
Multifocal non-contiguous spinal tuberculosis can be favorably managed with a combination of early diagnosis, aggressive surgical management, and tailored chemotherapy.
Dr. Sathish Muthu, Department of Orthopaedics, Orthopaedic Research Group, Coimbatore, Tamil Nadu, India. E-mail: drsathishmuthu@gmail.com
Abstract
Introduction: Multifocal non-contiguous spinal tuberculosis (MSTB) is a rare pathology, often described as a manifestation of delayed presentation, neglected illness, or disease in immunocompromised individuals. The non-contiguous spread is attributed to the valveless nature of venous drainage to the spinal column. This unique vascularity enables the infection to spread randomly across different spinal regions. These atypical presentations can cause a diagnostic dilemma and may be confused with neoplastic pathologies. MSTB is also associated with a higher incidence of neurological adversities.
Case Report: This report describes the experience with three patients (ages 22–45) presenting with progressive neurological deficits and back pain. None of the patients had a prior tuberculosis (TB) history. Magnetic resonance imaging revealed multifocal, non-contiguous spinal lesions involving the cervical, thoracic, and lumbar segments, showing vertebral destruction and cord compression. All patients underwent aggressive surgical intervention, including multilevel decompression, debridement, and long-segment stabilisation. The diagnosis of spinal TB was confirmed by histopathology and cartridge-based nucleic acid amplification test. Following surgery and supervised anti-tubercular therapy, all patients demonstrated neurological recovery.
Conclusion: MSTB without pulmonary involvement is rare. This series emphasizes that a combination of early diagnosis, aggressive surgical management, and tailored chemotherapy can lead to favorable outcomes. The cases highlight the importance of recognising atypical spinal TB presentations and adopting a multidisciplinary treatment approach.
Keywords: Spinal tuberculosis, tuberculosis, spine, surgery, non-contiguous, case report.
Multifocal spinal tuberculosis (MSTB) is a rare pathology, often described as a manifestation of delayed presentation, neglected illness or disease in immunocompromised individuals [1,2]. Non-contiguous spread in such MSTB is attributed to the valveless nature of venous drainage to the spinal column [3,4]. This peculiar vascularity enables the infection to randomly spread across different regions of the spine, beyond the limitations imparted by adjacent tissue barriers [5,6]. Such lesions can cause a diagnostic dilemma and may be confused with neoplastic pathologies or osteoporotic fractures [7,8,9]. MSTB is also associated with high complications, especially a higher incidence of neurological adversities [4,5,10]. We hereby describe our experience with 3 patients, who were managed with a combination of complex surgical intervention and anti-tubercular therapy (ATT). The cases have been presented for the rarity of such presentations, interesting management strategies, and challenges encountered in their treatment. Written informed consent was obtained from all patients for publication of the clinical details and accompanying images. Each patient was informed that data concerning their case would be submitted for publication, and all agreed to its use for academic and research purposes.
Case 1
A 24-year-old male presented with persistent upper back pain for 3 months, constitutional symptoms (fever, loss of weight and appetite) for 1 month, progressive gait instability (bedridden for 1 week), and bladder involvement (48 h). He was already initiated on 1st line ATT (elsewhere) without histopathological confirmation. On examination, there was a palpable, tender gibbus at T6-T8, with frank upper motor neuron (UMN)-type neurological involvement (Frenkel-C). On imaging (plain radiographs, computed tomography [CT], magnetic resonance imaging [MRI]), a potential diagnosis of MSTB disease (non-contiguous; significant T7-T8 vertebral collapse, T11-T12 disease, left L2 disease, L5-S1 left pedicle/vertebral disease, significant epidural collection/granulation tissue at T7-T8 and T10-T12) was made (although aggressive neoplastic lesions like lymphoma were also considered; Fig. 1a-k).
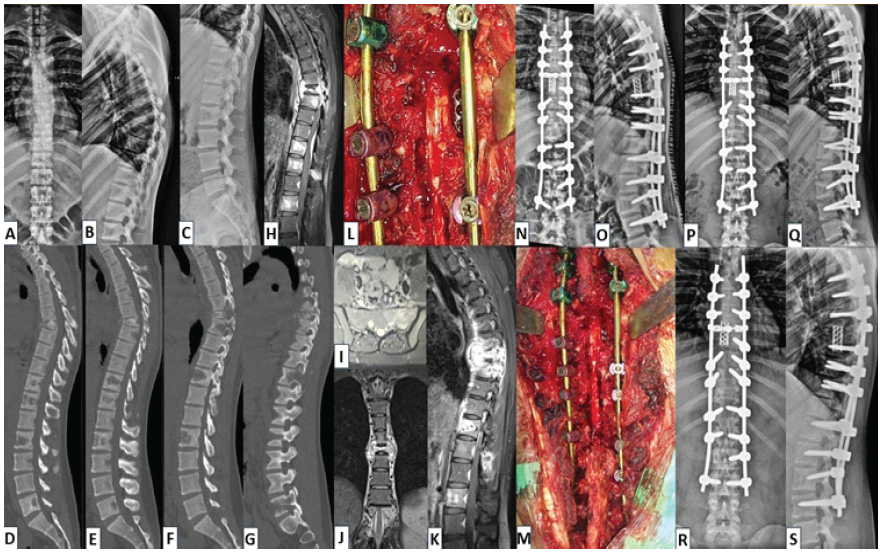
Figure 1: (a and b) Case 1 – Radiological findings pre-operative X-rays: Antero-posterior (AP) and lateral views of thoracolumbar spine showing increased haziness and collapse of T7, T8 vertebrae, (c) Lateral view of lumbar spine showing lytic lesions in the vertebral bodies of T11, T12, L2, (d and e) Mid-sagittal computed tomography (CT) sections showing complete collapse of T7, T8 vertebrae with focal kyphosis around 20°, (f and g) Para-sagittal CT sections showing multi-level lytic lesions at T7, T8, T11, T12, L2, L5, (h) mid-sagittal sequence of contrast-enhanced magnetic resonance imaging (CE-MRI) image showing hyperintense signals in pre-vertebral and epidural regions suspicious for granulation tissue with T7 collapse and T11, T12, L2 hyperintense areas with preserved vertebral height, (i) axial section of CE-MRI showing abscess within left vertebral body and pedicle of sacrum, (j) coronal section of CE-MRI showing bilateral para-vertebral abscess and granulation tissues at T7-8 level, (k) sagittal section of CE-MRI showing complete destruction of T7-T8 vertebrae with paravertebral abscess at T12 level, (l and m) intra-operative images showing decompression of the thecal sac, anterior cage reconstruction and posterior instrumentation, (n and o) immediate post-operative AP and lateral radiographs showing long-segment posterior instrumentation and cage construct, (p and q) follow-up radiographs at 3 months showing good implant position and healing, (r and s) follow-up radiographs at 12 months showing good bony fusion at T7,T8 levels and satisfactory healing.
In view of worsening neurodeficit, the decision to go ahead with immediate surgical intervention (without prior biopsy) was made. The surgical steps included T4-L3 posterior instrumented fusion, laminectomy between T7 and T12, T7/T8 corpectomies, and debridement of unhealthy granulation tissues. L5-S1 lesion was managed conservatively at this point, with a potential plan of distal extension (in case of additional deterioration; Fig. 1 l and m).The histopathological examination (HPE) report was suggestive of tubercular infection (with granuloma). Gene Expert and tubercular culture were negative. He was started on ATT (1st line) based on the HPE and clinico-radiological presentation. At 6 weeks, barring some residual UMN findings, his neurological status had almost completely recovered. He responded well to ATT clinically, and his inflammatory markers also gradually improved. At 9 months, MRI revealed complete resolution of all lesions. ATT was discontinued at the end of 10 months (Fig. 1n-s). Patient is clinically stable with 18 months of follow-up.
Case 2
A 43-year-old lady presented with worsening pain over the cervicothoracic region (6 months) and recent-onset weight loss of 7 kg. She was treated by a non-allopathic practitioner for 3 months. Her X-ray revealed a semi-segmented hemivertebra (mixed formation-segmentation defect) at T6-T7. There was significant tenderness at the upper thoracic and thoracolumbar levels. Neurological examination was normal. Imaging studies (X-rays, CT and MRI) suggested a potential diagnosis of MSTB with non-contiguous involvement (T3-T4 spondylodiscitis [with partial destruction of right T4], T9-T10 spondylodiscitis [with T10 left-sided vertebral destruction], large granulation tissue on right and left paravertebral regions at T3-T4 and T10, respectively; and compressive epidural granulation tissue at both levels; Fig. 2a-k). CT-guided biopsy revealed a diagnosis of tubercular granuloma.
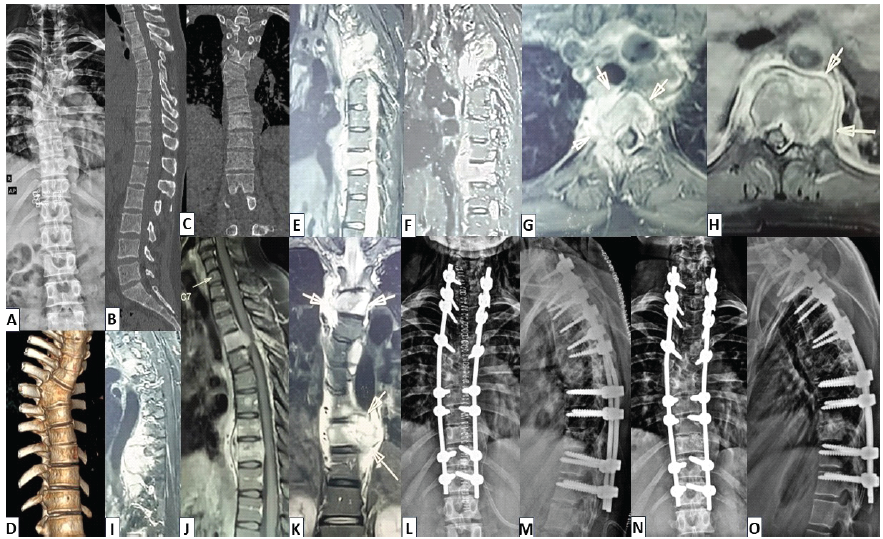
Figure 2: (a) Case 2 – radiological findings: Antero-posterior (AP) view of plain thoracolumbar radiograph showing right T6 hemivertebra with T6-T7 mixed formation-segmentation vertebral anomaly, (b) mid-sagittal section of computed tomography (CT) image showing end-plate irregularities at T3-T4 and T9-T10 levels (c and d) CT images – coronal and 3-D reconstruction sequences showing T6-T7 semi-segmented hemi-vertebrae (mixed formation-segmentation vertebral anomaly), (e and f) Sagittal sections-contrast-enhanced magnetic resonance imaging (CE-MRI) showing significant evidence of T3-T4 and T9-T10 spondylodiscitis with large granulation tissue on para-vertebral and pre-vertebral regions, (g and h) axial sections of CE-MRI showing partial destruction of right T4 vertebral body with large granulation tissue, left-sided vertebral destruction at T10 (with abscess/granulation tissue) and compressive epidural granulation tissue at both levels, (i) left para-sagittal section – short tau inversion recovery sequence of MRI showing extensive hyperintensity (S/O granulation tissue) at T9-T10 level, (j) mid-sagittal section of T2WI-MRI showing T3-T4, T9-T10 spondylodiscitis and pre-vertebral granulation tissue/abscess, (k) coronal section of CE-MRI showing para-vertebral granulation tissue at T3-T4 and T9-T10 levels, (l and m) immediate post-operative images showing C6-T12 posterior instrumented stabilisation, laminectomy from T2-T5 and T8-T11 levels, partial corpectomy of T4,T10 and reconstruction using iliac crest bone grafting, (n and o) follow-up plain radiographs-AP and lateral views at 6 months showing good implant position and satisfactory healing.
In view of disease severity, surgical debridement with cord decompression and long-segment instrumented fusion was planned. Considering intervening anomalous vertebrae at T6-7, the patient underwent C6-T12 posterior instrumented stabilisation, laminectomy from T2-T5 and T8-T11, circumferential decompression at T3-T4 and T9-T10 with partial corpectomy of T4 and T10, debridement of unhealthy granulation tissues, reconstruction at corpectomy levels with iliac crest bone graft, followed by posterior fusion with bone graft (at C6-T12; Fig. 2l-o). Tissue HPE, molecular tests and TB culture revealed the diagnosis of tuberculosis (TB). Surgery was followed by 1st-line ATT. She has completed 10 months of therapy, demonstrated clinical and radiological healing, and now remains stable with 16 months of follow-up.
Case 3
Another similar multilevel (cervical and thoracic) TB (biopsy-proven) in a 74-year-old male (with multiple comorbidities – diabetes, coronary artery disease and renal disease) is presented in Fig. 3. He had severe myelopathy and neurodeficit at presentation (Frenkel-C). The patient had a successful recovery after adequate chemotherapy for 11 months and was clinically stable with 14 months of follow-up.
