well-defined osteoblasts [1,10]. In this case, using both the vacuum-assisted device and the traditional curette yielded indistinguishable histologic findings, as observed by the pathologist, and ultimately identical diagnoses [11]. The only measurable difference noted was in the amount of tissue collected through each method, with almost double the amount of tissue being collected by volume through the vacuum-assisted device. The potential limitations of the technique include the expense of the vacuum-assisted bone harvester. However, it is possible that this cost is compensated by the increased speed with which a tumor may be removed using the bone harvester. In addition, in situations where swift removal of diseased tissue is crucial and it is essential to minimize contamination of the surgical field, utilizing this device may be worth the increased cost. Because the device is able to be attached to a standard operating room suction without requiring additional equipment there are no associated “hidden” costs to using the device. We are unable to provide a specific cost for the device due to pricing variations across the country. The method above describes a novel application of a vacuum-assisted bone harvester to remove a benign lesion of bone and the potential advantages and disadvantages are described.
OFD is a rare benign bone lesion primarily affecting the tibia, mainly found in children under 10. Diagnosis involves clinical, imaging, and histopathological analysis. Traditional bone biopsies for OFD can be challenging due to the lesion’s nature and surrounding reactive bone. A vacuum-assisted bone harvester was successfully used for biopsy and curettage in a young patient with OFD. This novel technique offers several advantages, including simultaneous suction and curettage, which may enhance the efficiency and effectiveness of bone lesion management. In addition, the device’s ability to minimize contamination of surrounding tissues and potentially reduce local recurrence rates makes it a valuable tool for orthopedic surgeons. Further studies and long-term follow-up are warranted to validate these findings and explore the full extent of this technique’s benefits in the management of bone pathology.
The vacuum-assisted bone harvester represents an innovative approach for obtaining biopsy specimens and performing curettage in bone lesions like OFD. Orthopedic surgeons should consider incorporating this technique into their practice, particularly in cases where traditional methods may be challenging or less effective.
References
- 1.Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO classification of soft tissue tumours: News and perspectives. Pathologica 2021;113:70-84. [Google Scholar | PubMed]
- 2.Most MJ, Sim FH, Inwards CY. Osteofibrous dysplasia and adamantinoma. J Am Acad Orthop Surg 2010;18:358-66. [Google Scholar | PubMed]
- 3.Saber AY, Patel BC. Osteofibrous dysplasia. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar | PubMed]
- 4.Archunan MW, Petronis S. Bone grafts in trauma and orthopaedics. Cureus 2021;13:e17705. [Google Scholar | PubMed]
- 5.Jakoi AM, Iorio JA, Cahill PJ. Autologous bone graft harvesting: A review of grafts and surgical techniques. Musculoskelet Surg 2015;99:171-8. [Google Scholar | PubMed]
- 6.Lukasiewicz AM, Bagi PS, Yu KE, Tyagi V, Walls RJ. Novel vacuum-assisted method for harvesting autologous cancellous bone graft and bone marrow from the proximal tibial metaphysis. Foot Ankle Orthop 2021;6:1-5. [Google Scholar | PubMed]
- 7.Guo W, Sun X, Zang J, Qu H. Intralesional excision versus wide resection for giant cell tumor involving the acetabulum: Which is better? Clin Orthop Relat Res 2012;470:1213-20. [Google Scholar | PubMed]
- 8.Park JW, Lee C, Han I, Cho HS, Kim HS. Optimal treatment of osteofibrous dysplasia of the tibia. J Pediatr Orthop 2018;38:e404-10. [Google Scholar | PubMed]
- 9.Berger-Richardson D, Xu RS, Gladdy RA, McCart JA, Govindarajan A, Swallow CJ. Glove and instrument changing to prevent tumour seeding in cancer surgery: A survey of surgeons’ beliefs and practices. Curr Oncol 2018;25:e200-8. [Google Scholar | PubMed]
- 10.Campanacci M. Osteofibrous dysplasia of long bones a new clinical entity. Ital J Orthop Traumatol 1976;2:221-37. [Google Scholar | PubMed]
- 11.Wu KA, Shenoy D, Sachs E, Somarelli JA, Pean C, DeBaun M, Brigman BE, Visgauss JD, Eward WC. Exploring versatile applications of a vacuum-assisted bone harvester in orthopedic surgery. BMC Musculoskelet Disord 2024;25(1):688:1-13. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Osteofibrous Dysplasia in a 4-Month-Old: A Rare Presentation in Early Infancy
June 1, 2026 Osteofibrous Dysplasia in a 4-Month-Old: A Rare Presentation in Early Infancy May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report
August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report May 1, 2025 Benign Spindle Cell Tumor of Flexor Tendon Sheath of Toe: A Rare Case Report
May 1, 2025 Benign Spindle Cell Tumor of Flexor Tendon Sheath of Toe: A Rare Case Report