
Motorcycle Wheel spoke injuries pose a serious source of complex foot and ankle injuries leading to long-term debilitating deformities. We recommend rigorous public education and awareness creation to forestall the rising trend of these preventable injuries.
Dr. Alexis D B Buunaaim, Department of Surgery, School of Medicine, University for Development Studies, Tamale, Ghana/Trauma and Orthopedic Department, Tamale Teaching Hospital, Post Office Box TL16, Tamale, Ghana. E-mail: abuunaaim@yahoo.co.uk
Abstract
Introduction: Motorcycle wheel spoke injuries refer to the entrapment of the foot and ankle of a rider or pillion rider into the spokes of a vehicle resulting in varied complex ankle-foot injuries.
Case Reports: We report 10 cases of motorcycle wheel spoke injuries between January 01, 2022, and December 31, 2023, the majority of whom were children with the youngest being 4 years and the oldest 43 years. A few of the cases sustained both soft-tissue injuries and bony injuries (fractures) around the ankle while the rest sustained only soft-tissue injuries. We believe a lot more of these cases do not get to the tertiary facility for varied reasons. The mean length of hospital stay was 19 ± 13 days with a potential indirect negative economic impact on the state, patients, and their families. These injuries can be prevented by developing policies aimed at public education, baring children from riding pillion, and designing protective wheel covering.
Conclusion and Recommendation: Cases of motorcycle wheel spoke injuries are on the rise in the Northern part of Ghana. We recommend public education and awareness creation as well as stringent implementation of road traffic regulations in Northern Ghana .
Keywords: Wheel spoke, injury, Achilles, Northern Ghana.
Motorcycle road traffic accidents are a significant contributor of morbidity and mortality in Ghana. A good proportion of the mechanism of motorcycle accidents involves the entrapment of the foot and ankle of riders into the wheel spokes of the motorcycle termed wheel spokes injuries (WSI) [1]. The ascendency of these injuries in some parts of the world has been attributed to inadequate safety protocols and children being the main victims [2]. The spectrum of WSI ranges from minor soft-tissue lacerations to extensive crush injury with tendon and bony involvement to subtotal amputations, mainly involving the heel and ankle sites [2]. Few single-center studies attempted to address the occurrence of motorcycle WSIs in both developed and developing nations. Chiang et al. reported that 50% of all injuries in Singapore occur among motorcycle riders and their pillion riders [3]. A similar study in Anambra state, Nigeria found 41.4% of participants sustaining injuries from motorcycle accidents out of which 10.3% had wheel spokes entrapment injuries [4]. These preventable injuries exert enormous pressure on the resources of patients, their immediate families, healthcare institutions, and governments. Despite these untoward effects, there is however a paucity of literature about this type of preventable injuries caused by motorcycle wheel spokes mostly in developing countries. As a result, this case series is aimed at creating awareness of the increasing number of these injuries and the need for policy orientation on education and preventive strategies to help curb this rising threat in our society.
Case 1
A 43-year-old male motorcycle rider presented with an 8-h duration of painful deformity at the left ankle with a laceration exposing bony fragments and inability to bear weight. He lost control of his motorcycle while attempting to avoid a head-on collision with an oncoming truck which veered onto his lane and got his left foot and ankle entrapped in the spokes of the front wheel. There was no initial loss of consciousness. Physical examination revealed a painful deformity of the left ankle with a laceration posteriorly showing exposed bone fragments and a positive Thompson test. Foot and ankle radiographs revealed a fracture dislocation of the left ankle with bimalleolar fractures (Fig. 1). Intraoperative assessment showed loss of distal 2 cm of the left fibular and a transverse medial malleolar fracture as well as a torn anterior part of the joint capsule. Serial debridement and left ankle spanning external fixation were done with the repair of the Achilles tendon. Wound coverage was subsequently achieved with a split-thickness meshed skin grafting. Follow-up 12 weeks later showed the wound healed completely and fractures united satisfactorily with no equinus deformity, ankle dorsiflexion of 20° from plantigrade position, and plantarflexion of 25° from plantigrade position (Fig. 2).
Intraoperative assessment showed loss of distal 2 cm of the left fibular and a transverse medial malleolar fracture as well as a torn anterior part of the joint capsule. Serial debridement and left ankle spanning external fixation were done with the repair of the Achilles tendon. Wound coverage was subsequently achieved with a split-thickness meshed skin grafting. Follow-up 12 weeks later showed the wound healed completely and fractures united satisfactorily with no equinus deformity, ankle dorsiflexion of 20° from plantigrade position, and plantarflexion of 25° from plantigrade position (Fig. 2).
Case 2
An 8-year-old male was the first of two pillion motorcycle riders en route to school when his left foot got trapped in the rear spokes of the motorcycle sustaining an avulsion of the left heel and partial laceration of the left Achilles tendon. Physical assessment revealed avulsion of the left heel and partial laceration of the left Achilles tendon with a negative Thompson test. The posterior tibialis pulse was not palpable but the dorsalis pedis was palpable and comparable to the contralateral side (Fig. 3). The wound was debrided serially and 20% laceration of the Achilles tendon and the wound was dressed serially until granulation tissue was healthy and a split-thickness skin graft was done. The patient was nursed for 15 days on admission and subsequently discharged. The patient has since not reported back for follow-up.
The wound was debrided serially and 20% laceration of the Achilles tendon and the wound was dressed serially until granulation tissue was healthy and a split-thickness skin graft was done. The patient was nursed for 15 days on admission and subsequently discharged. The patient has since not reported back for follow-up.
Case 3
A 10-year-old male was returning home from school as a pillion rider. His left foot accidentally got trapped into the spokes of the rear wheel of the motorcycle sustaining a laceration at the posterior aspect of the left ankle with exposed tendon fascicles and a painful deformity of the distal leg and an inability to bear weight. On physical assessment, the left foot and ankle were swollen with a laceration of the Achilles tendon. Thompson’s test was positive. Posterior tibialis and dorsalis pedis pulses were palpable and comparable to the contralateral side. Radiographs of the left foot, ankle, and tibia showed a greenstick distal tibia fracture (Fig. 4). The patient underwent serial wound debridement and a delayed primary Achilles tendon repair and wound coverage with a split-thickness skin graft. The left foot was immobilized in planter flexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. Follow-up at 1 year after surgery showed that the wound healed completely and fractures united satisfactorily (Fig. 5) without equinus deformity, ankle dorsiflexion of 20° from plantigrade, and plantarflexion of 35° from plantigrade.
Case 4
A four-year-old male presented with an avulsion of the posterior aspect of the sole of the left foot. He was the first of two pillion riders en route to a peripheral health facility on account of developing a fever. The motorcycle rider hit a pothole and lost control resulting in the entrapment of the left foot of the patient in the rear spokes of the motorcycle. Physical assessment revealed a partial avulsion of the sole of the left hind foot with a distally placed base. Posterior tibialis pulse was not palpable but the dorsalis pedis was palpable and comparable to the contralateral foot. Thompson’s test was positive. Radiographs of the left foot and ankle showed a fracture of the calcaneus (Fig. 6). Serial debridement and fixation of the calcaneal fracture with Kirchner wire were done. The wound was serially dressed under sterile conditions till healthy granulation tissue developed. A split-thickness skin graft was subsequently done to cover the wound. Follow-up at 1 year revealed scar tissue at the heel. The ankle had an equinus deformity at 10° from plantigrade, dorsiflexes from 10° equinus to 10° and plantarflexes from 10° to 15° (Fig. 7).
Case 5
Nine-year-old male motorcycle pillion rider whose right foot and ankle got trapped in the spokes of the rear wheel. He sustained a laceration at the posterior aspect of the right ankle with exposed tendon fascicles and an inability to plantarflex. Physical assessment revealed an irregular laceration involving the right Achilles tendon about 3 cm from its point of attachment to the calcaneus. Thompson’s test was positive. Posterior tibialis and dorsalis pedis pulses were palpable and comparable to the contralateral side (Fig. 8). Radiographs of the right foot and ankle were unremarkable. The patient underwent serial wound debridement and a delayed primary Achilles tendon repair. The right foot was immobilized in plantarflexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. Wound coverage was achieved by split-thickness skin graft. Follow-up in a year showed a healed wound with minimal scar tissue and the ankle in plantigrade (Fig. 9). There are no functional deficits noted.
Case 6
Seven-year-old female pillion rider of a motorcycle whose right foot and ankle got trapped in the spokes of the rear wheel. She sustained a laceration at the posterolateral aspect of the right ankle with the ability to plantarflex. Physical assessment revealed a laceration involving the left Achilles tendon about 2 cm from its point of attachment to the calcaneus. Thompson’s test was negative. Posterior tibialis and dorsalis pedis pulses were palpable and comparable to the contralateral side (Fig. 10). Radiographs of the right foot and ankle were unremarkable. The patient underwent serial wound debridement and primary wound closure. The patient was nursed 8 days on admission and subsequently discharged and has since not reported back for follow-up.
Case 7
Eleven-year-old female pillion rider of a motorcycle whose left foot and ankle got trapped in the spokes of the rear wheel after hitting a speed ramp. She sustained an avulsion at the posterior aspect of the left ankle with exposed tendon fascicles and an inability to plantarflex. Physical assessment revealed an irregular partial avulsion involving the left Achilles tendon at the posterior part of the left ankle with a distally based flap. Thompson’s test was positive. Posterior tibialis and dorsalis pedis pulses were palpable and comparable to the contralateral side (Fig. 11). Radiographs of the right foot and ankle were unremarkable. The patient underwent serial wound debridement and a delayed primary Achilles tendon repair and wound coverage achieved by primary closure. The left foot was immobilized in planter flexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. The wound satisfactorily healed with no equinus deformity and no functional deficits (Fig. 12) at 12-month follow-up.
Case 8
An 8-year-old male who presented with a 2-h duration of a laceration at the posterior aspect of the right ankle following an entrapment of his right foot and ankle in the rear spokes of the motorcycle. An irregular transverse laceration involving the Achilles tendon is associated with bleeding. Physical examination showed an irregular laceration involving the right Achilles tendon with a positive Thompson test (Fig. 13). Radiographs of the foot, ankle and distal tibia, and fibular were unremarkable. Serial wound debridement and delayed Achilles tendon repair was done, and wound coverage was achieved with a split-thickness skin graft. The right foot was immobilized in plantarflexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. The patient has since not reported back for scheduled follow-up reviews.
Case 9
The 9-year-old male appeared well till about an hour before presentation when his left foot and ankle got entrapped in the rear spokes of the motorcycle as a pillion rider, sustaining a laceration at the posterior aspect of the left ankle. Examination showed an irregular laceration involving the left Achilles tendon with a positive Thompson test (Fig. 14). Radiographs of the foot and ankle were unremarkable. Serial wound debridement and delayed Achilles tendon repair were carried out and wound coverage was achieved with a split-thickness skin graft. The left foot was immobilized in planter flexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. The patient has since not reported back for scheduled follow-up reviews.
Case 10
A 7-year-old male who sustained a laceration at the posterior aspect of the right ankle following an entrapment of his right foot and ankle in the rear spokes of the motorcycle. An irregular transverse laceration involving the Achilles tendon is associated with bleeding. Physical examination revealed an irregular laceration involving the right Achilles tendon with a positive Thompson’s test (Fig. 15). Radiographs of the foot, ankle, and distal tibia wound and fibular were unremarkable. Serial wound debridement and delayed Achilles tendon repair was done, and wound coverage by primary repair. The right foot was immobilized in plantarflexion for 3 weeks and serially monitored, manipulated, and immobilized every 2 weeks till the plantigrade position was achieved. The wound healed satisfactorily at 12-month follow-up with no equinus deformity and no functional deficits (Fig. 16). All the cases should have sufficient follow-up and clinical and radiographic pictures of cases at the last follow-up.
The first documented cases of wheelspoke injuries were reported from October 1976 to February 1978 in which 21 cases were described among pillion riders [5]. Several authors have since reported cases sparsely throughout the world. The majority [6] of the the cases in our series were children below the age of 12 years with the youngest being 4 years old and the oldest being 43 years (Table 1). This is consistent with the findings of Mak et al. following their retrospective analysis of 24 cases that sustained motorcycle and bicycle spokes injuries [7,8]. Children usually turn to have relatively shorter limbs and, thus may be unable to firmly place their feet on the pillion rider’s paddle which results in the limbs either dangling or dislodging into the spokes with a minimal jolt. All the cases in this series were pillion motorcycle riders. Pillion riders may be more predisposed due to the inadequate wheel protective covering and the relatively low anticipation of a possible jolt due to their position on the motorcycle. This is in variance with the findings of Chiang et al. who concluded that there was no difference in the occurrence of the injuries between riders and pillion riders [3]. The foot, ankle, and distal aspect of the leg are liable to injury in wheel spokes injuries (WSI). All cases in this series sustained injuries limited to the foot, ankle, and distal aspect of the leg with the left being the side commonly affected. We attribute the limited scope of these injuries to the low-energy nature of the mechanism of trauma. Several previous studies found similar patterns of injuries around the foot and ankle [6, 8-10]. One of the cases in our series sustained a calcaneal fracture, one had a greenstick distal tibia fracture, one sustained a fracture dislocation of the left ankle, and the rest sustained various degrees of soft tissue injuries comparable to a single center study in Pakistan which found that about 7.82% of patients sustained an additional bone injury [1]. All patients had limb salvage procedures including serial debridement, Achilles tendon repair, ankle spanning external fixation, and split-thickness skin grafts. The mean length of hospital stay in our series was 19 ± 13 days with the shortest being 8 days and the longest being 46 days (Table 1) which was similar to the findings of Mak et al. in which 18.4 day mean length of hospital stay was found [7]. Adult patients forfeit their productive activities within the period of admission, thus affecting household income and may worsen the economic status of families. All pediatric cases in this series drew assistance from family caregivers such as parents, siblings, and friends while receiving treatment. This has the capacity to tip about 5% of families into bankruptcy [11]. The situation could be bigger than it appears since most of the cases probably do not come to the tertiary facility for treatment except the severe cases.
Motorcycle WSIs are becoming frequent with varied complex ankle and foot involvement. These injuries can readily be prevented by including adequate protective covering of the rear wheel of motorcycles and legislation barring children from riding pillion and increasing public awareness about these injuries and how to prevent them.
Wheel spoke injuries are on the ascendency in the Northern part of Ghana and frequently result in complex foot and ankle injuries and ultimately debilitating deformities requiring the expertise of a multidisciplinary team comprising orthopedic, vascular, plastic surgery, radiology, physiotherapy among others for appropriate management of these preventable injuries. Thus, aggressive public health education is urgently required to forestall these injuries by all stakeholders.
References
- 1.Keerio NH, Majoka MW, Lakhani S, Saqlain HA, Abidi SA, Hussain A. Pattern and Presentation of Pediatric Spoke Wheel Entrapment Injuries: Our Hospital Experience. Pakistan Journal of Medical & Health Sciences. 2023 Jun 17;17(04):612-. [Google Scholar | PubMed]
- 2.Naumeri F, Qayyum B, Cheema NI, Sohail M, Bashir MM. Motorcycle spoked wheel injuries in children: A preventable accident. Ulus Trauma Emergency Surgery Journal 2019;25:474-8. [Google Scholar | PubMed]
- 3.Chiang VX, Cheng JY, Zhang ZC, Teo LT. Comparison of severity and pattern of injuries between motorcycle riders and their pillions: A matched study. Injury 2014;45:333-7. [Google Scholar | PubMed]
- 4.Agu TC. Motorcycle spokes entrapment foot injuries: Prevalence, and pattern of presentation in a private orthopedic and trauma center, Southeast Nigeria - A 10 year retrospective analysis. Afr J Trauma 2017;6:6-10. [Google Scholar | PubMed]
- 5.Ahmed M. Motorcycle spoke injury. Br Med J 1978;2:401. [Google Scholar | PubMed]
- 6.Suri MP, Naik NR, Raibagkar SC, Mehta DR. Heel flap injuries in spoke wheel accidents. Injury 2007;38:619-24. [Google Scholar | PubMed]
- 7.Mak CY, Chang JH, Lui TH, Ngai WK. Bicycle and motorcycle wheel spoke injury in children. J Orthop Surg 2015;23:56-8. [Google Scholar | PubMed]
- 8.Gupta H, Shrestha R. Bicycle-spoke injuries of the foot and ankle: A prospective study. J Coll Med Sci 2014;9:36-9. [Google Scholar | PubMed]
- 9.Zhu YL, Li J, Ma WQ, Bin ML, Xu YQ. Motorcycle spoke injuries of the heel. Injury 2011;42:356-61. [Google Scholar | PubMed]
- 10.Chu G, Vlok L, Zwaag-Pijls C, Houser CM, De Groot B. Emergency department management and follow-up of children with bicycle spoke injuries. J Emerg Med 2014;47:259-67. [Google Scholar | PubMed]
- 11.Tsiga-Ahmed FI, Jalo RI, Ibrahim UM, Kwaku AA, Amina A, Sanusi SM, et al. Length-of-stay after a health facility birth and associated factors: Analysis of data from three Sub-Saharan African countries. Ghana Med J 2022;56:100-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Arthroscopic Treatment of a Large Traumatic Morel-Lavallée Lesion of the Knee in a Young Female Athlete: A Case Report
April 1, 2026 Arthroscopic Treatment of a Large Traumatic Morel-Lavallée Lesion of the Knee in a Young Female Athlete: A Case Report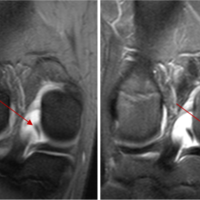 November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player
November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player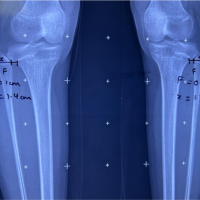 August 6, 2024 Bilateral Subluxation of the Proximal Tibiofibular Joint: A Rare Case Report
August 6, 2024 Bilateral Subluxation of the Proximal Tibiofibular Joint: A Rare Case Report November 10, 2023 Case Report: Traumatic Distal Achilles Tendon Rupture in a Pediatric Patient
November 10, 2023 Case Report: Traumatic Distal Achilles Tendon Rupture in a Pediatric Patient