
Brachial plexus neuropraxia after ORIF of acetabulum fracture is a rare but significant complication, requiring careful patient positioning by orthopedic and anesthesia teams to prevent nerve injury.
Dr Turki Alshehri, Department of Trauma and Orthopaedic Surgery, Armed Forces Hospital Southern Region, Khamis Mushait, Saudi Arabia. E-mail: express507@hotmail.com
Abstract
Introduction: Acetabular fractures are often sustained injuries linked to high-energy trauma, such as falls from a considerable height or road traffic incidents. The modified Stoppa technique is currently used approach to treat acetabular fractures. The brachial plexus injury following open reduction and internal fixation (ORIF) of the left acetabulum fracture wasn’t reported before.
Case Report: Herein we presented a case of a 16-years-old male with a history of road traffic accident sustained an isolated close left acetabulum fracture. X-ray shows associated both column acetabulum fracture with central subluxation. He was managed with open reduction and internal fixation through a modified Stoppa approach with a lateral window. The patient underwent ORIF on the 6th day of the trauma. Fixation was done with plates and screws. At recovery room he could not move whole left upper limb and no sensation while the operated limb DNV was intact. After 15 min of recovery, sensation returned, but motor deficit persisted, indicating brachial plexus neuropraxia. The brain CT scan of was performed and unremarkable finding. After 6 months, the patient restores his sensation on his own, and improved power 5/5 of the left upper limb.
Conclusion: Long stays under general anesthesia and patient position are considerable causes of BPI. Early diagnosis (clinical/imaging) and management typically involve conservative measures, with most patients achieving full recovery. Prevention procedures are essential, including monitoring the patient and proper intraoperative positioning to avoid such nerve injury.
Keywords: Acetabulum fracture, brachial plexus neuropraxia, post-operative, stoppa approach.
Acetabular fractures are commonly occurred injuries that are related to high-energy trauma, like the road traffic accident and falling from a significant height [1]. Acetabular fractures have decreased significantly after seatbelt use became obligatory to an incidence of 3/100000 [2]. Internal fixation combined with open reduction is the most effective treatment for acetabular fractures [3]. For best results, anatomic reduction with secure column fixation is necessary [4]. However, due to its deep placement and complex anatomical structure, a surgical approach to a broken pelvis is challenging [5]. Currently, the modified Stoppa approach – described by Hirvensalo et al. [6] in 1993 and Cole and Bolhofner [7] in 1994 – is utilized for the treatment of acetabular fractures. The modified Stoppa technique is largely successful in operations. However, especially for inexperienced surgeons, the possibility of surgical complications such as vascular and nerve damage might pose a serious risk [3]. The relationship between acetabulum fractures and peripheral nerve injury has only been briefly examined in case studies that have been previously published [8-10]. Brachial plexopathies and other iatrogenic peripheral nerve injuries are well-known in clinical practice and can occur in the majority of surgical or procedural settings. Surgeons and anesthesiologists are mostly responsible for them since they generally happen during the perioperative phase [11]. The brachial plexus is a network of nerves that extends into the hand and forearm after leaving the spinal cord and passing through the axilla. It is made up of the cervical nerves C5 through C8 as well as the nerve roots of the first thoracic nerve (T1). The brachial plexus of nerves innervates the hand, forearm, arm, shoulder, and upper limb both sensory and motorly [1]. About 0.2% of all patients undergoing general anesthesia will experience brachial plexus injury (BPI) [12]. Five to 10% of all BPIs are iatrogenic, and they are often reported following orthopedic, liver, breast, and heart surgery [13]. Most of the time, the mechanism of injury is caused by the nerve tissue being stretched or compressed, and the primary therapy is supportive. The key to reducing this type of patient morbidity is prevention. Using appropriate positioning procedures and keeping in regular contact with the anesthesia team when necessary, the surgeon can reduce this risk [14]. Comprehensive data on the incidence of traumatic nerve injuries, nerve injuries as surgical complication, and their associations with fracture types, fracture locations, and surgical techniques are few. To the best of our knowledge, our case is a first case of brachial plexus neuropraxia post-open reduction and internal fixation of left acetabulum fracture through a modified Stoppa approach.
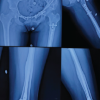
A 16-years-old male medically with a history of road traffic accident sustained isolated close left acetabulum fracture. Examination where was tenderness, restricted range of motion due pain, cannot bear weight, and distal neurovascular intact of left hip joint otherwise upper extremity examination unremarkable. X-ray shows associated both column acetabular fractures with central subluxation (Fig. 1).

Pan CT done showed an isolated left acetabulum fracture with segmented fracture of the left superior pubic rami fracture, acetabulum dissociated from the iliac bone and there is central subluxation (Fig. 2-7).
Second day of admission, emergency treatment was done for the patient in the form of left distal femur skeletal traction to reduce central dislocation and enhance the fracture complexity. Post-operation, the patient was fine, and distal neurovascular examination intact left the lower limb intact. The patient underwent ORIF on the 6th day of the trauma. Patient positioning was supine position on radiolucent Jackson table with both arms on 90° shoulder abduction over the arm support. After patient intubation, anesthesia physician inserted arterial line in the left upper extremity for better monitoring of the patient condition and Hgb assessment. After antibiotics and prepping with draping the patient, we proceeded with open reduction and internal fixation through a modified Stoppa approach with a lateral window. Fixation was done with suprapectineal Stryker plate, symphyseal recone plate, 2.7 mini fragment plate, and two posterior column screws (Fig. 8-11).

The surgery spent 10 h under general anesthesia and we are always informing the anesthesia and the nurses to monitor the patient during every trial of traction and ask them again to assess the patient positioning after that. Anesthesia team was changed after 3 PM with full endorsement was done regarding the patient condition, position, arterial line. After finishing the surgery, the drape was removed and the patient positioning found as superman position for the bilateral upper extremity which alerted the surgeon to examine the patient upper limbs motor and sensory in the recover as well as distal neurovascular of operated limb. At recovery, the patient was crying and shouting because he could not move whole left upper limb and no sensation at all while the operated limb DNV was intact. Case discussed among orthopedic team regarding the possibility of brachial plexus injury due to the patient position. Anesthesia team called to assess the patient and confirmed the examination. The neurology team consulted directly for better evaluation and clarification of this issue. The neurologist suggested either to be a stroke or brachial plexus. Stroke code was activated, and CT brain was performed and reported as unremarkable finding. After 15 min, sensation was recovered over the dorsum aspect of the left hand but there was motor deficit (power 0/5) of the left whole upper limb. He was diagnosed initially by a neurologist with brachial plexus neuropraxia due to severe hyperabduction of upper limbs. A meeting was hold with the patient and his father to clarify this issue and discuss with them the management plan. Post-operative pelvis X-ray day 1 (Fig. 12).

During post-operative assessment day 3, the patient motor condition improved as there was flicker flexion movement of left fingers except thumb (power 1/5) and flicker flexion movement of left wrist, sensation intact over the hand only. Electromyography (EMG) was done during the 1st-week post-operative, and it was unremarkable (Fig. 13). Patient during the hospitalization started on Vitamin B1, B6, and B12, and at the same time cock up splint was applied with arm sling. Furthermore, the patient was referred to physiotherapy and occupational therapy to start the rehabilitation of acetabulum fixation and left brachial plexus injury at the same time. Patient was discharged with full instruction and good analgesia, Vitamin B1, B6, B12, and anticoagulant. Furthermore, the patient father instructed to do passive ROM for the left upper limb and keep applying the cock up splint and arm sling. All post-discharge follow-up with orthopedics, neurology, and occupational therapy were explained to the patient and his father. The patient was seen post-operative 2 weeks, 6 weeks, 12 weeks, and 6 months with gradual significant, distal to proximal improvement of his left upper limb motor and sensory function (Fig. 14 and 15). During the follow-up with the neurology team, an EMG appointment was arranged 3 months after the injury, but the patient and his family missed the appointment as they lived away from Riyadh City and they noticed an improvement in symptoms.

The patient and his family understood the whole management plan from the discharge day, and they are compliance to it with full restriction to attend every appointment with orthopedic, neurology, and occupational therapy. Patient kept for bed to recliner wheelchair mobilization for 3 months then started gait training with gradual mobilization from partial to full weight bearing. The patient got full recovery of brachial plexus injury after 6 months with power 5/5 of all left upper limb joints and sensation 2/2.
Serious orthopedics injuries, acetabular fractures might present a challenging surgical case. Roughly 80% of acetabular fractures are caused by high-energy trauma, such as those sustained in road traffic accidents, while roughly 10.7% are caused by falls from a considerable height [15]. Acetabulum fractures are regarded as major injuries and occur more frequently in patients with multiple traumas [15]. Patients who have experienced hip deformity or discomfort in the past typically also have other related injuries, such as sciatic nerve palsy, hip dislocation, or fractures in the femur neck. In addition, they may exhibit damage to the surrounding structures, such as fractures to the extremities, significant abdominal viscera trauma, and chest traumas [16]. Here we presented a first case of 16-years-old male with a history of road traffic accident sustained isolated close left acetabulum fracture, with brachial plexus neuropraxia post-ORIF. The upper extremities are innervated by the intricate network of nerves known as the brachial plexus. It is formed in the posterior cervical triangle by the joining of the ventral rami of the first thoracic nerve root with the fifth, sixth, seventh, and eighth cervical nerve roots [17]. The location of the damage within the nerve pathway determines the kind of brachial plexus injury (BPI) [18]. There are several ways to harm the brachial plexus, including pressure, tension, and overstretching. Neuropraxia is the term used to describe when nerves are stretched to the point of harm [19]. Although there are several reasons why BPI occurs following surgery, the main contributions include perioperative mechanical stresses such as compression, stretching, and laceration. While laceration is frequently brought on by direct injury from the blade or needle, stretching and compression are usually brought on by inadequate limb padding and placement during surgery, excessive use of surgical retractors, extended immobility, and hematoma around the nerve [20], it also occurs in 0.2% of all patients receiving general anesthesia [12]. Inappropriate placement, particularly when arms are abducted more than 90°, advanced age (more than 60 years), lengthy operation duration (316 ± 62 min), hypotension, and hypothermia are risk factors for intraoperative blood pressure damage [21]. Regarding our case, the cause of BPI may be due to staying the patient more than ten hours under general anesthesia the superman position for the bilateral upper extremity, to avoid injuring the brachial plexus the surgery time must be taken into consideration, taking into account the most appropriate and comfortable position for the patient during surgery.The BPI can happen in two basic ways: traction and compression. A compression injury occurs when the head rotates, compressing the brachial plexus nerve root. The most prevalent type, compression neuropraxia, usually affects elderly individuals [22]. When a nerve is pushed, generally downward, traction neuropraxia develops. While less frequent than compression neuropraxia, this damage is more common in young adults and adolescents [22]. Regarding our case, he was unable to move their left upper limb and no sensation. After 15 min of partial recovery, sensation returned over the hand only, but motor deficit persisted, indicating brachial plexus neuropraxia following traction and compression injury during a lengthy procedure.Physician understanding of these entities is the most important factor in identifying peripheral nerve damage, including BP. Incisional discomfort, lack of patient awareness, and strong analgesia, which is prevalent in post-procedural care, typically cause delays in diagnosis. For a diagnosis, a thorough medical history and examination are essential. Neurologic evaluation is recommended if a neurologic impairment is identified [23]. Regarding imaging diagnosis, magnetic resonance imaging (MRI) and/or computed tomography (CT) myelography are typically used to determine BPI. The kind, location, and seriousness of the injury all affect how BPI is managed. In addition, it could cure itself or need straightforward, non-surgical treatment like physical therapy to return to normal [22]. When assessing these injuries, EMG is a valuable supplementary tool that may be used to determine if an injury is acute or chronic [23]. Regarding our case the MRI was requested by neurologist, however, we did not agree immediately post-operative. The brain CT scan of was performed and unremarkable finding for acute stroke. EMG was done during the 1st week post-operative and it was unremarkable. The treatment of peripheral nerve injuries, such as brachial plexopathy, is mostly supportive: Conservative therapy for three weeks is the first line of treatment, unless there is a suspicion of vascular problems, compartment syndrome, or an accidental cut to the nerve. Electrodiagnostics (Edx) should be carried out three weeks later. Since Wallerian degeneration is incomplete and information is unreliable, an Edx conducted before 3 weeks produces extremely poor results. Nothing else has to be done in the event of a Sunderland Type I injury because healing is typically complete and spontaneous [23]. The patient should ideally be sent to a hand surgeon who treats BPI for further care if axonotmesis is detected. Better recovery and prompt treatment are possible outcomes of early referral [14]. Regarding to our case during 6 months, the patient recovered gradually from day 1 post-operative up to full recovery after 6 months. His recovery started distal to proximal with sensation improvement before motor regardless. In the 1st month, the patient was able to do wrist and finger extension 3/5 and no elbow or shoulder movement with intact sensation. In 3rd month, he was able to do full wrist ROM flexion and extension 5/5 and elbow flexion 3/5 with restored deltoid sensation and improved power 5/5 of the left upper limb. At 6 months of fellow-up, the patient has FROM for wrist, elbow, and shoulder with motor power 5/5 and sensation 2/2. The main objective with these injuries is prevention. Reduced arm abduction, extension, and external rotation, frequent limb repositioning, keeping the head in a neutral posture, and appropriate shoulder padding in the Trendelenburg position are some of the tactics used to reduce risk [23]. One group was able to lower the incidence of BPI to 0.02% across 15,000 operations by following these suggestions [24]. A basic X-ray can be used to diagnose an acetabular fracture, but since many patients have numerous organ damage, a CT scan which is more accurate than a traditional X-ray is frequently required. Typically, plain films with Judet views and an anterior-posterior pelvis are acquired initially [2]. Regarding our case, X-ray shows ABC acetabular fracture with central subluxation. Numerous variables, such as age, male gender, heart disease, dementia, institutionalization, rehabilitation, and the cause and energy of the original injury, are linked to a patient’s death or morbidity. It is important for the patient’s rehabilitation and ought to be done following hip trauma [25]. It is extremely difficult for trauma surgeons, especially orthopedic surgeons, to treat acetabular fractures. Treating these patients may need coordination between different departments since the high-energy trauma that causes these fractures also damages internal organs and blood vessels [7]. When it comes to treating pelvic ring injuries and acetabular fractures, the modified Stoppa method is great. It can facilitate the direct reduction of the medially displaced quadrilateral surface, facilitate access to and visualization of the displaced quadrilateral surface, and provide the simple insertion of a buttress plate into the inferior pelvic brim with only one incision. In addition, it permits the afflicted acetabular dome to be directly reduced [26]. However, it has some disadvantages. For example, exposure of the quadrilateral surface may result in injury to the obturator nerve. The screw insertion angle is restricted in situations with posterior column fractures. Hernias can develop after surgery. It is known that the modified Stoppa technique can lead to wound infection, fixation failure, sciatic nerve palsy, obturator nerve injuries, and external iliac vein injuries. Additional issues including inguinal hernia, peritoneal cavity rupture, cystotomy, superior gluteal artery, lateral femoral cutaneous nerve palsy, rectus abdominis muscle atrophy, and deep vein thrombosis have also been documented [27]. Regarding our case, he was managed with open reduction and internal fixation through a modified Stoppa approach with lateral window. Fixation was done with suprapectineal Stryker plate, symphyseal recone plate, 2.7 mini fragment plate, and 2 posterior column screws.
In patients with acetabular fractures, post-operative nerve injuries were observed in the operated limb due to direct nerve injury or traction injury. Herein we presented the first reported case of left acetabulum fracture, which managed with open reduction and internal fixation of through the modified Stoppa approach, and complicated with post-operative of brachial plexus neuropraxia associated with not maintaining the patient position during a lengthy procedure.
Orthopedics surgeons and anesthesia should consider the patient positioning and try to keep the perfect positioning from pre-operative, intraoperative and post-operative period. This can be by asking all OR personnel to observe and maintain the patient position during any traction maneuver and post-traction by checking head, neck, upper extremity, and lower as well. Keep on you consideration to examine upper limbs post a lengthy procedure as well.
References
- 1.Mudawi A, Moghamis IS, Alzobi O, Babikir E, Abdelsalam S, Samhadaneh MA. Bilateral pelvic crescent fracture combined with left acetabular fracture: A case report. Int J Surg Case Rep 2022;99:107701. [Google Scholar | PubMed]
- 2.Hoge, Stephen. and Brad J. Chauvin. “Acetabular Fractures.” StatPearls, StatPearls Publishing, 4 July 2023. [Google Scholar | PubMed]
- 3.Lee H, Jo S, Lee G, Cho Y. Perioperative complications of the modified stoppa approach for the treatment of pelvic bone fractures: A single-institution review of 48 cases. J Trauma Injury 2021;35:19-24. [Google Scholar | PubMed]
- 4.Borg T, Berg P, Larsson S. Quality of life after operative fixation of displaced acetabular fractures. J Orthop Trauma 2012;26:445-50. [Google Scholar | PubMed]
- 5.Kim HY, Yang DS, Park CK, Choy WS. Modified stoppa approach for surgical treatment of acetabular fracture. Clin Orthop Surg 2015;7:29-38. [Google Scholar | PubMed]
- 6.Hirvensalo E, Lindahl J, Bostman O. A new approach to the internal fixation of unstable pelvic fractures. Clin Orthop Relat Res 1993;297:28-32. [Google Scholar | PubMed]
- 7.Cole JD, Bolhofner BR. Acetabular fracture fixation via a modified stoppa limited intrapelvic approach. Description of operative technique and preliminary treatment results. Clin Orthop Relat Res 1994;305:112-23. [Google Scholar | PubMed]
- 8.Dunbar RP Jr., Gardner MJ, Cunningham B, Routt ML Jr. Sciatic nerve entrapment in associated both-column acetabular fractures: A report of 2 cases and review of the literature. J Orthop Trauma 2009;23:80-3. [Google Scholar | PubMed]
- 9.Yang KH, Han DY, Park HW, Park SJ. Intraarticular entrapment of the obturator nerve in acetabular fracture. J Orthop Trauma 2001;15:361-3. [Google Scholar | PubMed]
- 10.Fassler PR, Swiontkowski MF, Kilroy AW, Routt ML Jr. Injury of the sciatic nerve associated with acetabular fracture. J Bone Joint Surg Am 1993;75:1157-66. [Google Scholar | PubMed]
- 11.Birch R, Bonney G, Dowell J, Hollingdale J. Iatrogenic injuries of peripheral nerves. J Bone Joint Surg Br 1991;73:280-2. [Google Scholar | PubMed]
- 12.Kline DG, Judice DJ. Operative management of selected brachial plexus lesions. J Neurosurg 1983;58:631-49. [Google Scholar | PubMed]
- 13.Dawson DM, Krarup C. Perioperative nerve lesions. Arch Neurol 1989;46:1355-60. [Google Scholar | PubMed]
- 14.Daga G, Kerkar PB. Brachial plexus injury after right hepatectomy. Indian J Surg Oncol 2017;8:191-4. [Google Scholar | PubMed]
- 15.Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br 2005;87:2-9. [Google Scholar | PubMed]
- 16.Demetriades D, Karaiskakis M, Velmahos GC, Alo K, Murray J, Chan L. Pelvic fractures in pediatric and adult trauma patients: Are they different injuries? J Trauma 2003;54:1146-51. [Google Scholar | PubMed]
- 17.Riska BS, Forsén L, Omsland TK, Søgaard AJ. Clinical anatomy Snell RS. In: Clinical Anatomy. 8th ed. United States: Lippincott Williams and Wilkins; 2007. [Google Scholar | PubMed]
- 18.Sakellariou VI, Badilas NK, Mazis GA, Stavropoulos NA, Kotoulas HK, Kyriakopoulos S, et al. Brachial plexus injuries in adults: Evaluation and diagnostic approach. ISRN Orthop 2014;2014:726103. [Google Scholar | PubMed]
- 19.Brachial Plexus Injury. Available at: https://www.hopkinsmedicine.org/health/conditions-and-diseases/brachial-plexus-injuries, last accessed: 2 feb 2025 [Google Scholar | PubMed]
- 20.Go YI, Kim DS, Kim GW, Won YH, Park SH, Ko MH, et al. Recovery of brachial plexus injury after bronchopleural fistula closure surgery based on electrodiagnostic study: A case report and review of literature. World J Clin Cases 2022;10:11090-100. [Google Scholar | PubMed]
- 21.Canbaz S, Turgut N, Halici U, Sunar H, Balci K, Duran E. Brachial plexus injury during open heart surgery--controlled prospective study. Thorac Cardiovasc Surg 2005;53:295-9. [Google Scholar | PubMed]
- 22.Li H, Chen J, Wang J, Zhang T, Chen Z. Review of rehabilitation protocols for brachial plexus injury. Front Neurol 2023;14:1084223. [Google Scholar | PubMed]
- 23.Desai KR, Nemcek AA Jr. Iatrogenic brachial plexopathy due to improper positioning during radiofrequency ablation. Semin Intervent Radiol 2011;28:167-70. [Google Scholar | PubMed]
- 24.Cooper DE, Jenkins RS, Bready L, Rockwood CA Jr. The prevention of injuries of the brachial plexus secondary to malposition of the patient during surgery. Clin Orthop Relat Res 1988;288:33-41. [Google Scholar | PubMed]
- 25.Riska BS, Forsén L, Omsland TK, Søgaard AJ, Meyer HE, Holvik K. Does the association of comorbidity with 1‐year mortality after hip fracture differ according to gender? The Norwegian epidemiologic osteoporosis studies (NOREPOS). J Am Geriatr Soc 2018;66:553-8. [Google Scholar | PubMed]
- 26.Jakob M, Droeser R, Zobrist R, Messmer P, Regazzoni P. A less invasive anterior intrapelvic approach for the treatment of acetabular fractures and pelvic ring injuries. J Trauma 2006;60:1364-70. [Google Scholar | PubMed]
- 27.Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified stoppa approach for acetabular fracture. J Am Acad Orthop Surg 2011;19:170-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Girl with Multiple Fractures: A Unique Case of Polytrauma
October 1, 2025 Girl with Multiple Fractures: A Unique Case of Polytrauma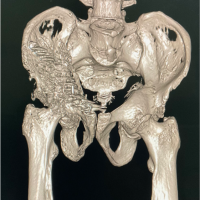 December 10, 2022 Acetabular Fracture Fixation in Paget’s Disease
December 10, 2022 Acetabular Fracture Fixation in Paget’s Disease June 9, 2021 Unusual Combination of Hip Dislocation with Ipsilateral Femoral Neck and Acetabulum Fracture: A Rare Case Report
June 9, 2021 Unusual Combination of Hip Dislocation with Ipsilateral Femoral Neck and Acetabulum Fracture: A Rare Case Report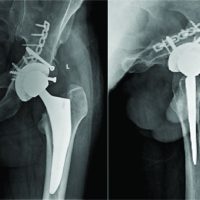 April 10, 2021 “Acute Primary Total Hip Arthroplasty for Combined Posterior Acetabulum Fracture with Ipsilateral Associated Posteriorly Dislocated Femoral Head with Femoral Neck Fracture. Using of Femoral Head as an Autograft Would be an Advantage”
April 10, 2021 “Acute Primary Total Hip Arthroplasty for Combined Posterior Acetabulum Fracture with Ipsilateral Associated Posteriorly Dislocated Femoral Head with Femoral Neck Fracture. Using of Femoral Head as an Autograft Would be an Advantage”