
Patients with infective arthritis should be carefully evaluated for uncommon organisms such as Burkholderia pseudomallei, as it can cause destructive arthritis if it is not identified early and managed adequately.
Dr. Ramesh Govindharaaju, Department of Orthopaedics, Government Medical College, Kozhikode, Kerala, India, , India. E-mail: rams.osum@gmail.com
Abstract
Introduction: Burkholderia pseudomallei, the causative agent of melioidosis, is endemic in tropical and subtropical regions, primarily in Southeast Asia and northern Australia. Cases of septic arthritis caused by B. pseudomallei in India have rarely been reported and have been described mostly in diabetic patients. This case report outlines a case of oligoarticular septic arthritis in a non-diabetic patient with a previous history of extrapulmonary tuberculosis (TB).
Case Report: A 62-year-old non-diabetic male receiving anti-tubercular therapy (ATT) for tubercular lymphadenitis presented with complaints of painful swelling of his left knee and right shoulder. Before consulting with us, he had undergone an arthrotomy and biopsy of his left knee at a different center. The biopsy was suggestive of granulomatous inflammation with negative cultures and acid-fast bacillus, for which he was advised to continue ATT for an extended duration. ATT did not improve his symptoms, and the patient developed a gradually progressing painful swelling of his right shoulder. At this point, he presented to us. Fresh cultures revealed B. pseudomallei as the causative organism. A strict regimen of intravenous ceftazidime followed by oral cotrimoxazole resulted in gradual recovery.
Conclusion: Cases of B. pseudomallei-induced infective arthritis and systemic melioidosis are now being identified in India, probably as a result of increased cross-country travel. This case report describes oligoarticular septic arthritis in a non-diabetic patient, which is unique among similar cases in the literature. A previous history of TB and negative routine cultures confounded the diagnosis.
Keywords: Burkholderia pseudomallei, infective arthritis, granulomatous arthritis, tuberculosis, ceftazidime, cotrimoxazole.
Melioidosis was first diagnosed by Captain Whitmore and Krishnaswami in 1911 in Myanmar [1]. It is a fatal disease caused by the Gram-negative obligate aerobe Burkholderia pseudomallei and is most prevalent in Southeast Asia and Northern Australia but relatively less common in the Indian subcontinent [2]. Pneumonia, skin infection, genitourinary infections, and septicemia are the usual presentations [3]. Diabetes mellitus (DM), exposure to soil or water, older age, excess alcohol consumption, chronic liver disease, chronic lung disease, chronic renal disease, and thalassemia are known risk factors [4,5]. The laboratory identification of B. pseudomallei can be difficult unless a high index of suspicion is maintained. The pale, large, wrinkled colonies look like environmental contaminants and are easily neglected. The organism grows more slowly than other bacteria that may be present in clinical samples [6]. MacConkey agar has been shown to promote good growth, but more selective media, such as Ashdown medium or Burkholderia cepacia medium, are advised. Automated culture methods such as BACTECÔ or VITEK are also very useful. Polymerase chain reaction has been suggested but is not widely available. Musculoskeletal infection due to melioidosis is not common in India, but few case reports have emerged. It mimics pyogenic bacterial infection, Gram-negative sepsis, and tuberculosis (TB) [7]. Histopathology may reveal necrotizing granulomas without acid-fast bacilli, which may confuse the image with that of TB [7,8]. B. pseudomallei is sensitive to ceftazidime, amoxy-clavulanic acid, cotrimoxazole, and doxycycline but resistant to aminoglycosides, second-generation cephalosporins, fluoroquinolones, and rifamycins.
History
A 62-year-old male presented to the Orthopaedics Department at Government Medical College and Hospital, Kozhikode, with progressive pain and swelling in his left knee and right shoulder joints. He was previously diagnosed with extrapulmonary (TB lymphadenitis) approximately 1.5 years prior, and he was already under anti-tubercular therapy (ATT). Before presenting to us, he had already undergone an arthrotomy and lavage in his left knee. Routine cultures were apparently negative, and GeneXpert did not yield any tubercular bacilli, but a biopsy of synovial tissue revealed granulomatous inflammation. Hence, it was assumed that the arthritis was due to tubercular etiology and that the negative GeneXpert was probably because the patient was already taking ATT. However, continuing further treatment for TB did not improve his joint symptoms, and he developed similar complaints in his right shoulder, at which point he presented to us.
Clinical examination
On examination, the patient was non-ambulant due to knee pain. His left knee revealed diffuse swelling, with prominent muscle wasting in his thigh and calf. The surgical scar of his arthrotomy was healed by primary intention in its proximal three-fourths, but the distal extent exhibited some granulation tissue and seropurulent discharge (Fig. 1). The joint was tender to touch, swollen, slightly erythematous and had a fixed flexion deformity of 20° and varus laxity with an arc of motion from 20 to 90°. Movements were associated with crepitus. Further flexion was limited by pain and spasms. The right shoulder exhibited mild swelling, with wasted muscles and a painful range of motion. There was no discharging sinus. The degree of abduction was <45°, and all other movements were grossly restricted.

Investigations
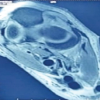
Blood parameters revealed a total leucocyte count (TLC) of 9300 cells/mm3, an erythrocyte sedimentation rate (ESR) of 86 mm/h, and a C-reactive protein (CRP) concentration of 72 mg/L. Plain anteroposterior radiographs revealed peri-articular osteopenia and advanced arthritis of the left knee joint with grossly reduced and uneven joint space (Fig. 2a). The femoral condyles revealed gross destruction with irregular margins and loss of the normal convex contour. The medial tibial condyle was excavated, and the patella subluxated laterally. The lateral radiograph revealed some lysis in the anterior aspect of the proximal tibia and osteophytes (Fig. 2b). The right knee appeared normal for his age. Severe joint destruction with loss of normal femoral and tibial condylar morphology is highly suggestive of tubercular arthritis of the knee or advanced neuropathic arthropathy. A plain radiograph of the right shoulder revealed moderate degenerative changes, including joint space reduction, loss of normal humeral head morphology, and superior migration of the head (Fig. 2c), possibly due to concomitant rotator cuff pathology. However, owing to the more recent involvement, the destruction was not as advanced as that in the left knee. Ultrasonography of both joints revealed heteroechoic collections and thickening of the overlying skin and subcutaneous tissues.

Differential diagnosis
- Tubercular arthritis
- Advanced neuropathic arthropathy (Charcot’s joint)
- Septic arthritis with atypical or uncommon bacteria.
Management
The patient underwent an incision and drainage from his right shoulder. Pus and tissue samples were collected for biopsy and culture. A synovial biopsy (Fig. 3) from the patient’s left knee was taken for culture and histopathological analysis. Aspirate and biopsy samples from both sites were sent for microscopy with Gram staining, acid-fast bacillus, and routine culture. GeneXpert was negative. Histopathological examination, however, shows granulomatous inflammation with necrosis, increasing the suspicion of multifocal TB arthritis, especially given the previous history of extrapulmonary TB. The samples were tested for atypical bacteria through BACTECÔ, which is an automated culture method that enhances the growth and detection of fastidious organisms, significantly improving diagnostic sensitivity compared with conventional blood culture techniques. This method works by detecting CO2 production as an indicator of microbial growth, allowing for earlier identification of infections. The culture on MacConkey agar showed a non-lactose-fermenting, pale, colorless colony with a wrinkled or crinkled appearance (Fig. 4), which is characteristic of B. pseudomallei. Although the ashdown medium is more specific for B. pseudomallei (containing gentamicin to inhibit Gram-negative enteropathogens), this culture enabled us to isolate the organism, which, through Gram staining, depicted the characteristic safety pin appearance (Gram-negative, bipolar rods) (Fig. 5) of B. pseudomallei. At this stage, we consulted with the infectious disease specialist and started ceftazidime 2 g intravenous for 4 weeks (acute phase), followed by oral cotrimoxazole (trimethoprim-sulfamethoxazole) for 6 months (maintenance phase).



One month after initiating targeted antimicrobial therapy, the patient’s wounds healed completely, and by the end of 2 months, his pain and swelling had improved (Fig. 6). However, the destruction caused by chronic infective arthritis caused difficulty walking and painful knee and shoulder movements. The patient was followed up for a total of 18 months, and joint aspirates were negative for B. pseudomallei at this time. The TLC was 8200 cells/mm3, the ESR was 32 mm/h, and the CRP concentration was <6 mg/L. The patient was advised total knee arthroplasty for advanced arthritis of his left knee and reverse shoulder arthroplasty for his right shoulder to improve his quality of life.

Most cases in the literature describe musculoskeletal melioidosis in patients with poorly controlled diabetes. In 2007, Karuppal et al. described a case of septic arthritis of the knee in a 32-year-old diabetic male from Northern Kerala caused by B. pseudomallei [9]. In 2020, Parija et al. described a similar case in a diabetic patient from Raipur [10]. In 2021, Deb et al. [11] described a case of knee septic arthritis in the Andaman and Nicobar Islands in a 42-year-old diabetic male who underwent arthrotomy, culture, and recovery with targeted antibiotics. Saluja et al. in 2024 [6] described a case of multifocal osteomyelitis in a 45-year-old male from Tamil Nadu with uncontrolled diabetes. Jain et al. in 2023 described a case of lumbar infective spondylodiscitis caused by co-infection of melioidosis and TB in a 63-year-old diabetic farmer, which highlighted the fact that a patient with extrapulmonary TB can have a co-existing infection with B. pseudomallei at the same or different site and that all attempts should be made to arrive at an accurate diagnosis before initiating targeted therapy [12]. These reports are also consistent with the 10-year retrospective study of melioidosis in South China by Wu et al. [13], who reported that DM was the most common predisposing factor (38/44 patients, 86.4%), followed by hepatic disorders, hypertension, and chronic kidney disease. Previous tubercular infection in our patient suggested an immunocompromised state even without diabetes, which most likely acted as a risk factor for the development of uncommon infections, such as B. pseudomallei.
B. pseudomallei-induced septic arthritis is rare, but in the last decade, a few emerging cases have been reported in various parts of India. This could be a result of underreporting of such cases or due to increasing air travel to endemic areas. This case highlights the importance of considering melioidosis in patients with persistent or atypical arthritis, even in non-diabetic patients. A history of TB and negative routine cultures may confound the diagnosis, but a high index of suspicion must be maintained, and early identification through automated cultures and specific culture media and prompt initiation of targeted antibiotics are crucial in preventing rapid joint destruction.
B. pseudomallei should be considered in chronic or atypical septic arthritis, even in non-endemic regions, even when routine cultures are negative, or when TB is suspected.
References
- 1.Whitmore A, Krishnaswami CS. A hitherto undescribed infective disease in Rangoon. Ind Med Gaz 1912;47:262-7. [Google Scholar | PubMed]
- 2.Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev 2002;15:527-44. [Google Scholar | PubMed]
- 3.Thin RN, Brown M, Stewart JB, Garrett CJ. Melioidosis: A report of ten cases. Q J Med 1970;39:115-27. [Google Scholar | PubMed]
- 4.Jain VK, Jain D, Kataria H, Shukla A, Arya RK, Mittal D. Melioidosis: A review of orthopedic manifestations, clinical features, diagnosis and management. Indian J Med Sci 2007;61:580-90. [Google Scholar | PubMed]
- 5.Cheng AC, Currie BJ. Melioidosis: Epidemiology, pathophysiology, and management. Clin Microbiol Rev 2005;18:383-416. [Google Scholar | PubMed]
- 6.Saluja SS, Kumar MM, Gopal S. A rare case of melioidosis causing multifocal osteomyelitis in an uncontrolled diabetic host. J Orthop Case Rep 2019;9:95-101. [Google Scholar | PubMed]
- 7.Punyagupta S. Melioidosis: A great imitator. Ramathibodi Med J 1983;6:147-53. [Google Scholar | PubMed]
- 8.John TJ. Melioidosis, the mimicker of maladies. Indian J Med Res 2004;119:6-8. [Google Scholar | PubMed]
- 9.Karuppal R, Marthya A, Justus S, Kumaran CM, Padinjareyil G. Burkholderia pseudomallei - a rare cause for septic arthritis. Joint Bone Spine 2007;74:659-60. [Google Scholar | PubMed]
- 10.Parija D, Kar BK, Das P, Mishra JK, Agrawal AC, Yadav SK. Septic arthritis of knee due to Burkholderia pseudomallei: A case report. Trop Doct 2020;50:254-7. [Google Scholar | PubMed]
- 11.Deb S, Singh M, Choudhary J, Jain VK, Kumar S. A rare case of knee septic arthritis by Burkholderia pseudomallei: A case report from a tertiary care Hospital of Andaman and Nicobar Island. J Orthop Case Rep 2021;11:20-3. [Google Scholar | PubMed]
- 12.Jain M, Ratna HVK, Mohanty S, Padhi S, Tripathy S. Coinfection of melioidosis and tuberculosis causing infective lumbar spondylodiscitis: A rare case report. JBJS Case Connect. 2023 May 12;13(2). doi:10.2106/JBJS.CC.22.00770. PMID: 37172118. [Google Scholar | PubMed | CrossRef]
- 13.Wu H, Wang X, Zhou X, Chen S, Mai W, Huang H, et al. Osteomyelitis and septic arthritis due to Burkholderia pseudomallei: A 10-year retrospective melioidosis study from South China. Front Cell Infect Microbiol 2021;11:654745. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report
July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report
May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting
February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting