
Osteofibrous dysplasia presents as a lytic, tender swelling in infants, which is confirmed with early imaging and biopsy, and then treated conservatively with close monitoring in uncomplicated cases.
Dr Raja Ganesh Rayudu, Department of Orthopedics, Dr. D. Y. Patil Hospital, Navi Mumbai, Maharashtra, India. E-mail: rajaganesh70@gmail.com
Abstract
Introduction: Osteofibrous dysplasia (OFD) is a non-malignant lesion of cortical bone, where fibrous tissue replaces normal bone. Its presentation is rare in infants and may clinically and radiologically mimic other malignant lesions such as adamantinoma, making diagnosis challenging. Biopsy and imaging play a key role in diagnosis.
Case Report: The patient, a 4-month-old infant of Indian origin, presented with a tender swelling over the proximal aspect of the right tibia. Radiographic evaluation revealed a lytic lesion. Further magnetic resonance imaging and histopathological evaluation confirmed the diagnosis of OFD. We planned to treat it conservatively and monitor the lesion size regularly, given the patient’s age and absence of complications. Surgical intervention is deferred unless there is progression or functional compromise.
Conclusion: This case highlights the diagnostic challenges of OFD in infants and its differentiation from malignant lesions. Through this report, we aim to broaden clinical awareness regarding the occurrence of OFD in young infants and emphasise the role of imaging and biopsy in establishing a definitive diagnosis.
Keywords: Osteofibrous dysplasia, pediatric orthopedics, tibial swelling, infant bone lesions, fibro-osseous tumor.
Osteofibrous dysplasia (OFD) is a benign fibro-osseous condition of bone that typically affects the cortical bone of the anterior mid-shaft of the tibia in children [1]. The term OFD was first devised by Dahlin and Johnson in 1972 [2]. The usual age of presentation of OFD ranges from 7 days to 22 years [3]. Skeletal neoplasms of the newborn and neonates are rarely encountered, and only a few cases have been reported. It is frequently misdiagnosed owing to a lack of distinctive radiographic findings and inadequate sampling materials [4]. OFD typically presents as a monostotic lesion, affecting a single bone in about 85% of cases. However, 5% of cases show polyostotic involvement (multiple bones affected) [5]. This report describes a rare case of OFD in a 4-month-old infant.
A 4-month-old male infant was brought to D. Y. Patil Hospital by his mother with a chief complaint of swelling in the right lower limb for the last 10 days. There was no history of trauma, fall, or injury. The child was irritable and crying but was feeding well. The swelling was bony, hard, and non-progressive over the proximal tibia. Tenderness was noted over the swelling, indicated by the infant’s crying during palpation. The swelling was firmly fixed, without any discharging sinuses. He had no history of fever and chills. No associated history of any trauma, ENT or ocular bleeding, loss of consciousness, or vomiting and was then admitted for further evaluation. The patient had no significant medical history. He had a normal full-term delivery with no significant birth complications. Developmental milestones were age-appropriate for 4 months. He was fully immunised for his age. Family history was notable for a non-consanguineous marriage. No known family history of genetic disorders or similar illnesses. The patient was breastfed from birth. On general examination, the patient was conscious and alert, responding to auditory and visual stimuli, recognised his mother, and had an appropriate cry for his age. He was afebrile, with a pulse rate of 120/min and SPO₂ of 100% on room air. Pallor, icterus, cyanosis, clubbing, lymphadenopathy, and oedema were all negative. On inspection of the right lower limb, a diffuse swelling measuring 1.7×1 cm was noted over the proximal tibia. No scars, erythema, dilated veins, tattoo marks, discolouration, fissures, sinuses, or ecchymoses were present. There was no local rise in temperature. Toe movement and sensation were present. Distal pulses were palpable. X-ray reports revealed an ill-defined expansile lytic lesion involving the diaphysis of the proximal right tibia. Therefore, we then performed a J-needle biopsy with an above-knee cast application. The sample was sent for histopathology examination, which showed a lesion composed of fibrous stroma and bony trabeculae, which was lined by osteoblasts.
Radiographs:
Anteroposterior (Fig. 1) and lateral (Fig. 2) X-rays demonstrate an expansile osteolytic lesion involving the medullary cavity of the proximal diaphysis of the right tibia. The margins were well-defined, multilobulated and irregular.

Figure 1: Anteroposterior X-rays.

Figure 2: Lateral X-rays.
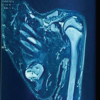
MRI:
Proton density fat-saturated images demonstrated hyperintense lesions with few hypointense areas. (Figs 3 and 4).
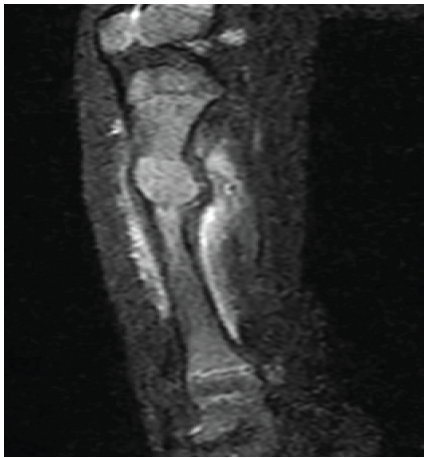
• Figure 3: Sagittal T1-weighted magnetic resonance imaging shows an expansile mass replacing the medullary space, showing intermediate intensity signals.
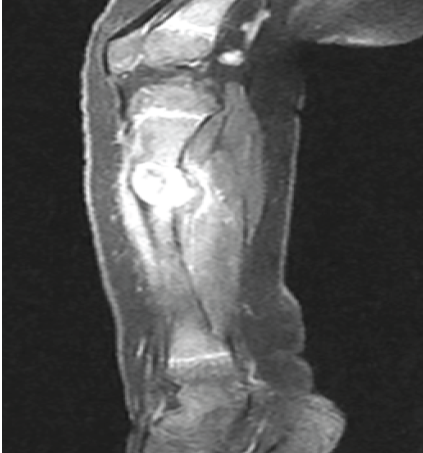
Figure 4: Sagittal T2-weighted magnetic resonance imaging reveals heterogeneous hyperintense signal intensity.
Histopathology (Fig. 5, 6, 7, 8, 9):
Histopathology revealed bony trabeculae lined by osteoblasts within a fibrous stroma.
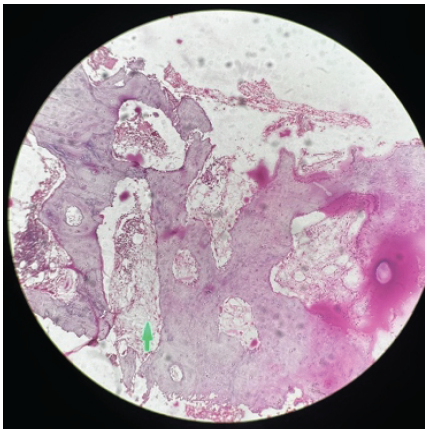
Figure 5: Woven bone trabeculae rimmed by osteoblasts.
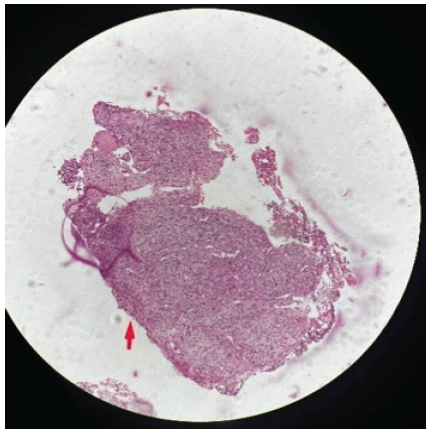
Figure 6: Bland fibroblastic stroma.
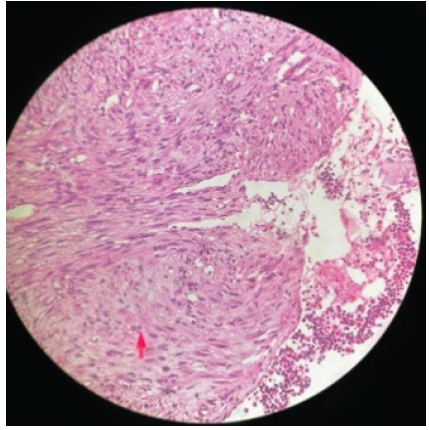
Figure 7: Fibrous stroma with spindle to stellate-shaped cells.
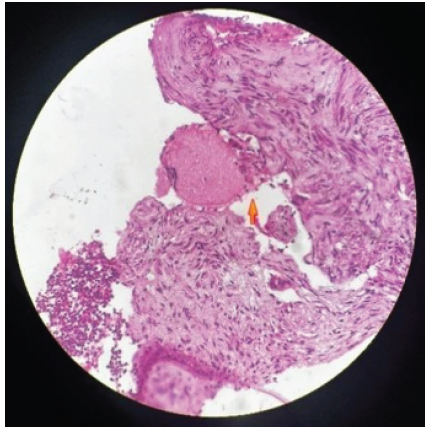
Figure 8: Multinucleated giant cell in the fibrous stroma.
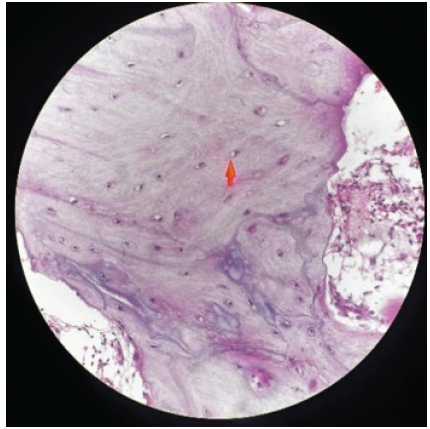
Figure 9: Woven bone with osteocytes in the lacunae.
OFD is a rare, benign, fibro-osseous cortical bone lesion most commonly found in children, typically between 1 and 10 years of age, and predominantly affecting the anterior tibial cortex [1]. Neonatal or infantile presentation is extremely rare, with very few cases reported worldwide. The earliest documented case was in a 3-day-old neonate, described by Castaldo et al., who presented with a tibial swelling later confirmed as OFD on biopsy [6]. Another case by Hindman et al. reported a pathological fracture of the tibia at birth due to congenital OFD [7]. Our case of a 4-month-old infant thus represents a rare early-age manifestation, expanding the known age spectrum of OFD and highlighting the importance of including it in the differential diagnosis of tibial lesions, even in infancy.
Clinical and radiological features:
The child presented with a firm, non-mobile, tender swelling over the proximal tibia without systemic signs such as fever or trauma. These features are consistent with typical OFD presentations [1,8]. Radiographs showed a well-defined, eccentric, expansile lytic lesion with multilobulated contours, involving the diaphyseal cortex of the proximal tibia – a hallmark radiological feature of OFD [1,5]. MRI confirmed intermediate T1 and heterogeneously hyperintense T2 signal changes within the lesion, with no soft-tissue involvement or periosteal reaction – features supportive of a benign fibro-osseous process [6,9]. Radiographic surveillance is recommended every 6–12 months until skeletal maturity, particularly for:
- Large lesions
- Unusual sites (e.g., fibula, radius)
- Patients <5 years at diagnosis
- Suspected recurrence or progression.
An MRI should be repeated in case of symptom changes or rapid lesion growth to exclude soft-tissue invasion or malignant transformation [8,9].
Histopathology and differential diagnosis:
Histopathology remains the gold standard for OFD diagnosis. The biopsy in our case revealed woven bone trabeculae lined by osteoblasts within a fibrous stroma, a confirmatory feature of OFD [1,10]. Differentiation from other fibro-osseous lesions is essential:
- Fibrous dysplasia lacks osteoblastic rimming and tends to be more medullary rather than cortical [10].
- Classic adamantinoma includes nests of epithelial cells that stain positive for cytokeratin, indicating malignancy [10].
- OFD-like adamantinoma, an intermediate lesion, shows sparse epithelial elements but can behave more aggressively [9,10].
The exact aetiology of OFD remains uncertain. It is considered a developmental lesion, not a true neoplasm. Some studies suggest a potential link between OFD and adamantinoma due to histological and radiological similarities. Molecular studies have identified cytokeratin expression in stromal cells of some OFD cases, blurring the lines between OFD and OFD-like adamantinoma [9,10]. While adamantinoma exhibits epithelial gene expression (e.g., keratin-14 and -19), OFD does not consistently show this. However, rare progression of OFD to adamantinoma has been described, making long-term vigilance essential, even in histologically benign lesions [9]. Moreover, GNAS mutations, which are commonly found in fibrous dysplasia, are typically absent in OFD, helping distinguish the two entities at the molecular level [10]. Some experts view OFD and OFD-like adamantinoma as part of a spectrum, where OFD may be a precursor lesion to adamantinoma. OFD-like adamantinoma contains sparse epithelial cells and has intermediate behaviour. However, no clear progression pathway has been proven definitively [9]. This overlap has led to ongoing controversy in the classification and nomenclature of these lesions. Immunohistochemistry (cytokeratin positivity) and close clinical monitoring are crucial to distinguish benign from low-grade malignant lesions, especially in recurrent or aggressive cases. Thus, histology and immunohistochemistry play a crucial role in distinguishing these entities.
