
Hematomas that develop acutely or gradually in the gluteal region in patients who have undergone surgery for intertrochanteric fractures with cephalomedullary nails should serve as a reminder to surgeons of the potential injury and pseudoaneurysm of the superior gluteal artery.
Dr. Furkan Başak, Department of Orthopedics and Traumatology, Umraniye Training and Research Hospital, Istanbul, Turkey. E-mail: furbasacu@gmail.com
Abstract
Introduction: Superior gluteal artery (SGA) injury is an uncommon, yet critical complication associated with trochanteric fracture surgery. While deep femoral artery branches are more frequently affected, SGA involvement is infrequent but potentially life threatening. Knowledge of anatomy plays a crucial role in reducing the likelihood of such complications. Factors contributing to deep femoral artery injury include direct trauma from fracture fragments, excessive drilling, or inadvertent arterial damage during instrumentation. To date, only a few cases have reported SGA injuries following trochanteric fracture surgery. In this study, we report a late presented SGA pseudoaneurysm after intramedullary nailing of intertrochanteric fracture.
Case Report: A 72-year-old female with a right intertrochanteric fracture underwent surgery involving the placement of a short cephalomedullary nail. In the 3rd week postoperatively, the patient presented with a sizable hematoma near the proximal and posterior section of the incision. Subsequent investigations unveiled a pseudoaneurysm in the SGA as the source of the hematoma and declining hemoglobin levels. The pseudoaneurysm was successfully treated with embolization, and the patient recovered without complications.
Conclusion: Prompt recognition of post-operative hemoglobin decrease, regardless of clinical symptoms, is essential. Computed tomography angiography is valuable for early detection and intervention of SGA injuries. Surgeons must be careful when opening the incision and determining the entry point, as anterior incision and medialized guidewire may increase the risk of SGA injury. Awareness of this rare complication and its management is vital to prevent possible complications.
Keywords: Intertrochanteric fracture, fixation, ıntramedullary nail, superior gluteal artery, complication, pseudoaneurysm.
Hip fractures are common injuries, particularly among elderly individuals with osteoporosis, accounting for approximately 8–10% of all fractures [1]. In the United States, it is estimated that around 300,000 patients are hospitalized annually due to hip fractures, and this number is projected to increase [2]. While surgical options are commonly preferred for the treatment of intertrochanteric femur fractures with high potential for union, the proximal femoral nail is the most frequently chosen method [3,4]. The ease of application and improved stability provided by proximal femoral nailing are among the reasons for its preference [3]. Iatrogenic complications can occasionally arise during surgeries for intertrochanteric femur fractures with short intramedullary (IM) femoral nails. These complications may include malalignment and damaging surrounding soft tissues, nerves, or blood vessels. In some cases, complications like hematoma formation or infection at the surgical site can occur postoperatively. Although rare, superior gluteal artery (SGA) injury associated with proximal femoral nailing poses a life-threatening complication [5]. If not detected promptly, it can lead to complications such as hemorrhagic shock, gluteal compartment syndrome, and necrosis, all of which pose significant risks to the patient’s life [6,7]. To mitigate these risks, meticulous surgical technique, careful pre-operative planning, and vigilant post-operative monitoring are crucial to ensure the best possible outcomes for patients undergoing surgery for intertrochanteric femur fractures with short IM femoral nails. In this report, we present a case of a patient who underwent surgery for an intertrochanteric femur fracture and subsequently developed SGA injury.
A 72-year-old female patient presented to our emergency department with an inability to walk following a fall at home, resulting in a displaced fracture of the right femur. Physical examination and X-ray imaging confirmed a diagnosis of an Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association type 31; A2.2 [8]. Right intertrochanteric femur fracture and surgical intervention were recommended (Fig. 1a). The patient had a known history of hypertension. A pre-operative routine single dose of anticoagulant regimen, including 0.4 mg of low molecular weight heparin, was initiated.
Preoperative laboratory findings showed hemoglobin level of 9.3 g/dL, hematocrit (Hct) of 30.3% and an international normalized ratio of 1.16. On the 3rd day of hospitalization, the patient underwent surgery, which was performed using a traction table. A 3–5 cm incision was made approximately 4 cm proximal to the greater trochanter. After blunt dissection of the abductors, a guidewire was inserted from the major trochanter. Only the nail entrance at the greater trochanter was reamed using a 14 mm reamer. An 11/220 mm diameter nail (PROFIN®, TST Ind., Istanbul, Turkey) was introduced over the guide wire. Proximal fixation was achieved with 8.5 × 100 and 8.5 × 95 mm two lag screws, and distal fixation with a 5.0 × 36 mm screw (Fig. 1b). After achieving hemostasis and conducting fluoroscopy checks, the procedure concluded. Postoperative laboratory assessments at 12 h post-operation revealed a hemoglobin level of 5.6 g/dL and Hct of 18.1%. Due to the low hemoglobin level, two units of blood were transfused. Subsequent blood tests indicated a post-transfusion hemoglobin level of 8.9 g/dL and Hct of 26.9%. On the 1st postoperative day, hemoglobin measured 8.8 g/dL and Hct was 26.5 g/dL. To address a further decline in hemoglobin level (8.2 g/dL) and Hct (25.6%) on the same day in the evening, an additional unit of blood was transfused. Subsequent hemoglobin and Hct levels during follow-up were 9.6 g/dL and 26.3%, respectively. Minimal discharge was observed during wound dressings on the 1st post-operative day, and no discharge occurred on the 2nd and 3rd days. The patient was instructed to perform physiotherapy exercises. With a clean wound and normal blood parameters, the patient was discharged with a prescription that included 0.4 mg of low molecular weight heparin, oral ferritin, paracetamol, and a proton pump inhibitor.

On the 20th day after the post-operative period, the patient visited the clinic for routine checkups, revealing a 10 × 8 cm hematoma in the right gluteal region (Fig. 2). The hematoma had formed over the past 2 days. The patient’s hemoglobin (Hb) level measured 8.9 g/dL, and Hct was 28.4. The patient was readmitted to the ward for further monitoring. A superficial ultrasound was scheduled to assess the mass in the gluteal region, revealing a hematoma measuring 90 × 40 mm. On the 2nd day of hospitalization, Hb levels further declined to 8.7. With Hb dropping to 6.7 on the 3rd day, a blood transfusion was planned, and subsequent Hb levels reached 8.4. The patient consulted with the vascular surgery department, leading to the decision to perform computed tomography (CT) angiography. Results indicated a pseudoaneurysm formation near the nail entrance point. Consequently, an angiography was scheduled to embolize the pseudoaneurysm. During the angiography performed by the interventional radiology team, they identified an injury to the SGA, resulting in a pseudoaneurysm. The pseudoaneurysm was successfully treated by coiling and was located in one of the inferior recurrent divisions of the superior branch of the SGA (Fig. 3).
Following embolization, the patient’s condition remained stable, with an increase in hemoglobin levels. Low molecular weight heparin was prescribed again to prevent deep vein thrombosis. Full weight bearing was allowed, and the patient was subsequently discharged. Subsequent post-operative follow-ups showed stable hemoglobin levels and a reduction in the size of the hematoma over time (Fig. 4).
Vascular injuries associated with trochanteric fractures are quite rare [9,10]. Frequently seen at the branches of the deep femoral artery (71.41%), whereas the involvement of the SGA (9.8%) is rarer [10]. Several factors play a role in the injury of the femoral artery, these include direct injury to the artery by fracture fragments, damage due to excessive drilling, or arterial injury during the placement of retractors [10,11]. SGA injuries associated with trochanteric fracture surgery are exceptionally rare, with only four reported cases to date [4,5,9,12]. In the case presented by Ward et al. [9], a patient with a subtrochanteric fracture underwent IM nail (IMN) fixation, and a decrease in hemoglobin levels was noted from the 1st post-operative day. Ward et al. emphasized that nail entry points could cause arterial injuries and improper positioning of guidewires might result in SGA injuries. Ailaney et al. [5]. operated on a patient with an atypical intertrochanteric fracture due to alendronate use, and their patient also experienced a decrease in hemoglobin levels from the 1st post-operative day. Ailaney et al. concluded that suspicion of SGA injury should be considered when there is a post-operative decrease in hemoglobin levels, even in the absence of clinical symptoms. Fernandes et al. [12]. reported a similar case involving an SGA injury in a patient treated for an intertrochanteric fracture with an IMN. In this instance, the patient also experienced a significant and abnormal decline in hemoglobin levels during the 1st post-operative week. However, the authors suggested that the injury occurred due to the use of a scalpel in the proximal incision area instead of employing blunt dissection. Carrol et al. [4]., presenting a similar case, reported a pseudoaneurysm of the deep branch of the SGA and attributed the injury to the position of the guidewire. Our case differed from previous cases in several ways. First, while in previous cases, the injured artery was the inferior (or deep) branch of the SGA, in our case, it was an inferior recurrent division arising from the superior branch of the SGA. As indicated by Fernandes et al. [12], the orientation of the guidewire cannot be the sole reason for the injury. In our case, the dissection was performed using a blunt technique, and a scalpel was not utilized. However, the incision was positioned too anterior and proximal. Therefore, to gain a better view of the trochanter major, excessive posterior traction with retractors may have caused the injury. Furthermore, although there was an acute decrease in hemoglobin levels in our case, similar to previous cases, hemoglobin levels could be corrected with transfusions, and the patient was discharged, as in the case of Ward et al. [9]. Bleeding from the injured vessel might have diminished or stopped after the initial injury, possibly due to clot formation. However, it could have resumed upon patient mobilization, likely due to clot dislodgment [9]. This finding suggests that the use of low-molecular weight heparin cannot be implicated in pseudoaneurysm formation. Post-operative unexpected large hemoglobin decrease should be taken into account [13]. The stability of hemoglobin levels in the early post-operative period does not necessarily rule out the presence of an SGA injury. Even a patient who experiences a decrease in hemoglobin levels on the 10th day postoperatively may have encountered such an injury [10]. This is particularly significant when edema and ecchymosis appear in the gluteal region alongside a reduction in hemoglobin; in such cases, the possibility of an arterial injury should not be dismissed. Furthermore, it’s essential for surgeons to consider the potential for injury to the SGA when hematomas develop suddenly or gradually in the gluteal region in patients who have undergone surgery for intertrochanteric fractures with short cephalomedullary nails. Unnecessary attempts to evacuate the hematoma can result in uncontrolled bleeding from a pseudoaneurysm, putting the patient’s life at risk. Initially, the diagnosis for the current case pointed to a hematoma caused by low molecular weight heparin, and plans were made for hematoma evacuation following the cessation of LMWH. However, a rapid decrease in hemoglobin levels on the 3rd day at the second admission prompted reconsideration of a vascular injury. It is crucial to understand that bleeding from a small-caliber vessel may not lead to intraoperative hemorrhage, rapid hematoma formation, lower extremity ischemia, loss of peripheral pulses, or an immediate significant drop in hemoglobin () levels. Instead, one should anticipate gradual decreases in hemoglobin levels and the gradual development of hematomas [5]. Subsequent analyses and consultations revealed the presence of a pseudoaneurysm in the SGA.
SGA pseudoaneurism after IM nailing of pertrochanteric fracture is a rare complication encountered in the surgical treatment of trochanteric fractures. Although it is a rare complication, it can be life threatening. Proper determination of the incision line and careful identification of the guide wire entry point reduces the likelihood of complications. In patients with post-operative hemoglobin decrease, even in the absence of clinical findings, the possibility of SGA injury should be considered, and CT angiography should not be avoided. It should be considered that SGA injury may have occurred in patients who develop post-operative hematoma and are accompanied by hemoglobin decrease, and invasive procedures should not be rushed.
Development of SGA injury is a rare but potentially life-threatening complication in trochanteric fracture surgery. Understanding the anatomy and carefully determining the incision line with cautious dissection can reduce the risk.
References
- 1.Kömür B, Kaan E, Yilmaz B, Özdemir G, Duymuş T. Evaluation of gamma nails in intertrochanteric fractures of femur and modified technique for removal. Open Access Library J 2015;2:1-6. [Google Scholar | PubMed]
- 2.Kannus P, Parkkari J, Sievänen H, Heinonen A, Vuori I, Järvinen M. Epidemiology of hip fractures. Bone 1996;18:57-63. [Google Scholar | PubMed]
- 3.Niu E, Yang A, Harris AH, Bishop J. Which fixation device is preferred for surgical treatment of intertrochanteric hip fractures in the United States? A survey of orthopaedic surgeons. Clin Orthop Relat Res 2015;473:3647-55. [Google Scholar | PubMed]
- 4.Carroll C, Warren M, Nammour M, Taillac H, Mautner J. Superior gluteal artery bleed after cephalomedullary nail. Ochsner J 2020;20:339-42. [Google Scholar | PubMed]
- 5.Ailaney N, O’Connell R, Giambra L, Golladay G. Superior gluteal artery pseudoaneurysm following. Intramedullary nailing of an atypical femoral fracture. BMJ Case Rep 2019;12:e231490. [Google Scholar | PubMed]
- 6.Gee MJ, Tolat A, Sinha J. Syndrome following pelvic fracture and superior gluteal artery bleed. Eur J Trauma Emerg Surg 2007;33:188-91. [Google Scholar | PubMed]
- 7.Zhang Q, Chen W, Smith WR, Pan J, Liu H, Zhang Y. Superior gluteal artery injury presenting as delayed onset shock. Arch Orthop Trauma Surg 2010;130:251-6. [Google Scholar | PubMed]
- 8.Fracture and Dislocation Compendium. Orthopaedic trauma association committee for coding and classification. The orthopedic trauma association classification of fractures. J Orthop Trauma 1996;10 Suppl 1:v-ix, 1-154. [Google Scholar | PubMed]
- 9.Ward JP, Strauss EJ, Tejwani NC. Injury to the superior gluteal artery during intramedullary fixation of an atypical subtrochanteric stress fracture-a case report. Bull Hosp Jt Dis (2013) 2013;71:297-300. [Google Scholar | PubMed]
- 10.Barquet A, Gelink A, Giannoudis PV. Proximal femoral fractures and vascular injuries in adults: Incidence, aetiology and outcomes. Injury 2015;46:2297-313. [Google Scholar | PubMed]
- 11.Yoon HK, Oh HC, Park J, Oyunbat C, Kim T. Rupture of the deep femoral artery during proximal femoral Nailing following an intertrochanteric fracture: A case report. Hip Pelvis 2016;28:54-9. [Google Scholar | PubMed]
- 12.Fernandes PX, Medeiros DM, Teixeira RC, Nunes AM, Seco AS, Caetano AC. Injury to the superior gluteal artery during intramedullary fixation of a proximal femoral fracture-a case report. J Orthop Case Rep 2019;9:27-31. [Google Scholar | PubMed]
- 13.Lazarides MK, Arvanitis DP, Dayantas JN. Latrogenic arterial trauma associated with hip joint surgery: An overview. Eur J Vasc Surg 1991;5:549-56. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report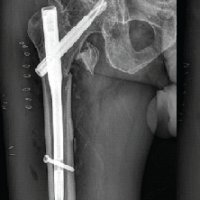 September 1, 2025 A Rare Case of Pseudoaneurysm of Profunda Femoris Artery Following Surgical Fixation of an Intertrochanteric Fracture
September 1, 2025 A Rare Case of Pseudoaneurysm of Profunda Femoris Artery Following Surgical Fixation of an Intertrochanteric Fracture August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study
August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study