
Even though K-wires in shoulder injuries are still associated with loosening and migration to spine and other vital structures, early identification can aid for easy removal and prevent drastic consequences.
Dr. K Venkataramana, Department of Orthopedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: venkat.ortho@aiimsmangalagiri.edu.in
Abstract
Introduction: Kirshner wires are commonly used for orthopedic surgical fixation for shoulder injuries, particularly around the acromioclavicular joint. They are versatile, cheap, and minimally invasive in stabilizing bone fragments. However, there have been cases of secondary migration of K-wires from the clavicle to surrounding tissues, particularly around the cervical spine.
Case Report: We present a case of a 60-year-old female with left-sided neck pain and radiation to the left upper limb, a K-wire was found to have migrated through the C7-T1 foramina left side into the spinal canal posterior to the vertebral body in a transverse trajectory. The patient underwent surgical removal of the K-wire, and post-operative pain improved without neurological complaints.
Conclusion: Even though Kirshner wires are versatile, cheap, and minimally invasive in stabilizing bone fragments, but migration to unexpected anatomical sites remains a concern. This paper reviews the literature and discusses clinical presentation, diagnostic modalities, and surgical approaches related to spinal canal migration of K-wires.
Keywords: Kirshner wire, migration, spinal canal, clavicle fixation, acromioclavicular repair.
Unstable fractures around the shoulder girdle involving the acromioclavicular joint or lateral end clavicle are usually managed by reduction and stabilization with Kirschner’s wires (K-wires) [1] and tension band wires or sutures. K-wires are thin, malleable, and can break easily compared to plates and screws, hence cause loosening and migration to surrounding tissues [2]. K-wires are usually cut/bend at the skin surface externally or over the bone surface internally, most of them requiring removal of the wire after fracture healing is complete [3]. Migration of K-wire from joints to deep visceral organs/tissues is rare. It can cause complications, primarily when originating from acromioclavicular and clavicle fixations [4,5] as their usage around the shoulder is associated with migration into thoracic cavity, soft tissues/vessels in the neck/thoracic region, and thoracic/cervical spine [6]. Migration into the spinal canal is rare but can lead to neurologic complications. Probable reasons for these complications were breakage/loosening and migration of implant to surrounding tissues, especially K-wires. Certain factors associated with increased incidence of these complications around the shoulder joint due to the inherent mobility of the shoulder girdle, and negative intrathoracic pressure. We report here a case of Transforaminal migrated K-wire from the lateral end clavicle to C7-T1 foramina lying in to cervical spinal canal managed by surgical removal with no neurological deficit.
A 65-years-old female had presented to us with complaints of chronic pain around the left side of the neck with mild radiation of pain to shoulder region for 1 year with VAS(visual analoge scale) around 6/10. She does not have any paresthesia/numbness over upper limb. She had a previous history of surgery of her left shoulder operated 8 years ago for lateral end clavicle fracture by K-wires and tension band wire fixation.
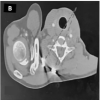
On radiological evaluation X-ray (Fig. 1 and 2) and Computed tomography (CT) Cervical spine (Fig. 3 and 4) there were 2 K-wires of unequal sizes and stainless-steel wire in lateral end clavicle across acromioclavicular joint. Another K-wire was lying at the level of C7 vertebral body lying posterior to vertebral body in the canal. A part of K-wire was lying in the spinal canal across the foramina(C7-T1) in the transverse trajectory toward transverse process. Possibly the wire from the lateral end clavicle was broken and migrated toward cervical spine in transverse trajectory. Measurements were made to localize the tip of the K-wire lying anterior to the transverse process; the lateral end of the wire was lying at 1.5–2 cm from skin surface.
Surgical exploration was planned with the possibility of need for corpectomy and wire retrieval from the spinal canal and simultaneous supraclavicular exploration to trace the tip of K-wire and release the adhesions around the K-wire. Patient was counseled about the same and went ahead for surgery.

Intraoperatively, through a mini-open incision over supraclavicular region K-wire tip was explored (Fig. 5) under image guidance. Wire tip was freely mobile and free from any soft-tissue adhesions. Slow movements allowed K-wire to be extracted backward in the same trajectory as wire was loose and removed completely out of the wound (Fig. 6). No cerebrospinal fluid (CSF) leak was noticed. Other K-wires over lateral end clavicle and acromion were removed through separate incision. Moreover, manipulation of the shoulder was attempted to improve range of movement. Postoperatively patient was asymptomatic with resolved pain over the neck and shoulder region. VAS improved to zero and no post-operative neurological symptoms were reported. The patient was on regular follow-up until 1 year and asymptomatic with no recurrence of similar complaints.

Clinical features
Migration of K-wires is rare but possible, with the prevalence of 5.8 to 54% [3]. The slow movement may be unnoticed due to the sharp tip, which can dissect the tissue planes. Spinal migration occurs around the transverse process, lamina, and anterior to vertebral bodies. Migration through neural foramen into the spinal canal is rare; only 20 cases are reported in the literature (Table 1). Most of them occurred in males and only two females, including the present case. The initial surgery was related to shoulder girdle in almost all cases except Furuhata et al. [6], reported after sternal repair for cardiac surgery. The duration between initial surgery and diagnosis of migration was the earliest in 26 days [7] and the longest in 19 years [4]. Clinical features varied from asymptomatic with incidental detection on follow-up in three cases [7-9]. Most of the cases reported neck pain/headache and radiating to the shoulder and upper limb without neurological deficits. Only five cases reported neurological deficits causing quadriparesis, Brown-sequard syndrome, and bowel and bladder involvement [10-14]. Furuhata et al. described a case of K-wire used for sternum fixation after cardiac surgery migrating to the spinal canal after piercing through the vertebral body [6]. Etiology is unknown but is attributed to movements of the shoulder girdle, negative intrathoracic pressure, breathing movements, etc. Older case reports have frequently noted a high incidence of paraparesis and quadriparesis. Interestingly, no paraparesis has been reported since the case report of Fransen et al. in 2007 [14].
Investigations
CT scan helps to know the lesion’s anatomy and identify the sharp tip’s exact location. CT angiography is recommended in case of suspicion of vessel involvement. We did a CT angiogram to check proximity or injuries to vertebral vessels. MRI is usually avoided to prevent loose metal oscillation from the magnetic field. MRI done in a study by Al Rhaazi et al. [15] reported no neurologic deterioration after the scan.
Surgical procedure
All reports removed the migrated wire except Liberski and Ficek [16] due to the patient’s refusal of surgery. Bennis et al. [8] reported that approaching the tip of the K-wire and removal along the axis of penetration was necessary to avoid neurologic complications. Loncán et al., in their patient with Brown-Sequard syndrome, did not consider exposing dura due to uncertain benefits and risks associated. Longitudinal traction was used to pull the wire. The patient recovered sphincter control, could walk independently with a cane by 2 months, and was asymptomatic by 4 months [10]. Li et al. [17] reported using thoracoscopy to remove the K-wire while being prepared for an open procedure. Fransen et al. performed a laminectomy of T2/3, exposed both ends of the wire, and removed it with traction. They faced CSF leakage, which stopped with fibrin glue [14]. Gulyaev et al. [4] used a combined posterior and lateral approach in a patient with C6/7 involvement to avoid secondary spinal cord injury and CSF leakage. Several case reports have used extensive exposures to expose the lateral part of the wire. We approached with minimal incision exposing the tip of the wire, dissected and separated from surrounding tissues, extracted the wire along the axis of trajectory without any complications.
Outcomes
Improvement in symptoms in patients is seen in all patients after surgery, and none have reported surgery-related secondary spinal cord injury or vascular injuries. Improvement in neurologic status, including quadriparesis, and Brown-Sequard syndrome in the case reports suggests the need for prompt diagnosis and early treatment can give excellent results. Residual neurological deficits were minimal reported by Priban et al with permanent sexual dysfunction.
Plate fixation methods are preferred over K-wire fixation in the shoulder region. Otherwise, early removal of wires is essential to avoid complications. Migration into the spinal canal is sporadic but has been reported increasingly in recent years. Removal of K-wire is preferable even in asymptomatic patients. Minimal invasive longitudinal removal is safe after thorough investigations. In neurologic involvement, a combined posterior and lateral approach can be necessary. CT angiography is essential to rule out vertebral or spinal artery involvement. It helps in planning alternate approaches for K-wire removal.
K-wire fixation was widely used for injuries around the shoulder girdle. A possible complication is loosening and migration of K-wires to visceral structures or spinal canal. Cases operated years back must be actively followed up for any possible consequences and counseled for implant removal if required. This case again emphasizes to wisely choose proper implant to prevent such complications.
References
- 1.Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: A comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthopaedica Scandinavica. 2002 Jan;73(1):50–3. [Google Scholar | PubMed]
- 2.Leidel BA, Braunstein V, Pilotto S, Mutschler W, Kirchhoff C. Mid-term outcome comparing temporary K-wire fixation versus PDS augmentation of Rockwood grade III acromioclavicular joint separations. BMC Res Notes 2009;2:84. [Google Scholar | PubMed]
- 3.Firoozabadi R, Kramer PA, Benirschke SK. Kirschner wire bending. J Orthop Trauma 2013;27:e260-3. [Google Scholar | PubMed]
- 4.Gulyaev DA, Godanyuk DS, Kaurova TA, Krasnoshlyk PV, Maikov SV. Kirschner wire migration into spinal canal after acromioclavicular joint fixation (literature review and clinical case). Traumatol Orthop Russia 2018;24:121-8. [Google Scholar | PubMed]
- 5.Minić L, Lepić M, Novaković N, Mandić-Rajčević S. Symptomatic migration of a Kirschner wire into the spinal canal without spinal cord injury: Case report. J Neurosurg Spine 2016;24:291-4. [Google Scholar | PubMed]
- 6.Furuhata R, Nishida M, Morishita M, Yanagimoto S, Tezuka M, Okada E. Migration of a Kirschner wire into the spinal cord: A case report and literature review. J Spinal Cord Med 2020;43:272-5. [Google Scholar | PubMed]
- 7.Was MT, Kurowski K, Francuz I. Migration of Kirschner wire into the spinal canal as complication of inveterate shoulder luxation treatment-case study. Ortop Traumatol Rehabil 2010;12:370-5. [Google Scholar | PubMed]
- 8.Bennis S, Scarone P, Lepeintre JF, Puyo P, Aldea S, Gaillard S. Asymptomatic spinal canal migration of clavicular K-wire at the cervicothoracic junction. Orthopedics 2008;31:12 [Google Scholar | PubMed]
- 9.Farion AO, Paskov RV, Bazarov AY, Prokopev AN, Svinoboev SL, Mezentsev AA. Migration of a Kirschner wire into the spinal canal after acromioclavicular joint repair (case report). Genij Ortop 2023;29:425-30. [Google Scholar | PubMed]
- 10.Loncán LI, Sempere DF, Ajuria JE. Brown-Sequard syndrome caused by a Kirschner wire as a complication of clavicular osteosynthesis. Spinal Cord 1998;36:797-9. [Google Scholar | PubMed]
- 11.Regel JP, Pospiech J, Aalders TA, Ruchholtz S. Intraspinal migration of a Kirschner wire 3 months after clavicular fracture fixation. Neurosurg Rev 2002;25:110-2. [Google Scholar | PubMed]
- 12.Pribán V, Toufar P. A spinal cord injury caused by a migrating Kirschner wire following osteosynthesis of the clavicle: A case review. Rozhl Chir 2005;84:373-5. [Google Scholar | PubMed]
- 13.Mamane W, Breitel D, Lenoir T, Guigui P. Spinal migration of a Kirschner wire after surgery for clavicular nonunion. A case report and review of the literature. Chir Main 2009;28:367-9. [Google Scholar | PubMed]
- 14.Fransen P, Bourgeois S, Rommens J. Kirschner wire migration causing spinal cord injury one year after internal fixation of a clavicle fracture. Acta Orthop Belg 2007;73:390-2. [Google Scholar | PubMed]
- 15.Al Rhaazi N, Susatyo AY, Faesal, Bari YA. Spinal K-wire migration following acromioclavicular dislocation surgical treatment: A case report with scoping review discussion. MBIOMJ 2023;33:118-25. [Google Scholar | PubMed]
- 16.Liberski J, Ficek K. Kirschner wire migration from the clavicle to the cervical spine. Int J Case Rep Images 2013;4:308. [Google Scholar | PubMed]
- 17.Li Y, Wang B, Lv G, Xiong G, Liu W. Video-assisted thoracoscopic surgery for migration of a Kirschner wire in the spinal canal: A case report and literature review. Turk Neurosurg 2013;23:803-6. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review
April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review December 10, 2022 Unusual Failure of Modular TKA Prosthesis and Screw Migration following Revision Total Knee Arthroplasty
December 10, 2022 Unusual Failure of Modular TKA Prosthesis and Screw Migration following Revision Total Knee Arthroplasty March 10, 2021 A Case of Tumor-Induced Osteomalacia: Finding the Culprit Acetabular Tumor and Successful Resection with a Novel Hip Joint-Preserving Surgery
March 10, 2021 A Case of Tumor-Induced Osteomalacia: Finding the Culprit Acetabular Tumor and Successful Resection with a Novel Hip Joint-Preserving Surgery January 10, 2018 Unusual Presentation of Tuberculosis of Subtalar Joint
January 10, 2018 Unusual Presentation of Tuberculosis of Subtalar Joint