
To learn a new technique that serves as an effective option in the management of highly comminuted patella fractures by providing excellent mechanical stability and clinical outcomes.
Dr. Arul Prasanna, Department of Orthopaedics, JJ Arul Hospital, 2/1A2, Dindigul – Madurai NH, Dindigul, Tamil Nadu, India. E-mail: arulprasanna2018@gmail.com
Abstract
Introduction: Comminuted patella fractures pose a challenge to orthopedic surgeons since tension band wiring and cerclage are not effective and often lead to loosening of wires, hardware problems, dislocation of fracture, and failure of osteosynthesis resulting in post-traumatic osteoarthritis and knee stiffness. The aim of this study is to evaluate the clinical outcome in patients with AO 34C2 and 34C3 highly comminuted patella fractures treated with a unidirectional fixed-angle titanium patella locking plate.
Materials and Methods: Twelve patients who presented with AO 34C2 and 34C3 comminuted patella fractures, aged between 18 and 79 years were included in the study. All fractures were reduced and fixed with a unidirectional angle fixed stable titanium patella locking plate. Knee range of motion and knee outcome survey activities of daily living scale were used to evaluate the outcome.
Results: Union of fracture was achieved in all 12 patients. The mean flexion at the final follow-up was 123° (110°–130°). None of the patients had extensor lag. One patient had hardware irritation which resolved at final follow-up.
Conclusion: This technique serves as an effective option in highly comminuted patella fractures by providing excellent mechanical stability resulting in anatomical reduction, excellent functional outcome, and lower incidence of hardware irritation or failure of osteosynthesis.
Keywords: Patella fracture, comminuted, locking plate, osteosynthesis, patellectomy.
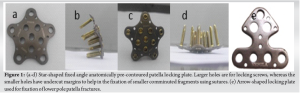
Patella fractures are rare, being 1% of total skeletal fractures [1]. The patella is an important unit of the knee extensor mechanism, playing a pivot role in knee flexion, kneeling, and squatting. Osteosynthesis in comminuted patella fractures is challenging since absolute articular reduction is necessary as incongruency of 2 mm and more, leads to patella-femoral osteoarthritis [2]. Tension band wiring has been a gold standard modality of treatment for transverse patella fractures, but not the optimum treatment in case of comminuted patella fractures for the following reasons (a) tension band wiring requires an intact cortical buttress to convert the tensile forces into compressive forces (b) during healing of fractures, to resist bending, compression, and tension, the fractures need to be accurately reduced and fixed with absolute rigidity to obtain the best possible outcome [3,4] (c) in comminuted fractures, the principle of tension band does not apply in almost all cases (d) tension band wiring does not work during knee extension. All these limitations lead to the development of other modalities of better fixation for comminuted and osteoporotic patella fractures and various plates such as mesh plates, hook plates, and mini plates. In our study, we used a star-shaped unidirectional angle fixed anterior titanium locking plate with multiple suture holes and undercut margins which help in preserving small bony fragments for achieving anatomical reconstruction. These pre-contoured plates recess into the soft tissue, torn retinaculum is repaired onto the plate using sutures which helps in reducing hardware irritation as the patella is subcutaneous (Fig. 1). Only a few studies have been done till now and our study has given comparable results [5].
This prospective observational study was conducted from 2021 to 2023, at an Orthopedic Speciality Hospital. Twelve patients fulfilling the inclusion criteria and giving consent were included in the study. The aim of the study was to analyze the functional and radiological outcome of comminuted patella fracture fixed with a locking plate.
Inclusion criteria
(1) Age 18–79 years, (2) AO 34C2 and 34C3 comminuted patella fractures with displacement and articular incongruency, and (3) fractures <3 weeks old were included in the study.
Exclusion criteria
(1) Ipsilateral lower limb fractures around the knee, (2) open wound, (3) anterior knee soft-tissue defects, and (4) patella fractures post-total knee replacement were excluded from the study.
Technique
A standard midline longitudinal approach was used, raising a thick soft-tissue flap to make sure the plate was covered adequately. Usually, a 2-cm lateral or medial arthrotomy was done to clinically palpate the articular reduction. The fracture edges were carefully exposed, minimizing unnecessary periosteal dissection to maximize perfusion and keep soft-tissue attachments to comminuted fragments. The fracture site was carefully debrided of non-viable tissue and any small fragments that could not be incorporated into the reduction were removed and saved for possible bone grafting. Fragment reduction and compression of major fragments, through clamp application, must be performed first, when possible, before plate application. The reduction was then secured using k wires, following which an appropriate size star-shaped locking plate was chosen according to the size of the patella and fracture pattern (Fig. 2).

The unidirectional angle fixed titanium locking plate by Nebula (from India) (3.5 mm screw system) was used in all patients. It has suture holes to fix the comminuted small bony fragments to the plate using non-absorbable braided suture (Fig. 3). Once fixation with locking screws was completed, a finger was passed through the lateral arthrotomy to check for any breach of the articular surface by screws. Intraoperative anteroposterior, lateral, and skyline fluoroscopy views were taken to ensure articular congruency and anatomical reduction (Fig. 4). Knee range of motion was performed to ensure stable fixation.

Over the course of 2 years, 80 patients presented with patella fractures at our center, out of which 12 patients had comminuted patella fractures. Informed consent was obtained from 12 patients and who were included in the study. Out of 12 patients, One was female and 11 were male. The average age was found to be 42 years. The average time of follow-up was 1.2 years. Out of 12 patients, all 12 (100%) achieved union. One patient (8%) had anterior knee pain and difficulty while kneeling due to implant impingement. No elective implant removal was done. One patient (25/Male) had suffered a transverse patella fracture, which was fixed using standard tension band wiring, following which he again suffered a fall to the same knee 2 weeks postoperatively, which had resulted in failure of tension band wiring and comminution of the fracture fragments (Fig. 5a and b). The tension band wiring was removed, the fracture was reduced and fixed using a star-shaped patella plate, which had gone onto the united well (Fig. 5g-l), and achieved knee flexion of 130° without any extensor lag at 1-year follow-up (Fig. 6).


During follow-up, all the patients had full recovery of the extensor mechanism. The mean flexion achieved was 123° (110–130°), six patients achieved knee flexion of 120°, whereas five patients achieved 130° of knee flexion (Fig. 7 and 8). Almost all patients were able to sit cross-legged except one patient with pre-existing medial compartment osteoarthritis.


The influence of symptoms on daily activity is shown in Table 1 and the functional outcome in Table 2, both of which had been evaluated using the knee outcome survey activities of daily living (ADL) scale.


No patient had severe disability in daily activity (Table 1) and the functional outcome of the patient was also well acceptable (Table 2). Eleven out of 12 (92%) patients were pain-free or slightly affected by pain in daily activity. Eleven out of 12 (92%) did not have knee stiffness. Ten out of 12 (83%) did not have a problem in walking. One out of 12 (8%) patients had difficulty in kneeling on the front. None had difficulty in standing. One patient with a pre-existing Medial Compartment had some restrictions in daily activity. The average ADL score was 86%, which means the function of the patient’s knee in daily life returned to an average of 97% to their function before trauma.
Scoring
Each row has a maximum of 5 points and the lowest of 0 points, 5 being given to the best outcome and 0 to the worst. The first column scored 5 points, followed in successive columns by scores of 4, 3, 2, 1, and 0 for the last column. The total points for all patients were calculated which came out to be 818, and then divided by 70 (maximum points for the individual patient) *12 (total number of patients in the study). The average ADLS score calculated was 818/(70 × 12) × 100 = 97% (Table 3).
In this study, we have done a prospective functional analysis of comminuted patella fractures using fixed angle titanium patella locking plate and compared it with the available relevant date of tension band wiring. Tension band wiring tends to fail in comminuted patella fractures, as it requires an intact cortical buttress [6,7]. In our study, using an anatomically pre-contoured locking plate, we were able to achieve union in all our cases. Dy et al. in their meta-analysis reported a reoperation rate of 34% post-tension band wiring compared to 5% in the locking plate group. Smith et al. observed that almost 22% of patients treated with tension band wiring suffered from displacement in the perioperative period, which was overcome by the use of a more rigid construct such as a locking plate [8,9]. Biomechanical studies by Wurm et al. [10] and cadaveric studies by Thelen et al. [11,12] have proved the superiority of locking plates to tension band wiring. This has enabled early rehabilitation protocol and prevention of knee stiffness which occurs with tension band wiring. Our recommended post-operative protocol is to start weight bearing immediately as tolerated, passive knee flexion of up to 90° with brace support for the first 2 weeks, and then 120° passive to active assisted knee flexion over the next 4 weeks. Tension band wiring in comminuted fracture results in wire breakage, failure to achieve absolute stability, and failure to achieve articular congruity [13,14,15,16] which can be overcome by a Patella locking plate which maintains compression and provides a rigid construct. Partial and complete patellectomy leads to a poor extensor mechanism, especially in younger populations, and also issues while performing total knee replacement at a later stage. Our surgical technique allows direct clinical visualization of the articular surface which avoids the development of patella-femoral joint arthritis which leads to better outcomes. In our study, a good functional recovery of range of motion was observed, with 123° as an average and 11 patients achieving more than 120° of knee flexion. Only one patient had a knee flexion of 110° due to pre-existing Patello-femoral osteoarthritis and medial compartment osteoarthritis. Most of the patients were symptom-free, only one patient had pain which affected his daily activity slightly, the reason being pre-existing knee osteoarthritis. One patient had pain while kneeling, but improved with activity modification. This pain may be attributed to the scar of the wound rather than the implant itself. Wurm et al. [5] had done a similar study in Germany, using a similar plate, which included patients with periprosthetic patella fracture and failed tension band wiring, in which they had achieved a range of motion of 127° and complication rate of 6%. The average ADL score in their study was 77% as compared to 97% in our study. The results are almost reproducible in the Indian population, except for a better outcome in our study. They had a lesser ADL score as they had a larger proportion of patients who had undergone multiple surgeries resulting in larger anterior scar (Table 4).

Singh et al. [17] conducted a similar study in the Indian population, using a fixed angle locking plate, among 20 displaced, osteoporotic patella fractures, with excellent outcome, with mean flexion of 124° and average ADL score of 86%, comparable to our study. The advantages of plating over tension band wiring, cerclage, and patellectomy in comminuted patella fractures are preserving maximum bone stock while achieving anatomical reduction and stable fixation, which is important for normal quadriceps excursion. It has minimum wound problems, less hardware failure, lesser hardware irritation, reduced incidence of knee stiffness due to early rehabilitation, and better articular reduction.
The disadvantages include:
- Penetration of screws intra-articularly if not cautious
- Hardware cost.
Limitations
This was a prospective cross-sectional analytical study and a direct comparison of the patella plate fixation with other modalities of treatment was not done. This study had a small sample size; further studies with a bigger sample size and comparison with other modalities will aid in providing better comparative results.
Based on our study, we conclude that angle fixed patella locking plate is an optimum modality of fracture fixation in comminuted patella fractures and in cases of failed tension band wiring as it is a more bone-preserving implant which provides excellent mechanical stability and anatomical reduction leading to excellent functional outcome and decreased incidence of hardware irritation or failure of osteosynthesis. The better biomechanical strength has helped patients in early rehabilitation and early return to their daily lives.
Treating comminuted patella fractures have always been a challenge. This technique proves to be an effective option in managing them and also obtaining good clinical and functional outcomes.
References
- 1.Wild M, Windolf J, Flohé S. Fractures of the patella. Unfallchirurg 2010;113:401-11; quiz 412. [Google Scholar | PubMed]
- 2.Boström A. Longitudinal fractures of the patella. Reconstr Surg Traumatol 1974;14:136-46. [Google Scholar | PubMed]
- 3.Labitzke R. Zuggurtungen-richtiges und falsches am beispiel der patellafraktur. Chirurg 1997;68:638-42. [Google Scholar | PubMed]
- 4.AO Principles of Fracture Management. Available from: https://www.thieme.com/books-main/orthopaedic-surgery/product/4437-ao-principles-of-fracture-management [Last accessed on 2020 Jul 07]. [Google Scholar | PubMed]
- 5.Wurm S, Bühren V, Augat P. Treating patella fractures with a locking patella plate-first clinical results. Injury 2018;49 Suppl 1:S51-5. [Google Scholar | PubMed]
- 6.Matthews B, Hazratwala K, Barroso-Rosa S. Comminuted patella fracture in elderly patients: A systematic review and case report. Geriatr Orthop Surg Rehabil 2017;8:135-44. [Google Scholar | PubMed]
- 7.Böstman O, Kiviluoto O, Nirhamo J. Comminuted displaced fractures of the patella. Injury 1981;13:196-202. [Google Scholar | PubMed]
- 8.Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7. [Google Scholar | PubMed]
- 9.Dy CJ, Little MT, Berkes MB, Ma Y, Roberts TR, Helfet DL, et al. Meta-analysis of re-operation, nonunion, and infection after open reduction and internal fixation of patella fractures. J Trauma Acute Care Surg 2012;73:928-32. [Google Scholar | PubMed]
- 10.Wurm S, Augat P, Bühren V. Biomechanical assessment of locked plating for the fixation of patella fractures. J Orthop Trauma 2015;29:e305-8. [Google Scholar | PubMed]
- 11.Thelen S, Schneppendahl J, Jopen E, Eichler C, Koebke J, Schönau E, et al. Biomechanical cadaver testing of a fixed-angle plate in comparison to tension wiring and screw fixation in transverse patella fractures. Injury 2012;43:1290-5. [Google Scholar | PubMed]
- 12.Thelen S, Schneppendahl J, Baumgärtner R, Eichler C, Koebke J, Betsch M, et al. Cyclic long-term loading of a bilateral fixed-angle plate in comparison with tension band wiring with K-wires or cannulated screws in transverse patella fractures. Knee Surg Sports Traumatol Arthrosc 2013;21:311-7. [Google Scholar | PubMed]
- 13.Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg 2011;19:198-207. [Google Scholar | PubMed]
- 14.Wild M, Khayal T, Miersch D, Windolf J, Hakimi M. Die zuggurtungsosteosynthese nach patellafraktur. Unfallchirurg 2008;111:892-7. [Google Scholar | PubMed]
- 15.Choi HR, Min KD, Choi SW, Lee BI. Migration to the popliteal fossa of broken wires from a fixed patellar fracture. Knee 2008;15:491-3. [Google Scholar | PubMed]
- 16.Suh KT, Suh JD, Cho HJ. Open reduction and internal fixation of comminuted patellar fractures with headless compression screws and wiring technique. J Orthop Sci 2018;23:97-104. [Google Scholar | PubMed]
- 17.Singh S, Surana R, Rai A, Sharma D. Outcome analysis of fixed angle locking plate in patella fractures: A single centre experience from North India. Indian J Orthop 2020;55:655-61. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function July 1, 2026 Traumatic Case of Comminuted, Shattered Navicular Bone Fracture: A Rare Case of Midfoot Catastrophe
July 1, 2026 Traumatic Case of Comminuted, Shattered Navicular Bone Fracture: A Rare Case of Midfoot Catastrophe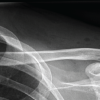 March 1, 2026 Distal Clavicle Refracture after All-Suture Double Coracoclavicular and Acromioclavicular Stabilization: A Case Report
March 1, 2026 Distal Clavicle Refracture after All-Suture Double Coracoclavicular and Acromioclavicular Stabilization: A Case Report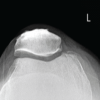 March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report
March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report