
All-inside anterior cruciate ligament reconstruction using a hamstring autograft is a minimally invasive technique that provides effective restoration of knee stability and favorable short-term functional outcomes in patients with complete ACL tears.
Arvind Karoria, Department of Orthopaedics, SRVS Medical College, Shivpuri, Madhya Pradesh, India. E-mail: medicalpublications24@gmail.com
Abstract
Background: Anterior cruciate ligament (ACL) injury is a common knee ligament injury affecting young and physically active individuals. Arthroscopic ACL reconstruction is the standard treatment for symptomatic tears to restore knee stability and function. The all-inside ACL reconstruction technique using hamstring autograft has gained popularity because of its minimally invasive nature and preservation of bone stock. This study aimed to prospectively evaluate the short-term functional outcomes of all-inside ACL reconstruction using hamstring autograft in patients with complete ACL tears.
Materials and Methods: This prospective study was conducted at Gandhi Medical College, Bhopal, and associated Hamidia Hospital. Thirty-six patients aged 18–50 years with clinically and radiologically confirmed ACL tears were included. All patients underwent arthroscopically assisted all-inside ACL reconstruction using hamstring autograft. Pre-operative evaluation included clinical examination, radiological assessment, and functional scoring using Lysholm–Tegner score, International Knee Documentation Committee (IKDC) score, and Visual Analog Scale. Patients were followed at 1, 3, and 6 months postoperatively to assess stability and functional outcomes.
Results: Most patients were aged 18–29 years, and male patients predominated. Road traffic accidents were the most common mechanism of injury. Most surgeries were performed within 1–3 months after injury. The majority of grafts measured 6–6.5 cm in length with an 8 mm diameter. Post-operative evaluation showed negative Lachman, anterior drawer, and pivot shift tests in all patients, with no varus or valgus instability. Most patients achieved excellent or good Lysholm–Tegner scores, whereas IKDC grading showed normal or near-normal knee function in all cases.
Conclusion: All-inside ACL reconstruction using hamstring autograft provides good short-term functional outcomes with restoration of knee stability in patients with complete ACL tears.
Keywords: Anterior cruciate ligament, all-inside anterior cruciate ligament reconstruction, hamstring autograft, arthroscopic surgery, knee instability, functional outcome.
The anterior cruciate ligament (ACL) is a key stabilizing structure of the knee joint that plays a crucial role in maintaining rotational stability and preventing anterior translation of the tibia relative to the femur. ACL injuries are among the most common ligament injuries of the knee and frequently occur in young, physically active individuals, particularly during sports involving pivoting, jumping, and sudden deceleration movements [1]. These injuries can result in pain, instability, and functional impairment. If left untreated, they may lead to recurrent episodes of knee giving way and an increased risk of meniscal damage and early osteoarthritis [1].
ACL reconstruction (ACLR) has become the standard treatment for symptomatic ACL tears in active patients with functional instability. The primary objectives of ACL reconstruction are restoration of knee stability, prevention of secondary intra-articular damage, and return to pre-injury levels of activity and sports participation [2]. Various graft options have been described for ACL reconstruction, including autografts, allografts, and synthetic grafts. Among these, hamstring tendon autografts are widely used because of their favorable biomechanical properties, lower donor-site morbidity, and satisfactory long-term clinical outcomes [3].
Functional outcome assessment following ACL reconstruction is commonly performed using validated scoring systems such as the Lysholm Knee Score, International Knee Documentation Committee (IKDC) score, and Tegner activity scale, which help evaluate post-operative knee stability, pain, and functional recovery [4]. Several studies have reported that ACL reconstruction with hamstring autograft provides good to excellent functional outcomes and allows most patients to return to their previous activity levels following appropriate rehabilitation [5].
In recent years, the all-inside ACL reconstruction technique has gained increasing attention. This technique utilizes socket creation rather than full tunnels on both the femoral and tibial sides and employs suspensory fixation devices. The approach is considered minimally invasive and is associated with advantages such as preservation of bone stock, reduced post-operative pain, and potentially faster rehabilitation compared with conventional techniques [6]. Clinical studies have demonstrated comparable functional outcomes and knee stability between the all-inside technique and conventional ACL reconstruction methods [7].
Despite the growing popularity of the all-inside technique, there is still limited prospective data evaluating its functional outcomes in patients with complete ACL tears. Therefore, the present study was conducted to prospectively evaluate the short-term functional outcomes of all-inside ACLR using hamstring autograft in patients with complete ACL tears.
Study design and setting
This prospective, single-center, observational clinical study was conducted in the Department of Orthopaedics at Gandhi Medical College, Bhopal, and its associated tertiary care center, Hamidia Hospital, Bhopal, India. The study included patients diagnosed with a complete ACL tear who underwent arthroscopically assisted all-inside ACL reconstruction using a hamstring autograft. A total of 36 patients meeting the eligibility criteria were enrolled. The study was conducted after obtaining written informed consent from all participants. The sample size was determined based on feasibility and the number of eligible patients presenting during the study period. As this was a prospective observational study conducted within a defined timeframe, all patients meeting the inclusion criteria were consecutively enrolled, resulting in a total sample size of 36 patients.
Inclusion criteria
Patients were included in the study if they met the following criteria:
- Patients aged 18–50 years with clinically and radiologically confirmed ACL tear
- Patients willing to undergo surgical intervention and provide consent to participate in the study.
Exclusion criteria
Patients were excluded if they had:
- Associated fractures in the involved extremity
- Concomitant major ligament injuries, such as the posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament injuries.
Pre-operative evaluation
All patients were admitted to the orthopedic ward and evaluated using a standardized case record form. A detailed clinical history was obtained, including duration of symptoms, mechanism of injury, previous treatment received, and limitations in activities of daily living.
Clinical examination included assessment of knee instability using the Lachman test, anterior drawer test, pivot shift test, and varus–valgus stress test. The neurovascular status of the affected limb was also evaluated.
Radiological investigations included plain radiography of the knee joint to rule out associated bony injuries. Magnetic resonance imaging of the affected knee was performed in patients with positive clinical findings suggestive of an ACL tear to confirm the diagnosis and evaluate associated intra-articular pathology.
Routine laboratory investigations—including complete blood count, liver and renal function tests, random blood sugar, serum electrolytes, bleeding time, clotting time, viral markers, and urine routine and microscopic examination—were performed as part of the preoperative assessment.
Functional evaluation was performed preoperatively using the Lysholm-Tegner knee score, IKDC score, and Visual Analog Scale for pain.
Surgical procedure
All patients underwent primary arthroscopically assisted ACL reconstruction using the all-inside technique under spinal anesthesia. Patients were positioned supine on the operating table with the operative limb placed at the edge of the table and a pneumatic tourniquet applied to the proximal thigh. Examination under anesthesia was performed to confirm knee instability and exclude additional ligament injuries.
Diagnostic arthroscopy was carried out using a 30° arthroscope through standard anterolateral and anteromedial portals. A systematic evaluation of the suprapatellar pouch, patellofemoral joint, medial and lateral compartments, menisci, and intercondylar notch was performed. Torn ACL remnants were debrided to identify the femoral and tibial footprints.
Graft harvesting and preparation
The semitendinosus tendon was harvested through a small longitudinal incision over the pes anserinus. The harvested tendon was cleaned of muscle fibers and prepared as a quadrupled hamstring autograft using No. 5 non-absorbable sutures with a whip-stitch technique. The graft was pre-tensioned on a tensioning board and soaked in vancomycin solution before implantation.
Femoral and tibial socket preparation
The femoral socket was created through the anteromedial portal at approximately 110–120° of knee flexion using a guide pin and cannulated reamer positioned at the center of the native ACL femoral footprint. Socket depth was calculated based on femoral tunnel length, loop length, and button length to allow adequate graft seating.
The tibial socket was created using a retrograde drilling technique with a FlipCutter system, guided at approximately 55–60° to the tibial plateau. The socket was positioned at the anatomical tibial footprint of the ACL.
Graft passage and fixation
The prepared graft was passed through the anteromedial portal into the joint and positioned within the femoral and tibial sockets using shuttle sutures. Femoral fixation was achieved using a cortical suspensory button, whereas tibial fixation was performed using an adjustable loop cortical fixation device. The knee was cycled through its range of motion multiple times to ensure appropriate graft tension and fixation stability.
Post-operative rehabilitation
A standardized rehabilitation protocol was followed for all patients. Early mobilization with controlled weight-bearing was initiated on the 1st post-operative day. Range-of-motion exercises and quadriceps strengthening were gradually introduced during the 1st few weeks. Progressive strengthening, proprioceptive training, and closed-chain exercises were incorporated during the rehabilitation period. Functional activities such as running and jumping were introduced after approximately 3 months, followed by sport-specific training in the later stages of recovery (Figures 1-5).
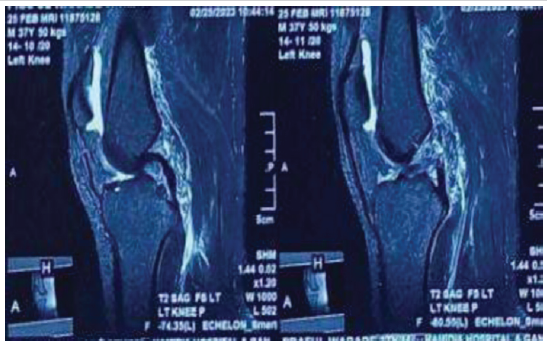
Figure 1: Pre-operative magnetic resonance imaging showing an anterior cruciate ligament tear in the left knee.

Figure 2: Post-operative X-ray.

Figure 3: Post-operative flexion.

Figure 4: Post-operative extension.

Figure 5: Post-operative squatting.
Follow-up and outcome assessment
Patients were followed postoperatively at 1 month, 3 months, and 6 months. At each follow-up visit, clinical evaluation included assessment of swelling, tenderness, and range of motion. Knee stability was assessed using the Lachman test, anterior drawer test, varus stress test, and valgus stress test. Functional outcomes were evaluated using the Lysholm-Tegner score and IKDC score during follow-up visits.
Statistical analysis
All collected data were entered into Microsoft Excel and analyzed using the Statistical Package for the Social Sciences (SPSS) software (IBM SPSS Statistics, version 25.0). Descriptive statistics were used to summarize baseline demographic and clinical characteristics. Continuous variables were expressed as mean ± standard deviation, whereas categorical variables were presented as frequencies and percentages. Comparative analysis between pre-operative and post-operative functional scores was performed using the paired Student’s t-test for normally distributed data. Changes in clinical test outcomes (Lachman test, anterior drawer test, pivot shift test) were analyzed using the McNemar test. P ≤ 0.05 was considered statistically significant. All statistical tests were two-tailed.
A total of 36 patients with complete ACL tears who satisfied the inclusion criteria were included in the present prospective study. The demographic distribution of the study population demonstrated that the majority of participants were in the younger age group, with most patients falling within the 18–29 years category, followed by the 30–39 years group, while comparatively fewer patients were in the 40–50 years age group. The study population showed a clear male predominance, with males representing the vast majority of cases, whereas females constituted only a small proportion of the participants (Table 1).
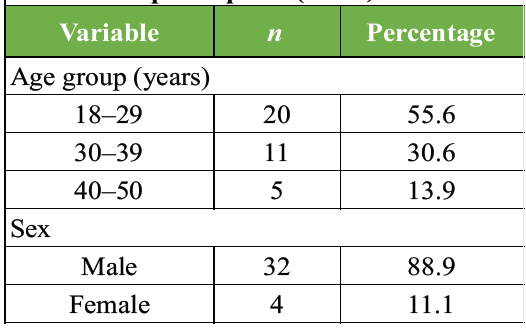
Table 1: Age and sex distribution of study
participants (n =36)
Analysis of injury characteristics indicated that road traffic accidents were the most common mechanism of injury, followed by slip and fall incidents, whereas sports-related injuries accounted for a smaller proportion of cases. With respect to the interval between injury and surgical intervention, most patients underwent surgery within 1–3 months after injury, whereas smaller proportions of patients presented either earlier or after a longer duration. Evaluation of graft parameters revealed that the majority of grafts measured within the 6–6.5 cm length range, whereas the remaining grafts were slightly longer. Similarly, most grafts had a diameter of 8 mm, with fewer patients demonstrating either smaller or larger graft diameters (Table 2).
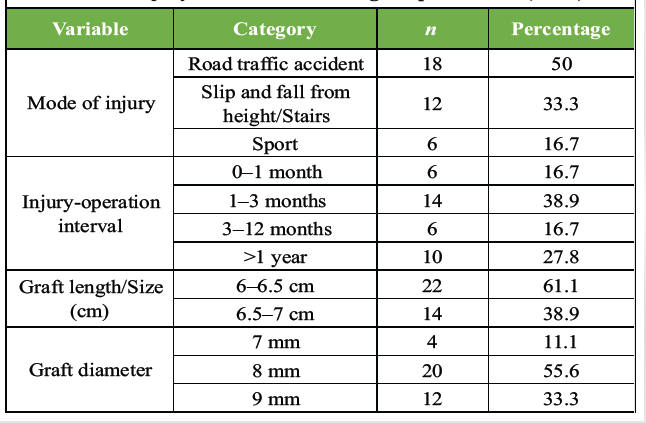
Table 2: Injury characteristics and graft parameters (n =36)
Post-operative clinical assessment during follow-up demonstrated excellent knee stability across the study cohort. All patients exhibited negative results on Lachman, anterior drawer, and pivot shift tests, and no instability was detected on varus or valgus stress testing. Furthermore, none of the patients reported post-operative episodes of knee giving way during the follow-up period, indicating satisfactory restoration of joint stability following reconstruction (Table 3).
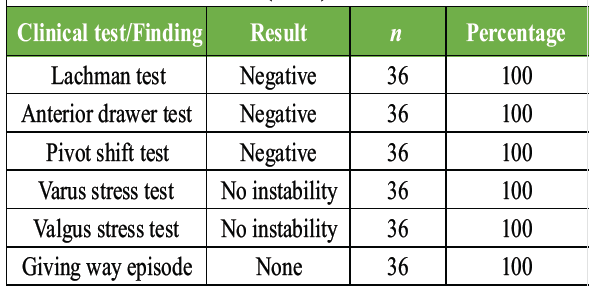
Table 3: Post-operative clinical test findings during follow-up
(n =36)
Functional outcome evaluation using the Lysholm-Tegner scoring system revealed that the majority of patients achieved outcomes classified as excellent, while a smaller proportion demonstrated good results. Only a limited number of patients fell within the fair category, and no cases were classified as poor. Overall, these findings indicated a favorable functional recovery among the study participants following the surgical procedure (Table 4).
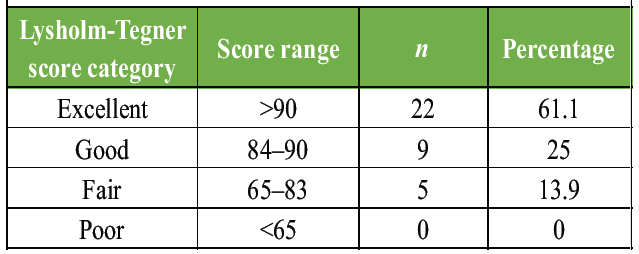
Table 4: Distribution of cases according to post-operative
Lysholm-Tegner score (n =36)
Assessment based on the IKDC scoring system further supported the positive functional outcomes observed in the cohort. Most patients were categorized as having near-normal knee function, while a substantial proportion achieved normal knee function. Notably, none of the patients fell into the abnormal or severely abnormal categories, suggesting effective restoration of knee function following all-inside ACL reconstruction (Table 5).
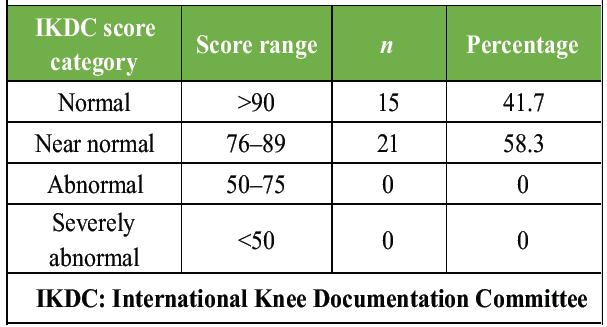
Table 5: Distribution of cases according to post-operative
IKDC score (n =36)
ACL reconstruction is widely performed to restore knee stability, functional capacity, and return to pre-injury activity levels in patients with ACL tears. The present study evaluated the functional outcomes following arthroscopic ACL reconstruction using hamstring autograft and demonstrated significant post-operative improvement in knee function, consistent with findings reported in recent literature.
Several studies have shown that arthroscopic ACL reconstruction using hamstring tendon autograft provides excellent functional outcomes with significant improvements in validated knee scoring systems. A prospective study reported that the mean Lysholm score improved markedly from approximately 49 preoperatively to around 95 at final follow-up, with nearly 90% of patients achieving excellent functional results after reconstruction [8]. Similar improvements have been documented in other prospective studies, where post-operative Lysholm scores increased to above 90, indicating restoration of knee stability and satisfactory functional recovery [9].
Systematic reviews and meta-analyses have further confirmed the effectiveness of hamstring autografts in ACL reconstruction. A recent meta-analysis evaluating outcomes in the Indian population demonstrated significant improvement in Lysholm, IKDC, and Tegner activity scores following reconstruction with hamstring tendon grafts, suggesting reliable functional recovery and improved activity levels after surgery [10]. These findings support the use of hamstring autograft as a dependable graft option for ACL reconstruction.
In addition to graft choice, surgical techniques also influence post-operative outcomes. The all-inside technique has gained popularity due to its minimally invasive nature and potential advantages such as reduced post-operative pain and faster early recovery. Comparative studies have shown that both all-inside and conventional tibial tunnel techniques result in excellent functional outcomes and comparable patient-reported outcome scores at follow-up [6]. However, early post-operative pain and rehabilitation may be slightly improved with the all-inside approach.
Other studies evaluating variations in hamstring graft preparation, such as multi-strand or five-strand graft constructs, have demonstrated significant post-operative improvements in functional scores such as IKDC and the knee injury and osteoarthritis outcome score. These techniques may help ensure adequate graft diameter and provide satisfactory knee stability with minimal complications [11]. Similarly, randomized studies comparing different hamstring graft configurations have reported significant improvement in functional outcomes regardless of the specific graft preparation method, indicating the overall reliability of hamstring tendon grafts in ACL reconstruction [12].
The functional recovery observed following ACL reconstruction is also closely related to structured rehabilitation and progressive strengthening of peri-articular musculature. Studies evaluating post-operative functional recovery have shown that the most substantial improvement in knee function occurs within the first 6–12 months following surgery, highlighting the importance of early physiotherapy and rehabilitation protocols [11].
Recent evidence continues to support the effectiveness of the all-inside ACLR technique using hamstring autograft in achieving favorable early functional outcomes. A recent systematic review and meta-analysis demonstrated that all-inside ACL reconstruction yields comparable functional scores (IKDC and Lysholm) and knee stability outcomes to conventional full-tunnel techniques, with the added benefit of reduced post-operative pain and preservation of bone stock [13]. In addition, a 2024 cohort study reported significant early improvements in patient-reported outcome measures and high rates of return to pre-injury activity levels, emphasizing the role of minimally invasive techniques in enhancing recovery [14]. Furthermore, recent clinical investigations have highlighted that all-inside ACL reconstruction is associated with low complication rates and satisfactory graft integration, contributing to reliable short-term outcomes [15]. These findings are in agreement with the present study, which demonstrated restoration of knee stability and predominantly excellent to good functional outcomes within the short-term follow-up period.
The present study has several strengths. It was conducted using a prospective study design, allowing systematic data collection and follow-up of patients undergoing all-inside ACLR. A uniform surgical technique using hamstring autograft was applied in all cases, minimizing procedural variability. Functional outcomes were assessed using validated scoring systems such as the Lysholm-Tegner score and IKDC score, enhancing the reliability of outcome measurement. In addition, all patients underwent a standardized post-operative rehabilitation protocol, which contributed to consistency in recovery assessment.
The study has certain limitations that should be acknowledged. The sample size was relatively small, and no formal sample size calculation was performed, which may limit the generalizability of the findings. The follow-up duration was limited to 6 months, restricting the evaluation of long-term outcomes such as graft durability, return to sports, and late complications. The absence of a control or comparison group (such as conventional ACL reconstruction techniques) limits the ability to compare the effectiveness of the all-inside technique directly. Furthermore, the study included only patients with isolated ACL tears, which may not reflect outcomes in patients with associated ligament injuries. Potential selection bias and single-center design may also affect the external validity of the results.
Overall, the findings of the present study align with existing literature demonstrating that arthroscopic ACL reconstruction using hamstring autograft results in significant improvement in knee function and stability with low complication rates. The procedure remains a widely accepted and effective surgical option for the management of ACL injuries, particularly in young and physically active individuals.
The present study demonstrates that all-inside ACLR using hamstring autograft is an effective surgical technique for the management of complete ACL tears, providing excellent short-term functional outcomes and satisfactory knee stability. The majority of patients achieved excellent to good functional results based on Lysholm–Tegner and IKDC scoring systems, with restoration of joint stability and absence of post-operative instability episodes during follow-up. These findings suggest that the all-inside technique is a reliable and minimally invasive approach that facilitates early functional recovery and favorable clinical outcomes in patients undergoing ACL reconstruction.
The all-inside ACL reconstruction technique using a hamstring autograft represents a reliable, minimally invasive option that preserves bone stock while effectively restoring knee stability. It is particularly suitable for young and active patients with complete ACL tears, offering excellent short-term functional outcomes. The procedure demonstrates consistent improvement in validated functional scores with low postoperative instability. Early rehabilitation combined with this technique can facilitate faster recovery and return to daily activities.
References
- 1. Belozo FL, Belozo RS, Lopes CR, Yamada AK, Silva VR. Anterior cruciate ligament: A brief narrative review of main risk factors for injury and re-injury. J Bodyw Mov Ther 2024;38:92-9. [Google Scholar] [PubMed]
- 2. Xu J, Jia Y, Zhang B, Wang X, Sun R. Comparison of the clinical outcomes between all-inside and standard technique in anterior cruciate ligament reconstruction with 6-strand hamstring tendon autograft. Orthop Surg 2024;16:1034-41. [Google Scholar] [PubMed]
- 3. Parkes CW, Leland DP, Levy BA, Stuart MJ, Camp CL, Saris DB, et al. Hamstring autograft anterior cruciate ligament reconstruction using an all-inside technique with and without independent suture tape reinforcement. Arthroscopy 2021;37:609-16. [Google Scholar] [PubMed]
- 4. Inderhaug E, Strand T, Fischer-Bredenbeck C, Solheim E. Long-term results after reconstruction of the ACL with hamstrings autograft and transtibial femoral drilling. Knee Surg Sports Traumatol Arthrosc 2013;21:2004-10. [Google Scholar] [PubMed]
- 5. Yadav D, Bhandari PB, Khanal S, Bhattachan S, Bista K, Gurung S, et al. Functional outcome of arthroscopic anterior cruciate ligament reconstruction using hamstring autograft. Nepal Orthop Assoc J 2024;10:28-30. [Google Scholar] [PubMed]
- 6. Desai VS, Anderson GR, Wu IT, Levy BA, Dahm DL, Camp CL, et al. Anterior cruciate ligament reconstruction with hamstring autograft: A matched cohort comparison of the all-inside and complete tibial tunnel techniques. Orthop J Sports Med 2019;7:2325967118820297. [Google Scholar] [PubMed]
- 7. Tavakoli Darestani R, Afzal S, Pourmojarab A, Baroutkoub M, Sayyadi S, Barati H. A comparative analysis of suture-augmented and standard hamstring autograft single-bundle ACL reconstruction outcomes: Short-term functional benefits without long-term impact. BMC Musculoskelet Disord 2023;24:971. [Google Scholar] [PubMed]
- 8. Rout S, Garg R, Patidar R, Rout S. Functional outcome of arthroscopic anterior cruciate ligament reconstruction using a quadrupled hamstring autograft: A prospective study. Cureus 2025;17:e96654. [Google Scholar] [PubMed]
- 9. Soliman SH, Refaat RH, Hadhoud MM, Sakr SA. Functional evaluation of ACL reconstruction using peroneus longus tendon autograft versus hamstring tendon autograft. Int J Health Sci 2025;9:184-93. [Google Scholar] [PubMed]
- 10. Annamalai R, Venkatramanaiah C, Sujhithra A, Vignesh N, Danis Vijay D. Functional outcome of anterior cruciate ligament reconstruction with hamstring tendon autograft in Indian population: A systematic review and meta-analysis. J Clin Orthop Trauma 2024;59:102805. [Google Scholar] [PubMed]
- 11. Raj SV, Reddy VN, Shankaran GB. Evaluation of functional recovery after five-strand hamstring autograft anterior cruciate ligament reconstruction using validated IKDC and KOOS instruments: A single-center prospective observational study in South India. Int J Environ Sci 2025;11:581-9. [Google Scholar] [PubMed]
- 12. Elshrkawy A, Eid T, Darwish A, Zalalo S. Comparative study between 6 versus 4 bands hamstring autografts for anterior cruciate ligament reconstruction. Egypt J Hosp Med 2025;100:3738. [Google Scholar] [PubMed]
- 13. Lv X, Wang M, Zhao T, Wang L, Dong S, Tan H. All-inside versus complete tibial tunnel techniques in anterior cruciate ligament reconstruction: A systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res 2023;18:127. [Google Scholar] [PubMed]
- 14. Van Haren IE, Van Der Worp MP, Van Rijn R, Stubbe JH, Van Cingel RE, Verbeek AL, et al. Return to sport after anterior cruciate ligament reconstruction – prognostic factors and prognostic models: A systematic review. Ann Phys Rehabil Med 2025;68:101921. [Google Scholar] [PubMed]
- 15. Figueroa D, Arce G, Espregueira-Mendes J, Maestu R, Mosquera M, Williams A, et al. Return to sport soccer after anterior cruciate ligament reconstruction: ISAKOS consensus. J ISAKOS 2022;7:150-61. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study February 1, 2026 Does Adding Lateral Extra-Articular Tenodesis Improve Outcomes After Arthroscopic Anterior Cruciate Ligament Reconstruction? A Longitudinal Comparative Study
February 1, 2026 Does Adding Lateral Extra-Articular Tenodesis Improve Outcomes After Arthroscopic Anterior Cruciate Ligament Reconstruction? A Longitudinal Comparative Study October 1, 2024 Arthroscopic Reconstruction of Injured Anterior Cruciate Ligament Using Peroneus Longus Graft With Fixed Loop Endobutton – A Prospective Study
October 1, 2024 Arthroscopic Reconstruction of Injured Anterior Cruciate Ligament Using Peroneus Longus Graft With Fixed Loop Endobutton – A Prospective Study