
Hematoma block is a simple, effective, and safe method for pain management during manipulation and percutaneous pinning of extra- articular distal radius fractures in the emergency department. It significantly reduces intraoperative and post-operative pain, It is time- efficient, reduces hospital stay, and allows the procedure to be performed as an outpatient or day-care surgery.
Dr. Md Zafar Iqbal, Department of Orthopedics, Dr. Shankarrao Chavan Government Medical College, Nanded, Maharashtra, India. E-mail: docmdzafariqbal@gmail.com
Introduction: Fractures of the distal end of the radius have a higher prevalence, particularly in older individuals, and typically necessitate a painful procedure of reduction by manipulation. Various regional blocks, including hematoma blocks, are used to manage this pain. Hematoma block is simple, effective, and safe, providing adequate analgesia without increasing post-procedural infection risks.
Materials and Methods: This prospective study was conducted to observe and analyze the outcomes of 18 patients, aged from 18 to 65 years, who had displaced fractures in the distal end of the radius. These fractures were treated using percutaneous pinning under a hematoma block. The study measured the time from trauma to surgery, time for hematoma block administration, surgery duration, Visual Analog Scale (VAS) scores for pain preoperatively, intraoperatively, and postoperatively, reduction quality, and functional outcome using Mayo Wrist score and complications if any.
Results: The time from trauma to surgery was 31.44 ± 9.25 h. Hematoma block administration took 3.45 ± 1.34 min, and surgery duration was 29.16 ± 5.33 min. Pre-operative VAS was 6.39 ± 1.09, intraoperative VAS was 0.94 ± 0.54, and post-operative (3 h) VAS was 2.06 ± 0.80. The average pain-free duration postoperatively was 9.36 ± 3.21 h. Quality of reduction was excellent in 44.44% of cases and good in 38.89% of cases. Patients were discharged on average 4.19 ± 0.82 h after surgery. The functional outcome as noted by the Modified Mayo wrist score was excellent in 55.55% and poor in only 5.55% of cases.
Discussion: The hematoma block demonstrated effective post-operative pain control, comparable to the brachial plexus block. It provided significant perioperative pain relief, reduced hospital stay, and allowed for outpatient or daycare surgery.
Conclusion: Hematoma block is a viable alternative for managing extra-articular distal end radius fractures in the emergency department, offering effective pain relief with minimal risk of complications. Further studies are needed to compare its efficacy with other anesthesia modalities.
Keywords: Distal end radius fracture, hematoma block, percutaneous pinning, Visual Analog Scale score.
Fractures at the distal end of the radius are the most prevalent fractures among the elderly, comprising almost 16% of all fractures [1]. Fracture reduction requires manipulation which is a painful maneuver. Various methods of analgesia are available which include – Nerve root block, intravenous regional anesthesia, intramuscular sedation, hematoma block, general anesthesia, and conscious sedation. Hematoma block is a simple, efficacious method for pain management during manipulation and percutaneous Kirschner wires (K-wire) fixation in the emergency department. Research indicates that hematoma blocks are a reliable approach to achieving pain relief without an elevated risk of post-procedural infections when compared to other regional blocks [2]. These are equally effective in terms of achieving acceptable reduction and lowering discomfort during the procedure when compared to conscious sedation with intravenous (IV) propofol and other alternative method. This is determined by measuring the Visual Analog Scale (VAS) before, during, and after the procedure [3]. The technique of wrist hematoma block involves nerve paralysis as a primary mechanism. Administering anesthesia to the nerves surrounding an injury or fracture enables effective manipulation of the bones. Displaced or angulated fractures frequently result in the accumulation of blood around the fractured bones, leading to the formation of a hematoma. To effectively administer anesthesia, it is crucial to precisely identify the location of the fracture and directly inject the required anesthesia into that hematoma.
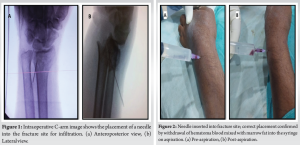
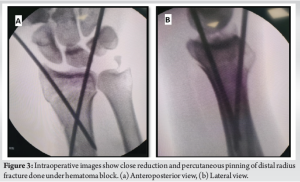
The study was a prospective observational study done between January 2022 and December 2022. The study was approved by the institutional ethical committee. The study included 18 patients, ranging in age from 18 to 65 years, who had displaced extra-articular distal end radius fractures. Only those patients who were admitted to a tertiary care center in Nanded, Maharashtra, within 48 h of the trauma were included in this study. Patients with compound injuries, intraarticular involvement, severe comorbidities, uncontrolled diabetes, and serious cardiac disease and patients below age 18 years and above age 65 years were excluded from the study. On admission, a detailed personal history was taken, and clinical evaluation was done for signs of fracture and confirmed after an X-ray of the injured wrist. All patients fulfilling the inclusion criteria were managed with percutaneous K-wire fixation under a hematoma block in the emergency operation room. Once the patient was shifted to the operating room patient received a single dose of IV antibiotic (cefoparazone+sulbactam 1.5 g). Electrocardiogram monitoring and pulse-oximetry monitoring were ensured during the entire procedure. Then 5 mL of lidocaine 2% with 5 mL of 0.5% bupivacaine was injected at the site of fracture. In all procedures, the needle was dorsally introduced up to the fracture after confirmation under the c-arm. Aspiration of blood mixed with fat globules of the bone marrow was confirmatory of needle placement into the fracture hematoma. Subsequently, the needle was removed while gradually administering the anesthetic medication. The identical treatment was performed on the underside of the fracture utilizing the same point of entry. Infiltration of a small amount of cocktails was also done at the entry points of K-wire. Gentle massage of the infiltration site was performed after infiltration (Figs. 1 and 2).
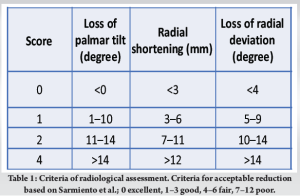
Manipulation and reduction were done after 10 min of infiltration of the cocktail, after standard painting and draping which was followed by K-wire fixation (Fig. 3). Pre-operative, intraoperative, and post-operative (after 3 h) VAS scores were assessed for pain. Reduction and fixation of the fracture were confirmed under C-arm intraoperatively. Postoperatively while discharged patient received a single dose of IV antibiotics and 3 days of oral antibiotics to avoid any risk of infection. Daily pin-track care was taught to the patient’s relative for dressings at home. K-wire removal was done on 6 weeks post-operative. During this period, standard sponge ball exercises and protected passive wrist range of motion exercises were started. After K-wire removal patient was started with active circumduction exercises and strengthening exercises. On 1-month, 2-month, and 6-month follow-up reduction was reassessed for quality of reduction, any secondary displacement, signs of union on X-ray, and complications if any.
Quality of reduction was assessed using the Sarmiento radiological score [3, 4] (modified Lidstrom criteria) as excellent, good, fair, or poor (Table 1). At 6 months’ follow-up, each patient was assessed for wrist function by the Modified Mayo Wrist score which takes into consideration pain, functional status, range of motion, and grip strength. Each parameter is given a maximum score of 25, and a total score is calculated by adding all four parameters [5].
In our study, most patients were female (61.11%), and left-sided injury was more observed (66.67%). The mean age of the study sample was 41 years (range 24–57 years). The mean time from trauma to surgery was 31.44 ± 9.25 h, 3.45 ± 1.34 min meantime was required for administration of hematoma block, and the mean time taken for reduction and fixation was 29.16 ± 5.33 min under hematoma block. Mean pre-operative VAS was 6.39 ± 1.09, after giving a block, intraoperative VAS was 0.94 ± 0.54 and post-operative mean VAS was 2.06 ± 0.80 (Table 2).

No analgesics were administered to any of the patients before reduction in this trial. We assessed the quality of reduction by Sarmiento radiological scoring criteria by analyzing anteroposterior and lateral X-ray images acquired immediately after the reduction procedure and 1 month later (Fig. 4). Quality of reduction was excellent for most patients (44.44%), followed by good in 38.89% of cases, whereas it was fair in two cases and poor in one case in whom revision surgery was needed. A single case out of 18 patients required sedation as the patient was having discomfort during manipulation (VAS score = 3). Furthermore, while giving traction for the reduction of the fracture, four patients reported mild discomfort at the elbow/arm as the total limb was not anesthetized, but this was tolerable without the need for any sort of extra sedation or analgesia.

After the hematoma block, in post-operative period, the patient experienced less pain after reduction (VAS: 2.25 ± 0.2) because of the anesthetic effect of the hematoma block. The average time for discharge after surgery under a hematoma block was 4.19 ± 0.82 h.
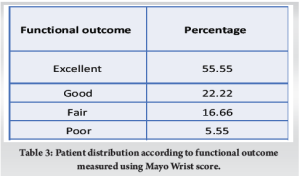
Patients operated under hematoma block had shorter induction time, and lower risk of systemic complications, lesser administration of the drug was required with shorter stay in the hospital, allowing the procedure to be performed as an outpatient procedure or day care procedure. Furthermore, post-operative analgesia was provided due to the hematoma block (9.36 ± 3.21 h) reducing the need for post-operative analgesia in the immediate post-operative period. Functional assessment done by Mayo Wrist score at 6 months’ follow-up. A score of 91–100 was considered excellent, 81–90 as good, 65–80 as fair, and <65 as poor. In our study, we found excellent results in 10 patients (55.55%), good in four patients (22.22%), fair in three patients (16.66%), and poor in one case (5.55%) (Table 3).
There were two cases of K-wire back-out at 1-month follow-up which did not need any intervention as the reduction was maintained. One patient had a secondary loss of reduction which was managed with open reduction and internal fixation with volar plating. No incidence of pin tract infection was noted in any case.
Many literature is available which shows hematoma block to be an effective alternate mode of anesthesia for close reduction and percutaneous pinning of distal end radius fracture with a significantly low complication rate [6, 7, 8, 9]. Despite numerous studies showing the comparatively inferior pain-relieving effectiveness of hematoma block, its popularity has significantly grown over time due to its safety and simplicity [10]. Achten et al. in their study compared the outcome of distal end radius fracture managed with close reduction and casting versus percutaneous K-wire fixation. They concluded that fixation with K-wire is better compared to casting as fixation is more stable and their lesser risk of loss of reduction [11]. Fanjalalaina et al. in their comparative study between close reduction and casting and percutaneous K-wire fixation of 38 patients with distal end radius displaced unstable fracture, who were given hematoma block, found that there was significant pain reduction in both groups. Adhering to the asepsis protocol ensures that there is no increased risk of infection when doing a hematoma block [6]. 2% lidocaine of volume 10–15 mL has been used by most authors for hematoma block for manipulation and reduction of distal end radius fracture [3, 12]. Orbach et al. [13] in their study to compare the efficacy of 20 mL of 1% lidocaine versus 10 mL of 2% lidocaine found that the VAS score was not significantly different for both the volume of lidocaine. In our study, we found that 10 mL of cocktail (5 mL 2% lidocaine + 5 mL 0.5% bupivacaine) was enough for all patients to attain effective anesthesia. In our study, the hematoma block demonstrated effective post-operative pain control, with a mean pain-free duration of 9.36 ± 3.21 h and a significant reduction in VAS scores, underscoring its potential in early post-operative pain management. Comparatively, Nho et al. found that while the brachial plexus block was superior in managing early post-operative pain (12.4 ± 3.9 h pain-free duration), general anesthesia was notably less effective, with a 2-h post-operative VAS score of 6.8 ± 2.5 [14]. Furthermore, a study by Kukreja et al. [15] showed comparable results to our study, this study compared supraclavicular and infraclavicular brachial plexus blocks with adequate pain control VAS 1.02 ± 0.32 and 1.77 ± 0.48, respectively, and time of discharge was significantly longer than our study i.e. 7.33 ± 2.73 and 16.52 ± 5.97 h, respectively. Our study attests to a significant reduction in VAS score during the peri-operative period as well as post-operative period, comparable to the Brachial plexus block. This technique is significantly less time-consuming and reduces the hospital stay of patients drastically to the extent that the procedure can be conducted as an outpatient procedure or a daycare surgery. While understanding the shortcomings of this technique such as conversion to open reduction was not possible during the same setting, of no use in compound fractures as hematoma is not contained in such cases. This technique has a limitation of being confined to closed extra-articular distal end radius fractures. Further studies and randomized controlled trials are needed to compare the efficacy of this modality to available modalities such as brachial plexus blocks and general anesthesia comparing their perioperative pain control, post-operative analgesia, and complications.
Hematoma block can be considered a good alternate mode of anesthesia with minimal risk of complication, for the management of extra-articular distal end radius fracture presently early after trauma in the emergency department. This technique also gives the added advantage of post-operative reduction in pain reducing the need for analgesia in the early post-operative period.
Extra-articular distal end radius fractures presenting early after trauma can be managed under a hematoma block in the emergency department successfully with prompt treatment, lesser complications, and provision of early discharge from the hospital.
References
- 1.Rockwood CA Jr., Green DP, Bucholz RW, Heckman JD. Fractures in Adults. 9th ed. Philadelphia, PA: Lippincott-Raven; 1996. p. 769-70 [Google Scholar]
- 2.Johnson PQ, Noffsinger MA. Hematoma block of distal forearm fractures: Is it safe? Orthop Rev 1991;20:977-9 [Google Scholar]
- 3.Myderrizi N, Mema B. The hematoma block an effective alternative for fracture reduction in distal radius fractures. Med Arh 2011;65:239-42. [Google Scholar]
- 4.Sarmiento A, Latta LL. Colles’ fractures: Functional treatment in supination. Acta Chir Orthop Traumatol Cech 2014;81:197-202. [Google Scholar]
- 5.Slutsky DJ. Outcomes assessment in wrist surgery. J Wrist Surg 2013;2:1-4. [Google Scholar]
- 6.Fanjalalaina RM, Tiana R, Jean Claude RH. Percutaneous pinning of distal radius fractures using hematoma block: Outcomes in our center. Peertechz J Orthop Rheumatol 2015;1:1-3. [Google Scholar]
- 7.Strohm PC, Müller CA, Boll T, Pister U. Two procedures for kirschner wire osteosynthesis of distal radial fractures: A randomized trial. J Bone Joint Surg 2004;86:2621-8. [Google Scholar]
- 8.Tabrizi A, Mirza Tolouei F, Hassani E, Taleb H, Elmi A. Hematoma block versus general anesthesia in distal radius fractures in patients over 60 years in trauma emergency. Anesth Pain Med 2016;7:e40619. [Google Scholar]
- 9.Thakkar CV. Hematoma block: An effective anesthesia for distal radius fractures. Int J Orthop Sci 2019;5:347-9. [Google Scholar]
- 10.Ogunlade SO, Omololu AB, Alonge TO, Salawu SA, Bamgboye EA. Haematoma block in reduction of distal radial fractures. West Afr J Med 2002;21:282-5. [Google Scholar]
- 11.Achten J, Sones W, Dias J, Hedley H, Cook JA, Dritsaki M, et al. Surgical fixation with K-wires versus plaster casting in the treatment of dorsally displaced distal radius fractures: Protocol for Distal Radius Acute Fracture Fixation Trial 2 (DRAFFT 2). BMJ Open 2019;9:e028474. [Google Scholar]
- 12.Alatishe KA, Ajiboye LO, Choji C, Idowu OS, Olanrewaju OS. A comparative study of the analgesic effect of haematoma block versus intravenous sedation for reduction of distal radius fractures in adults. Int J Anesth Pain Med 2022;8:66. [Google Scholar]
- 13.Orbach H, Rozen N, Rinat B, Rubin G. Hematoma block for distal radius fractures - prospective, randomized comparison of two different volumes of lidocaine. J Int Med Res 2018;46:4535-8. [Google Scholar]
- 14.Nho JH, Jang BW, An CY, Yoo JH, Song S, Cho HB, et al. General versus brachial plexus block anesthesia in pain management after internal fixation in patients with distal radius fracture: A randomized controlled trial. Int J Environ Res Public Health 2022;19:9155. [Google Scholar]
- 15.Kukreja P, Kofskey AM, Ransom E, McKenzie C, Feinstein J, Hudson J, et al. Comparison of supraclavicular regional nerve block versus infraclavicular regional nerve block in distal radial open reduction and internal fixation: A retrospective case series. Cureus 2022;14:e24079. [Google Scholar]