Management:
OFD is considered self-limiting, often regressing spontaneously after skeletal maturity. Studies show that conservative management (biopsy and observation) is usually sufficient, particularly when deformity and fracture risk are low [1,8]. Dala-Ali et al. reported in a multicentre review that angular deformity <10° at presentation predicted good outcomes without surgery [11]. Recurrence rates post-curettage are high (~70%), but malignant transformation is exceedingly rare [1,11]. In our case, a diagnostic biopsy and protective above-knee cast were sufficient to manage the child, given the absence of deformity or fracture. Surgical intervention, such as curettage or resection, should be reserved for progressive deformity, functional impairment, or ambiguous diagnosis [8,11]. Children diagnosed with OFD require regular follow-up with radiographs, especially during growth spurts, to monitor lesion size, cortical expansion, and tibial alignment [8,11]. Although most regress or remain stable, rare progression or deformity (especially anterior bowing) may develop and should be addressed promptly.
This case highlights an unusual presentation of OFD in early infancy and contributes to the limited existing literature on its occurrence at such a young age. Reporting rare infantile presentations broadens the recognised clinical spectrum of the disease and improves understanding of its natural history. Increased awareness of OFD in infants may support more informed clinical decision-making and help optimise long-term outcomes through age-appropriate management strategies.
Although OFD is uncommon in infancy, it should be included in the differential diagnosis of lytic tibial lesions in the pediatric population to avoid misdiagnosis. Awareness of this entity allows for appropriate evaluation and timely diagnosis, thereby preventing unnecessary aggressive treatment. Conservative management with regular radiological follow-up is a safe and effective approach in the absence of progression or functional impairment.
References
- 1. Saber AY, Patel BC. Osteofibrous Dysplasia. Treasure Island, FL: StatPearls; 2023. [Google Scholar] [PubMed]
- 2. Dahlin DC, Johnson EW Jr. Fibrous dysplasia. Pathologic and radiologic features. Radiol Clin North Am 1972;10:103-23. [Google Scholar] [PubMed]
- 3. Kim SY, Lee SH. Congenital osteofibrous dysplasia, involving the tibia of a neonate. J Korean Soc Radiol 2015;73:307-11. [Google Scholar] [PubMed]
- 4. Hindman BW, Bell S, Russo T, Zuppan CW. Neonatal osteofibrous dysplasia: Report of two cases. Pediatr Radiol 1996;26:303-6. [Google Scholar] [PubMed]
- 5. Liu R, Tong L, Wu H, Guo Q, Xu L, Sun Z, et al. Osteofibrous dysplasia: A narrative review. J OrthopSurg Res 2024;19:204. [Google Scholar] [PubMed]
- 6. Castaldo A, Siervo A, Ferrara D, Giugliano AM, Errico ME, Zeccolini M, et al. Osteofibrous dysplasia: A rare case in 3 day old female. Radiol Case Rep 2021;17:825-31. [Google Scholar] [PubMed]
- 7. Hindman BW, Bell S, Russo T, Zuppan CW. Neonatal osteofibrous dysplasia: Report of two cases. Pediatr Radiol 1996;26:303-6. [Google Scholar] [PubMed]
- 8. Westacott D, Kannu P, Stimec J, Hopyan S, Howard A. Osteofibrous dysplasia of the tibia in children: outcome without resection. J Pediatr Orthop. 2019;39(8):e614-e621.. [Google Scholar] [PubMed]
- 9. Park YK, Unni KK, McLeod RA, Pritchard DJ. Osteofibrous dysplasia: Clinicopathologic study of 80 cases. Hum Pathol 1993;24:1339-47. [Google Scholar] [PubMed]
- 10. Dala-Ali B, Donnan L, Masterton G, Briggs L, Kauiers C, O’Sullivan M, et al. Osteofibrous dysplasia of the tibia: The importance of deformity in surveillance. Bone Joint J 2022;104-B:302-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis