
Highlights the rarity of simultaneous ACL reconstruction and distal femoral osteotomy for genu valgum, demonstrating its effectiveness in addressing knee instability and malalignment with improved outcomes.
Dr. Parthasarathi Das, Department of Orthopaedics, Sadguru Hospital, Cuttack, Odisha, India. E-mail: psdas82@gmail.com
Abstract
Introduction: Anterior cruciate ligament (ACL) injury sometimes is associated with genu valgum. Valgus malalignment poses concerns due to its potential to increase strain on the ACL, thereby elevating the risk of osteoarthritis in the lateral compartment of the knee. However, lacune still exists regarding the concomitant reconstruction of ACL and distal femoral osteotomy in ACL-deficit knee with genu valgum. The present case report aims to fill this gap by presenting a rare case of a young patient with a symptomatic ACL deficit knee and femur-originated genu valgum.
Case Report: A young male presented with bilateral genu valgum at our clinic with pain and instability of the right knee following a sports injury for 1 year. The anterior drawer, Lachman, pivot shift, and McMurray test were positive in physical examination. The surgical intervention comprised lateral open wedge osteotomy of the distal femur, all-inside reconstruction of the ACL, and partial meniscectomy for the meniscal tear.
Conclusion: Simultaneous ACL reconstruction with femur osteotomy offers favorable outcomes in patients presenting with genu valgum. This integrated approach minimizes hospitalization and rehabilitation periods. Meticulous planning and surgical techniques, including careful femoral tunnel placement, can mitigate potential complications like plate interference.
Keywords: Osteotomy, anterior cruciate ligament, genu valgum.
The efficacy of high tibial osteotomy (HTO) along with reconstruction of the anterior cruciate ligament (ACL) in achieving favorable clinical outcomes and post-operative activity levels has been established in the literature [1]. Moreover, promising results have been reported for concomitant lateral closing wedge osteotomy alongside reconstruction of ACL, particularly in cases of femur-originated genu varum and ACL-deficient knees [2]. While genu valgum commonly arises from femoral deformities, its etiology may vary [3]. In this study, we present a case report detailing the clinical management of a young boy experiencing symptomatic knee instability, intermittent medial knee pain, and a history of occasional locking episodes. No studies have reported concomitant reconstruction of ACL along with distal femoral osteotomy (DFO) in ACL deficit knee with genu valgum. Very few studies have described the management of the concurrent occurrence of ACL deficiency with femoral-originated genu varus [2].
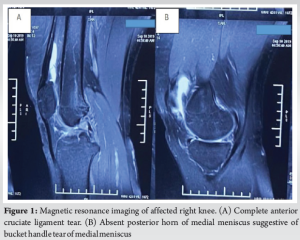
The 20-year-old male patient with a high body mass index and bilateral genu valgum presented with pain and giving way of right knee 1 year following a sports injury. The patient reported no significant past medical or drug history. Physical examination revealed bilateral flat feet. The anterior drawer test (ADT) was found to be positive with a 10 mm anterior subluxation of the tibia. The tests for the medial meniscus, including the Lachman test and McMurray test, were positive. Other tests, such as dial, valgus/varus stress, and posterior drawer, were insignificant. His knee flexion test, done at the bedside, which is a valuable tool for predicting the deformity at tibial or femoral origin, was of femoral origin [4]. In view of obesity, pain, and noncompliance from the patient side, we were unable to conduct a pivot shift test. He had no patellofemoral instability. There was an 8mm shortening of the right lower limb. The magnetic resonance imaging confirmed the complex ACL tear of the Right knee with a bucket handle tear of the medial meniscus, as seen in Fig. 1. The Lysholm score for the patient was 48, and the International Knee Documentation Committee score was found to be 38.
Pre-operative planning
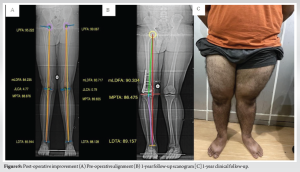
This study used scanograms of both lower limbs to assess deformity angles. The patient presented with a lateral proximal femoral angle of 95.22° and a mechanical distal femoral angle (mLDFA) of 84.23°. In addition, the medial proximal tibial angle (MPTA) was measured at 88.87°, and the lower distal tibial angle (LDTA) at 85.99°. The joint line congruence angle was 4.33°. Comparative analysis with normal mechanical axis angle values revealed a 5° increase in LPFA, a 4° decrease in mLDFA, a 2° increase in MPTA, and a 3° decrease in LDTA. This indicated that the valgus deformity primarily originated from the femur. The scanogram and clinical alignment of the patient can be seen in Fig. 2.
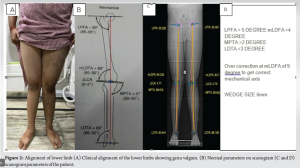
Using medical software, a plan for distal femur osteotomy was devised to correct the mechanical axis. Overcorrection at mLDFA (9° with a wedge size of 6 mm) and a lateral open wedge osteotomy of the distal femur were planned in view of limb length discrepancy (8 mm shortening in the right lower limb). Subsequent all-inside ACL reconstruction using the Arthrex zig technique was also planned.
Surgical technique
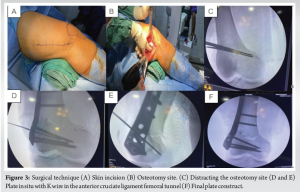
The procedure began with positioning the patient in supine position. Prophylactic dose of cefuroxime (1.5 g) and tranexamic acid (1 g) were administered through intravenous route, 30 min and 1 h before surgery, respectively. A tourniquet was tied during a surgical procedure. The ACL reconstruction was first preceded by an initial osteotomy. The distal femur was approached laterally, exposing the anterolateral surface. The site for performing osteotomy was marked 5 cm above the lateral epicondyle. Two K-wires were inserted, directed distally and medially (oblique to the joint line, aiming toward the medial epicondyle). A motorized saw was then utilized to cut the bone just above and in proximity to the K-wires, with the osteotomy carried out from lateral to medial, leaving 1 cm of bone intact on the medial side. Gradually and carefully, a gap over the osteotomy site was created using a lamina spreader, as seen in Fig. 3. Keeping the lamina spreader inferior with a 6 mm lateral wedge, the osteotomy was stabilized using a lateral distal femur locking plate and iliac crest bone graft to plug the gap due to osteotomy. This was followed by wound closure proximally.
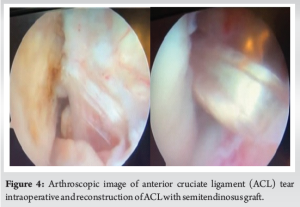
Following the diagnostic arthroscopy, which revealed an ACL tear seen in Fig. 4, a bucket handle tear of the medial meniscus, and chondral injury in the medial femur condyle, graft harvesting was performed. A semitendinosus graft was obtained and prepared into a four-fold configuration, measuring 7 cm long and 8 mm in diameter. The graft was equipped with two tight ropes and marked with fiber wire stitch at 2 cm intervals on both sides. Subsequent arthroscopy involved partial meniscectomy for the old bucket handle tear and microfracture with an awl for two chondral lesions in the medial femur condyle. The ACL stump was cleared with a shaver blade, and femur and tibial tunnels were made via an outside-in technique with an Arthrex r femur zig and flip cutter. The femur tunnel was drilled, keeping the aimer of zig in the anatomical attachment site of ACL below the lateral cortex, avoiding interference with the plate and screws. The tibia tunnel was similarly created, and the graft was passed and fixed with adjustable loops (tight rope, Arthrex r) over the bone. The positioning of the endo button of the tight rope over the femur was done just below the plate over the lateral cortex. The reconstructed ACL can be seen in Fig. 4. Thorough irrigation of the wound with normal saline was done which was followed by wound closure, and knee brace support was provided post-dressing.
Post-operative management
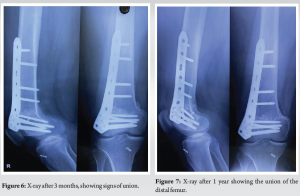
The patient was instructed to refrain from weight-bearing for 2 weeks post-operation, followed by toe-touch walking with the support of a knee brace. After 6 weeks, the patient was permitted to bear full weight after observing signs of bony union on a post-operative radiograph, as in Fig. 5. Closed-chain knee exercises commenced at the 6-week mark and were continued for more than 6 weeks until the 12-week mark. Subsequently, open-chain knee exercises were initiated and continued beyond the 12 weeks. Radiographs were done at 3 months, 6 months, and 1 year post-operative. There were signs of the union in follow-up, as seen in Figs. 6 and 7, during the post-operative evaluation of the patient.

A follow-up sonogram was done following 1 year of surgery to assess the correction of genu valgum. The values on the sonogram were compared with pre-operative measurements and the results are illustrated in Fig. 8. This comparison evaluates the surgical intervention’s effectiveness in addressing the valgus deformity and achieving the desired realignment of the lower limb.
The Lachman test for assessing the stability of the ACL was found to be negative at the 1-year follow-up. However, a 4 mm anterior translation was reported on the ADT. Despite this, no pain or instability was reported by the patient during daily activities. In addition, there was a notable improvement in the Lysholm knee score, which increased from 48 preoperatively to 91 at the 1-year follow-up. These findings suggest a favorable outcome following the surgical intervention, with significant knee function and stability improvements.
The presence of an ACL deficiency in the knee poses numerous challenges. Instances of giving away due to anterior instability might have led to the development of meniscal tears with subsequent degeneration of articular cartilage [5]. Research by Curado et al. reported that 29% of patients with ACL deficiency over a span of 22 years are affected by osteoarthritis, which ranges from moderate to severe [6]. Dejour et al. illustrated that performing reconstruction of ACL in isolation in patients with ACL deficit knees along with concurrent chondral/ meniscal injuries may paradoxically hasten the onset of OA and lead to the need for earlier re-operation [7]. Even delayed ACL reconstruction in young patients with maligned knees may correlate with a high occurrence of a secondary meniscal tear [8]. Reconstruction of ACL helps in the stabilization of the knee and encourages quick recovery from sports, but neglecting underlying issues such as genu valgum and varus can accelerate knee degeneration and osteoarthritis. A thorough evaluation that addresses concurrent conditions is essential for ensuring long-term knee health following surgery [9]. Therefore, staged or concurrent ACL reconstruction and varus-producing osteotomy are recommended among symptomatic patients of ACL deficiency along with lateral knee OA due to valgus knee. Genu valgum, a coronal plane deformity, requires correction to prevent lateral compartment osteoarthritis. The distal femur is the preferred site, as most of these deformities originate in this region. The two primary considerations are a medial closing wedge or lateral opening wedge osteotomy [10]. Lateral opening wedge osteotomy was performed on this patient. The main drawbacks of medial closing wedge osteotomy include a heightened potential for femoral artery injury and restricted access to the lateral compartment for associated procedures. Moreover, performing a medial closing wedge osteotomy presents technical complexities, necessitating meticulous pre-operative planning to ascertain the precise correction required. Intraoperative adjustments to deformity correction pose increased challenges due to these technical intricacies. However, lateral opening wedge osteotomy is more commonly practiced among surgeons, offering a technique that involves a single bone cut, facilitating more significant control over intraoperative corrections and adjustment to the mechanical axis. This method adds length to the valgus limb, proving advantageous when the extremity is shorter than its contralateral counterpart [11]. It also improves patella stability by improving alignment [2]. Though numerous studies have discussed and assessed the concurrent procedures of HTO and ACL reconstruction (ACL-R) [12-15], limited literature addresses the simultaneous undertaking of ACL-R and DFO. Given the femoral origin of the deformity, we performed the varus osteotomy in the distal femur. Numerous studies have shown evidence of elevation in the posterior tibial slope following open wedge HTO [16-20]. The anterior tibial translation rises by approximately 6 millimeters, with a 10-unit increase in the posterior tibial slope, thus exerting greater tension over the ACL [7]. In contrast, combined reconstruction of ACL with DFO does not impact the posterior tibial slope. This approach may offer the potential advantage of realigning the knee without augmenting the posterior tibial slope, unlike concurrent reconstruction of ACL and open wedge HTO. Additional research is warranted to compare the outcomes of concurrent reconstruction of ACL along with medial closing wedge and lateral opening wedge DFO, assessing their effects on the quality of life of the patient and their ability to return to sports. These studies would help in providing deeper insights into the advantages and drawbacks of each procedure, aiding in informed decision-making and optimizing patient outcomes.
Concurrent reconstruction of ACL with DFO has been reported to show favorable outcomes, including in a genu valgum patient. This combined approach offers the advantage of minimizing multiple hospitalizations and rehabilitation periods. Isolated ACL-R in patients with ACL deficiency, along with genu valgum, can have a detrimental effect on the outcome in terms of higher usage of the affected knee and exacerbation of degenerative changes of the knee joint.
This case report demonstrates the successful use of simultaneous ACL reconstruction and DFO in a young patient with bilateral genu valgum and ACL deficiency. This combined approach effectively addresses both knee instability and malalignment, offering significant clinical benefits by reducing the need for separate surgeries and minimizing recovery time. Careful surgical planning, particularly with femoral tunnel placement, is crucial to avoid complications such as plate interference.
References
- 1.Dean CS, Liechti DJ, Chahla J, Moatshe G, LaPrade RF. Clinical outcomes of high tibial osteotomy for knee instability: A systematic review. Orthop J Sports Med 2016;4:2325967116633419. [Google Scholar | PubMed]
- 2.Moradi A, Sadeghpour A, Khalilpour A. The clinical outcome of simultaneous lateral closed- wedge distal femoral osteotomy and anterior cruciate ligament reconstruction in the ACL-deficient knees with symptomatic femoral varus deformity. Arch Bone Jt Surg 2020;8:537-44. [Google Scholar | PubMed]
- 3.Kolb A, Isak V, Hobusch GM, Chiari C, Windhager R. Distal femoral varus osteotomy: Results of the lateral open-wedge technique without bone grafting. Int Orthop 2019;43:2315-22. [Google Scholar | PubMed]
- 4.Gautam VK, Maini L, Gupta R, Sabharwal A, Arora S. Flexion test in the coronal plane deformities of knee. J Clin Orthop Trauma 2013;4:115-8. [Google Scholar | PubMed]
- 5.Trojani C, Elhor H, Carles M, Boileau P. Anterior cruciate ligament reconstruction combined with valgus high tibial osteotomy allows return to sports. Orthop Traumatol Surg Res 2014;100:209-12. [Google Scholar | PubMed]
- 6.Curado J, Hulet C, Hardy P, Jenny JY, Rousseau R, Lucet A, et al. Very long-term osteoarthritis rate after anterior cruciate ligament reconstruction: 182 cases with 22-year' follow-up. Orthop Traumatol Surg Res 2020;106:459-63. [Google Scholar | PubMed]
- 7.Dejour H, Walch G, Deschamps G, Chambat P. Arthrosis of the knee in chronic anterior laxity. Orthop Traumatol Surg Res 2014;100:49-58. [Google Scholar | PubMed]
- 8.Kawashima I, Kawai R, Ishizuka S, Hiraiwa H, Tsukahara T, Imagama S. Association between knee alignment and meniscal tear in pediatric patients with anterior cruciate ligament injury. J Bone Joint Surg Am 2021;103:1604-10. [Google Scholar | PubMed]
- 9.Mortazavi SM, Noori A, Vosoughi F, Dogahe RR, Shariyate MJ. Femur originated genu varum in a patient with symptomatic ACL deficiency: A case report and review of literature. BMC Musculoskelet Disord 2021;22:437. [Google Scholar | PubMed]
- 10.O’Malley MP, Pareek A, Reardon PJ, Stuart MJ, Krych AJ. Distal femoral osteotomy: Lateral opening wedge technique. Arthrosc Tech 2016;5:e725-30. [Google Scholar | PubMed]
- 11.Mathew SE, Milbrandt TA, Young ML. Lateral opening wedge osteotomy of the distal femur for Genu Valgum: Master’s surgical technique. J Pediatr Orthop Soc North Am 2022;4:1-11. [Google Scholar | PubMed]
- 12.Bonin N, Selmi TA, Donell ST, Dejour H, Neyret P. Anterior cruciate reconstruction combined with valgus upper tibial osteotomy: 12 years follow-up. Knee 2004;11:431-7. [Google Scholar | PubMed]
- 13.Schneider A, Gaillard R, Gunst S, Batailler C, Neyret P, Lustig S, et al. Combined ACL reconstruction and opening wedge high tibial osteotomy at 10-year follow-up: Excellent laxity control but uncertain return to high-level sport. Knee Surg Sports Traumatol Arthrosc 2020;28:960-8. [Google Scholar | PubMed]
- 14.Jin C, Song EK, Jin QH, Lee NH, Seon JK. Outcomes of simultaneous high tibial osteotomy and anterior cruciate ligament reconstruction in anterior cruciate ligament deficient knee with osteoarthritis. BMC Musculoskelet Disord 2018;19:228. [Google Scholar | PubMed]
- 15.Zaffagnini S, Bonanzinga T, Grassi A, Muccioli GM, Musiani C, et al. Combined ACL reconstruction and closing-wedge HTO for varus angulated ACL-deficient knees. Knee Surg Sports Traumatol Arthrosc 2013;21:934-41. [Google Scholar | PubMed]
- 16.Ogawa H, Matsumoto K, Akiyama H. Effect of increased posterior tibial slope on the anterior cruciate ligament status in medial open wedge high tibial osteotomy in an uninjured ACL population. Orthop Traumatol Surg Res 2019;105:1085-91. [Google Scholar | PubMed]
- 17.Jacobi M, Villa V, Reischl N, Demey G, Goy D, Neyret P, et al. Factors influencing posterior tibial slope and tibial rotation in opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2015;23:2762-8. [Google Scholar | PubMed]
- 18.Lustig S, Scholes CJ, Costa AJ, Coolican MJ, Parker DA. Different changes in slope between the medial and lateral tibial plateau after open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2013;21:32-8. [Google Scholar | PubMed]
- 19.Ducat A, Sariali E, Lebel B, Mertl P, Hernigou P, Flecher X, et al. Posterior tibial slope changes after opening- and closing- wedge high tibial osteotomy: A comparative prospective multicenter study. Orthop Traumatol Surg Res 2012;98:68-74. [Google Scholar | PubMed]
- 20.Jaecker V, Drouven S, Naendrup JH, Kanakamedala AC, Pfeiffer T, Shafizadeh S. Increased medial and lateral tibial posterior slopes are independent risk factors for graft failure following ACL reconstruction. Arch Orthop Trauma Surg 2018;138:1423-31. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique
October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide