
In cases of clinical and radiological suspicion of malignant transformation in osteochondroma, it is advisable to plan for wide excision with clear margins as definitive management. It is also important to follow-up such patients regularly to look for signs of local recurrence/metastasis
Dr. Vineet Thomas Abraham, Department of Orthopaedics, All India Institute of Medical Sciences, Guntur, Andhra Pradesh, India. E-mail: abrahamvineet@hotmail.com
Abstract
Introduction: Osteochondroma is a benign bone tumor, commonly seen as a bony outgrowth from the metaphysis of long bones, having a stalk and cartilage cap. They may be sessile or multiple and usually arise before 20 years of age with no growth beyond puberty. Malignant transformation is a rare complication seen in 1% of solitary cases and 3–5% in the hereditary multiple enchondromatosis variety. Here, we report a rare case of atypical benign osteochondroma with clinical and radiological features suggestive of a malignant transformation.
Case Report: A 17-year-old boy presented to us with a complaint of swelling in his right thigh for 12 years. Radiological features were suggestive of malignant transformation, with bony outgrowth exhibiting heterogeneous calcification, local invasion, and a cartilage cap of size 2.5 cm. Bilateral lung nodules were detected on high-resolution computed tomography. Positron emission tomography scan showed no evidence of metastasis. The patient underwent a wide excision of the tumor and the histopathology revealed it to be a benign osteochondroma. It is an atypical presentation of osteochondroma in which we had a discrepancy in radio-histopathological correlation.
Conclusion: In instances of diagnostic uncertainty concerning atypical osteochondroma, opting for an excisional biopsy serves as a prudent next step for the planning of subsequent management. The patient needs to be followed up regularly to look for recurrence or any other signs of metastasis.
Keywords: Osteochondroma, exostosis, HME, imaging, chondrosarcoma.
Osteochondroma is the most common benign bone tumor [1]. It is not a true neoplasm but a developmental enchondromatous hyperplasia leading to a bony outgrowth on the external surface of long bones, usually arising from the metaphyseal area [2]. Classically, it has two pathognomonic features: The presence of medullary cavity continuity with the parent bone and a cartilaginous cap [3,4]. It may present as a solitary lesion or manifest as multiple hereditary enchondromatosis syndrome as an inherited autosomal dominant genetic disease [5]. Metastatic transformation is a rare complication seen in 1% of solitary cases and 3–5% in the hereditary multiple enchondromatosis variety, with symptoms such as an increase in size beyond skeletal maturity and new sudden onset pain [6]. Radiological signs such as cartilage cap of more than 1.5 cm in skeletally mature patients, irregular or indistinct surface of the lesion, focal radiolucency, heterogeneous irregular or scattered calcifications, and local soft-tissue invasion are strongly suggestive of the same [1].
A 17-year-old healthy male presented to us with complaints of painless swelling in the right thigh for the past 12 years. The swelling was first noticed at the age of 4 years, which progressively increased in size over the next 8 years. For the past 3–4 years, there was no gross increase in size of the lesion. On examination, he had a swelling on the medial aspect of the thigh above the knee joint, measuring 8 × 8 cm, non-tender with an irregular surface, and well-defined margins, and it was bony hard in consistency, fixed to the underlying bone (Fig. 1). X-ray findings were suggestive of a bony outgrowth with heterogenous calcification near the femur diaphysis (Fig. 2).
X-ray findings were suggestive of a bony outgrowth with heterogenous calcification near the femur diaphysis (Fig. 2).  Magnetic resonance imaging (MRI) revealed a lesion with an irregular surface, a cartilage cap of 2.5 cm, local invasion into rectus femoris and vastus medialis, and calcific rings and arcs within the lesion on computed tomography (CT) correlation (Figs. 3, 4, 5, 6).
Magnetic resonance imaging (MRI) revealed a lesion with an irregular surface, a cartilage cap of 2.5 cm, local invasion into rectus femoris and vastus medialis, and calcific rings and arcs within the lesion on computed tomography (CT) correlation (Figs. 3, 4, 5, 6). Multiple bilateral centrilobular and subpleural nodules, each <3 mm, were appreciated on high-resolution CT scan, as they are <1 cm, they are non-specific, and not considered to be metastatic in nature. The patient also underwent a positron emission tomography (PET) scan after the surgery, which showed no evidence of metastasis. Later, the patient underwent wide excision and histopathology confirmed the diagnosis of benign osteochondroma (Figs. 7, 8, 9).
Multiple bilateral centrilobular and subpleural nodules, each <3 mm, were appreciated on high-resolution CT scan, as they are <1 cm, they are non-specific, and not considered to be metastatic in nature. The patient also underwent a positron emission tomography (PET) scan after the surgery, which showed no evidence of metastasis. Later, the patient underwent wide excision and histopathology confirmed the diagnosis of benign osteochondroma (Figs. 7, 8, 9).
Osteochondroma is the most common benign bone tumor, accounting for 35% of benign and 8% of all bone tumors [1]. They typically arise from the metaphysis of long bones, most commonly in the distal femur [2]. Predominance is observed in the male population in the growing age group. They may be solitary or multiple lesions, as in the case of multiple hereditary osteochondroma syndrome, which has an autosomal dominant genetic inheritance pattern [5]. Osteochondromas cease to grow after skeletal maturity [7]. Our case had a progressive growth of the tumor mass till the age of 13 years, which was suggestive of its benign nature.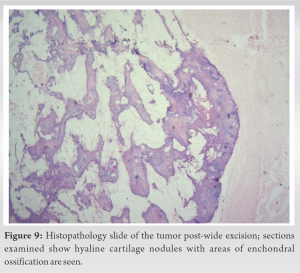
Woertler et al. conducted a MRI pictorial review of 2600 cases with symptomatic osteochondroma and found that a cartilage thickness of 2 cm in adults and 3 cm in children is suspicious of malignant transformation [8]. Stacy et al. in a pictorial essay, found that an increased thickness of the cartilage cap was suggestive of malignant transformation [9]. Ahmed et al. conducted a study on 107 patients suffering from secondary chondrosarcoma arising from osteochondroma. They found an irregularity in the surface, areas of lucency, and inhomogeneous mineralization within the tumor and surrounding soft tissue was characteristic of malignant transformation [10]. Our case exhibited a cartilage cap of <3 cm, irregular surface, invasion of the rectus, and vastus medialis, and on CT correlation, calcific rings and arcs were observed with scattered irregular calcifications.
Hence, in our case, the size of the cartilaginous cap which was <3 cm was indicative of a benign lesion but the rest of the MRI and CT features of the lesion were in favor of malignant transformation making it a borderline case for suspicion of malignancy. The histopathology post-wide excision was indicative of a benign osteochondroma. The patient underwent a PET scan post-surgery and will be on regular follow-up to look for local recurrence or other signs of metastasis.
We report this case due to its rare atypical presentation. Cases like these, characterized by altered radio-pathological correlation, pose a challenge to treat. In such cases, a detailed evaluation and a wide excision of the tumor with biopsy-proven clear margins serve as a prudent next step to rule out malignant transformation.
Osteochondroma is a common benign bone tumor that may undergo malignant transformation into secondary chondrosarcoma. In cases where there is suspicion of malignant transformation, wide excision with biopsy-proven clear margins can be a definite management.
References
- 1.Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar | PubMed]
- 2.Heck KR Jr. Benign bone tumors and neoplastic conditions simulating bone tumors. In: Canale ST, Beaty JH, editors. Campbell’s Operative Orthopaedics. 11th ed. Philadelphia, PA: Mobsy Elsevier; 2007. p. 858-61. [Google Scholar | PubMed]
- 3.Motamedi K, Seeger LL. Benign bone tumors. Radiol Clin North Am 2011;49:1115-34. [Google Scholar | PubMed]
- 4.Alyas F, James SL, Davies AM, Saifuddin A. The role of MR imaging in the diagnostic characterisation of appendicular bone tumours and tumour-like conditions. Eur Radiol 2007;17:2675-86. [Google Scholar | PubMed]
- 5.Garcia RA, Inwards CY, Unni KK. Benign bone tumors-recent developments. Semin Diagn Pathol 2011;28:73-85. [Google Scholar | PubMed]
- 6.Lin PP, Moussallem CD, Deavers MT. Secondary chondrosarcoma. Am Acad Orthop Surg 2010;18:608-15. [Google Scholar | PubMed]
- 7.Wootton-Gorges SL. MR imaging of primary bone tumors and tumor-like conditions in children. Radiol Clin North Am 2009;47:957-75. [Google Scholar | PubMed]
- 8.Woertler K, Lindner N, Gosheger G, Brinkschmidt C, Heindel W. Osteochondroma: MR imaging of tumor-related complications. Eur Radiol 2000;10:832-40. [Google Scholar | PubMed]
- 9.Stacy GS, Heck RK, Peabody TD, Dixon LB. Neoplastic and tumor like lesions detected on MR imaging of the knee in patients with suspected internal derangement: Part I, intraosseous entities. AJR Am J Roentgenol 2002;178:589-94. [Google Scholar | PubMed]
- 10.Ahmed AR, Tan TS, Unni KK, Collins MS, Wenger DE, Sim FH. Secondary chondrosarcoma in osteochondroma: Report of 107 patients. Clin Orthop 2003;411:193-206. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor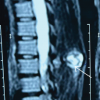 April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity
April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity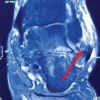 November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report
November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report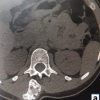 October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling
October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling