
Central-type mirror foot deformity requires surgical treatment with rays excision and restoration of the width of the foot.
Dr. Nikolaos Laliotis, Department of Orthopedic, Inter Balkan Medical Center, Thessaloniki, Greece. E-mail: nicklaliotis@gmail.com
Abstract
Introduction: Mirror foot is an extremely rare type of foot malformation and is characterized by the duplication of toes and metatarsals around a centrally located hallux toe. It can be part of a generalized congenital dysplasia or an isolated one. The central type is the less frequent form of the mirror foot.
Case Report: We present an isolated type of central mirror foot with eight toes, seven metatarsals, and four cuneiforms. The isolated toe was medially located. The child presented no other deformities. Surgical management was performed at the age of 1 year, consisting of central-ray removal, using a dorsal and plantar incision. The approximation of the remaining metatarsals was reinforced using a suture that enwrapped the bones. We achieved an appropriate reduction in the width of the foot. A year after the procedure, the foot had a normal shape.
Conclusion: Our manuscript presents the case of a central mirror foot that was treated surgically with adequate restoration of the proximity of the remaining rays.
Keywords: Mirror foot, 8 toes foot, polydactyly, congenital foot anomaly, surgical treatment.
Polydactyly is a common foot malformation, with a reported incidence of 1.7/1000 live births [1,2]. Foot polydactyly is categorized according to its location: Postaxial polydactyly affects the lateral side of the foot and is the most common form; preaxial polydactyly affects the medial side; central type affects the central rays and is the most rare type of polydactyly [3,4]. A foot with eight toes is an extremely rare form of foot polydactyly. The term “mirror foot” was originally used to describe mirror image toe duplication around the midline axis, with a hallux toe in the center. The Greek term “diplopodia” is also used to describe this form of extremely rare foot congenital malformation. In the presence of duplicated tarsal or metatarsal bones, the foot is characterized as a mirror foot, whereas in the presence of only toe duplication, the term “polydactyly” is more appropriate [5-7]. Mirror foot can be associated with a variety of congenital dysplasias (e.g., tibial hypoplasia, fibular dimelia, Laurin–Sandrow syndrome), as well as isolated dysplasia, as we have previously reported for feet with seven toes. The rarest type of mirror foot is a duplication of the central rays [8-11]. The formation of supernumerary bones can affect any part of the foot skeleton, including the metatarsal, tarsal, talus, or calcaneum. The management of central foot polydactyly requires appropriate ray excision to restore the width of the foot, retain tendons for adequate foot movement, and restore normal alignment [7,12]. We present the case of a child with a right-sided central mirror foot of eight toes, seven metatarsals, and four cuneiforms. We describe the surgical management with an appropriate reduction of foot width. At the 1-year follow-up, the foot was observed to be restored to normal shape.
A 2-month-old baby, who was the second child of the family, was referred to our pediatric orthopedic department. His mother had an uneventful full-term normal delivery, and the parents had no history of bone dysplasias or limb malformations. A prenatal ultrasound (US) examination was not performed, as the parents were younger than 30 years and the pregnancy was reported as uncomplicated. The baby displayed normal motor development and milestones. Clinical examination revealed normal development of the spine, upper limbs, hips, and knees. US examination of the hips and kidneys confirmed normal development. There was no limb-length discrepancy. The right foot had eight toes, with the medial one floppy, a well-formed plantigrade foot, and a full range of movements of the ankle joint. On evaluation by a pediatrician, the functions of the heart and kidney were found to be normal. Moreover, a radiological examination of the child’s feet was performed at the ages of 6 and 12 months. As shown in Fig. 1, the foot had eight toes, with a hypoplastic toe on the medial side (counted as the 1st toe) (Fig. 1).

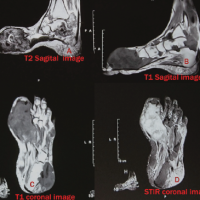
The radiological examination revealed that the medial hypoplastic toe had two ossified phalanges. Further evaluating the X-ray, there were seven metatarsals, with the 2nd and 3rd having a configuration of reduced length. The toe of the 1st metatarsal (counted as the 2nd toe) had two phalanges, as did the toe of the 3rd metatarsal (counted as the 4th toe). The remaining toes had three phalanges. There were ossification centers of the increased number of cuneiforms, hypoplastic navicular, and normally developed cuboid, talus, and calcaneum. The ankle joint, tibia, and fibula were normally developed (Fig. 2-4).

On clinical examination, the toes displayed normal movements, but the hypoplastic hallux had no sign of movement. The baby’s reaction to the sensation appeared normal. To ensure normal motor development, we waited until the child started walking independently. At 15 months of age, after starting to walk, the boy was surgically treated (Fig. 5).
Under general anesthesia, using a thigh tourniquet, we initially removed the hypoplastic 1st toe. Then, using a dorsal and plantar V-shaped incision, we removed the 2nd and 3rd metatarsals and toes. For each metatarsal, the tendons of the extensors and flexors of the amputated toes were properly dissected and cut at the level of the proximal metatarsal, by suturing each extensor to flexor. Vessels and nerves were appropriately ligated and cut using cautery. At the proximal part, the cuneiforms were left intact, but we realigned the proximal articular surface of the 4th and 5th metatarsals parallel to the cuneiform. The tibialis anterior was found duplicated, with a wide expansion both to medial and central cuneiform. We approximated the 1st and 4th initial metatarsals using sutures that encircled the metatarsals, reducing the width of the foot. The base of the retained 4th metatarsal was transferred to the area of the removed 2nd metatarsal. Particular care was taken to avoid lesions of intermetatarsal nerves and vessels. We stabilized the initial 4th and 5th metatarsals to cuneiforms using a smooth K-wire that was left protruding from the dorsum of the foot. The foot was immobilized in a cast. After 3 weeks, the K-wire was removed in the outpatient department. We used a fabricated cast to maintain the reduced width of the foot (Fig. 6).
The boy had an uneventful recovery. He started standing and walking with the cast 6 weeks after surgery. At the 1-year follow-up, he had maintained a nice shape of the foot, without an obvious discrepancy in length, and mainly the same width as that of the unaffected foot (Fig. 7).
Moreover, his radiological examination revealed normal development of the remaining metatarsals and toes, with reduced distance between the 1st and 2nd metatarsal Fig. 8.
A foot with eight toes represents an extremely rare type of mirror foot. This deformity may appear as an isolated deformity or as part of proximal bone dysplasia or syndromes. Verghese et al. reported preaxial mirror foot associated with tibial deficiency. They described patterns of fibular dimelia, tibial aplasia, tibial hypoplasia, and trapezoid tibia. The variety of duplication of the tarsal and mid-tarsal bones they reported was remarkable [8]. Deshmukh and Shyam reported the case of a child having a mirror foot with dysplastic tibia. The child was treated with the removal of supernumerary preaxial metatarsals and toes, as the first part of the surgery. Interestingly, the procedure did not include the excision of the duplicated talus. The varus deformity of the tibia underwent additional surgery in the second stage. However, the authors reported a recurrence of the deformity and a severe leg-length discrepancy [13]. Sahoo and Sahu reported a 17-year-old female with a mirror foot associated with eight toes and a trapezoid dysplastic tibia. Surgical treatment was not advised due to the severe shortening and deformity of the lower limb [14]. Bernardi et al. reported mirror foot in a girl with fibular duplication and VACTERL syndrome [9]. Mirror foot is described as associated with the Laurin–Sandrow syndrome, which is a rare congenital disorder characterized by polysyndactyly of the hands, mirror feet, and nose anomalies (hypoplasia of the nasal alae and short columella), often associated with ulnar and/or fibular duplication [10]. Palaniappan and Baalann presented the case of a 2-year-old boy affected by the syndrome; the boy had nine toes on the right and 10 toes on the left foot [15]. Mirror feet with eight toes as an isolated dysplasia are extremely rare. Fukazawa et al. have published three cases with a foot with nine metatarsals and eight toes among the two children with eight toes foot. They treated the child with ablation of the preaxial three toes and four metatarsals, after which the foot displayed an acceptable appearance [7]. Sananta et al. surgically treated a 5-month-old girl having bilateral mirror foot with eight toes on the right and seven toes on the left, by removing the medial preaxial toes and metatarsals. They described abnormal midfoot cartilage that was refashioned. They reported duplication of the tibialis anterior tendon that was inserted into the medial rays [1]. The central type of mirror foot is the rarest type of foot polydactyly. Papamerkouriou et al. presented a case of a central mirror foot with eight toes that was treated with dorsal and plantar V-shaped incisions. This enabled the appropriate management of the extra skin. They removed the 2nd, 3rd, and 4th toes from the medial side, without removing the medial cuneiform. They approximated the metatarsals using K-wires. Upon the follow-up radiological examination, a considerable gap remained between the metatarsals, but the shape of the foot was found to be comparable with the unaffected side [16]. Kim et al. reported surgical treatment of the central mirror foot with eight toes and metatarsals. They resected the 2nd, 3rd, and 4th rays and performed a partial excision of the midfoot. They transposed the 5th metatarsal to the base of the resected 2nd metatarsal and achieved a considerable reduction in the gap between the metatarsals [5]. We modified the existing surgical technique using a tight suture to reinforce the approximation of the remaining metatarsals. This method is similar to the approximation of the ribs in scoliosis surgery, wherein a rib is removed for either a bone graft or an excision to improve the rib hump. The ribs above and below the one that is removed are approximated with a set of stitches. These are placed around them and tightened to achieve approximation. We resected two metatarsals, and this probably facilitated the approximation of the metatarsals instead of cases that removed three metatarsals. Using both plantar and dorsal incisions, we had a clear identification of the bone and the articulation between the midtarsal and metatarsal bones. The follow-up period was brief, and the patient remains under regular annual examination. He wears the same size of shoes now. However, it is essential to continue looking after the patient and monitoring the growth of the foot [17].
We report a child with a central type of mirror foot, having eight toes and seven metatarsals, as an isolated deformity. We treated him at the age of 1 year, with central rays excision, with the approximation of the remaining gap using a reinforcement suture.
A central type of mirror foot can be surgically managed with the excision of supernumerary rays. The approximation of the remaining metatarsals is an important factor in reducing the width of the foot.
References
- 1.Sananta P, Sahdiniar FF, Siahaan LD. The management of mirror foot polydactyly: A case report. Int J Surg Case Rep 2022;91:106780. [Google Scholar | PubMed]
- 2.Vlahovic AM, Pistignjat BS, Vlahovic NS. Nine toes; Mirror foot deformity. Indian J Orthop 2015;49:478-81. [Google Scholar | PubMed]
- 3.Belthur MV, Linton JL, Barnes DA. The spectrum of preaxial polydactyly of the foot. J Pediatr Orthop 2011;31:435-47. [Google Scholar | PubMed]
- 4.Burger EB, Bus SA, Hovius SE, van Nieuwenhoven CA. Lateral versus medial hallux excision in preaxial polydactyly of the foot. Foot Ankle Int 2020;41:1553-62. [Google Scholar | PubMed]
- 5.Kim JS, Fowler JR, Davit AJ. Operative technique and management of central foot polydactyly. JPRAS Open 2022;32:61-71. [Google Scholar | PubMed]
- 6.Khan SA, Kumar A, Varhney MK. A rare association of deformities with diplopodia, aplasia of the tibia and double fibula: A case report. J Med Case Rep 2008;2:102. [Google Scholar | PubMed]
- 7.Fukazawa H, Kawabata H, Matsui Y. Mirror foot: Treatment of three cases and review of the literature. J Child Orthop 2009;3:277-82. [Google Scholar | PubMed]
- 8.Verghese R, Shah H, Rebello G, Joseph B. Pre-axial mirror polydactyly associated with tibial deficiency: A study of the patterns of skeletal anomalies of the foot and leg. J Child Orthop 2007;1:49-54. [Google Scholar | PubMed]
- 9.Bernardi P, Graziadio C, Rosa RF, Pfeil JN, Zen PR, Paskulin GA. Fibular dimelia and mirror polydactyly of the foot in a girl presenting additional features of the VACTERL association. Sao Paulo Med J 2010;128:99-101. [Google Scholar | PubMed]
- 10.Buzea C, Boulanger N. Laurin-sandrow syndrome - a review of the literature and classification system. Clin Dysmorphol 2022;31:109-12. [Google Scholar | PubMed]
- 11.Laliotis N, Konstantinidis P, Chrysanthou C. A seven toes foot: Case series as an isolated Dysplasia with variety of appearance. Cureus 2022;14:e32949. [Google Scholar | PubMed]
- 12.Shahcheraghi GH, Javid M. Treatment of the mirror foot with central ray resection: Report of 2 cases. Iran J Med Sci 2018;43:550-3. [Google Scholar | PubMed]
- 13.Deshmukh R, Shyam AK. Reconstruction of mirror foot with dysplastic tibia. J Orthop Case Rep 2015;5:54-6. [Google Scholar | PubMed]
- 14.Sahoo PK, Sahu MM. Mirror foot with trapezoidal dysplastic tibia- A case report. J Orthop Case Rep 2019;9:26-9. [Google Scholar | PubMed]
- 15.Palaniappan P, Baalann KP. Laurin-sandrow syndrome. Pan Afr Med J 2021;40:115. [Google Scholar | PubMed]
- 16.Papamerkouriou YM, Antoniou G, Krallis P, Anastasopoulos J. Central mirror foot: Treatment and review of the literature. Cureus 2020;12:e8448. [Google Scholar | PubMed]
- 17.Lalé SA, Burger EB, Bessems JH, Pollet V, van Nieuwenhoven CA. Long term follow-up and development of foot complaints in a surgically treated mirror foot-A case report and review of literature. Foot Ankle Surg 2017;23:e9-13. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report
April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report April 1, 2025 A Rare Footprint: A Case Report of Isolated Pre-Axial Fully Developed Supernumerary Toe
April 1, 2025 A Rare Footprint: A Case Report of Isolated Pre-Axial Fully Developed Supernumerary Toe January 1, 2025 Ellis-van Creveld Syndrome: A Rare Case Report with Emphasis on Skeletal Manifestations
January 1, 2025 Ellis-van Creveld Syndrome: A Rare Case Report with Emphasis on Skeletal Manifestations August 6, 2024 Case Report of a Delayed Rare Pipkin Type III Fracture in Adult Male Patient
August 6, 2024 Case Report of a Delayed Rare Pipkin Type III Fracture in Adult Male Patient