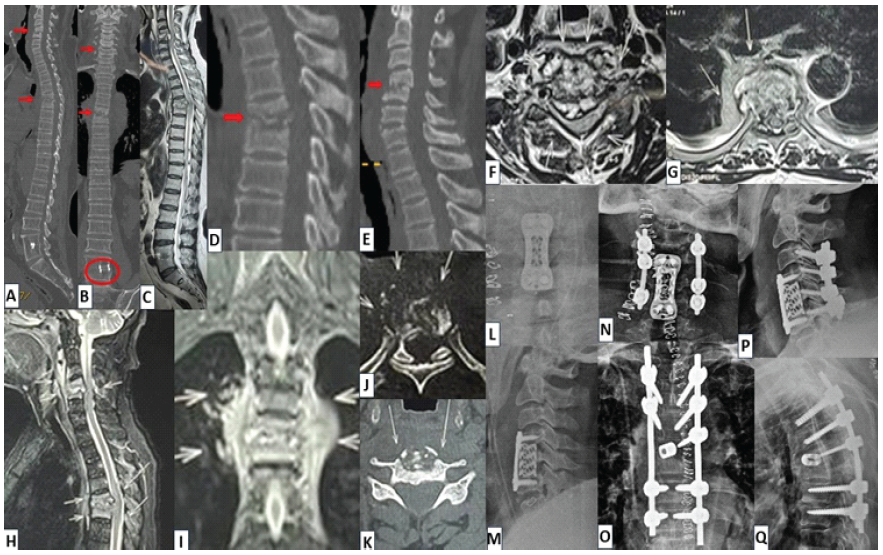
Figure 3: (a and b) Case 3 – radiological findings: Para-sagittal and coronal computed tomography (CT) images (of whole spine) showing destruction at C4-C5 and T5-T6 vertebral levels (evidence of previous surgery at L4-L5 level with interbody metallic cage), (c) mid-sagittal section of whole spine T2WI-magnetic resonance imaging (MRI) showing large epidural abscess at C4-C5 and T5-T6 levels with severe compression over spinal cord, (d and e) mid-sagittal CT sections showing destruction at C4-C5 and T5-T6 levels, suggestive of possible spondylodiscitis, (f and g) axial sections of T2WI-MRI showing large epidural abscesses with severe compression over spinal cord at C4-C5 and T5-T6 levels, (h) mid-sagittal sections of CE-MRI showing pre-/para-vertebral and large epidural abscess at C4-C5 and T5-T6 levels, (i) mid-coronal sections of short tau inversion recovery sequence on MRI showing large paravertebral abscess/granulation tissue at T5-T6 level, (j and k) axial sections of CT imaging showing severe bone destruction of T5 and C5 vertebral bodies, (l and m) stage 1: Post-operative AP and lateral radiographs showing C5 corpectomy with spinal decompression and C4-C5 fusion with Harm’s cage-plate construct, (n-q) stage 2: Post-operative radiographs showing the final constructs at the cervical and thoracic levels (360° fusion constructs).
Multifocal spread from spinal TB has been associated with factors like extremes of age, poor immunity, comorbidities, multidrug resistance, delayed presentation/ missed diagnosis, poor compliance or inadequate therapeutic dosing, lower socioeconomic status, and lack of awareness [2,3,5,6,9,10,11]. Such presentations indicate serious illness and are fraught with poorer outcomes and higher complications, including neurodeficits, progressive deformities, multiorgan/visceral involvement, higher morbidity, medication-related adversities (due to the need for higher drug dosing) and even mortality [12]. There are only limited reports of MSTB in the literature, with a majority being case reports of patients treated conservatively [5]. Among our patients, two presented with serious neurodeficits secondary to direct spinal cord compression from epidural abscess/granulation tissues. While two patients were young adults (one of whom had a substantial neurodeficit), one was an elderly male with multiple comorbidities. A comprehensive review of reports on patients treated surgically for MSTB is presented in Table 1. With multilevel disease (and in some situations, multi-skeletal lesions), neoplastic pathologies like malignancies (primary or secondaries) and other rarer infections like fungal/brucellar osteomyelitis must be considered [13]. Since extrapulmonary TB is paucibacillary, the yield on tubercular culture alone can be low (and diagnosis needs to be based on clinical/ radiological presentation, molecular tests and HPE [chronic granulomatous inflammation]) [2,14,15].
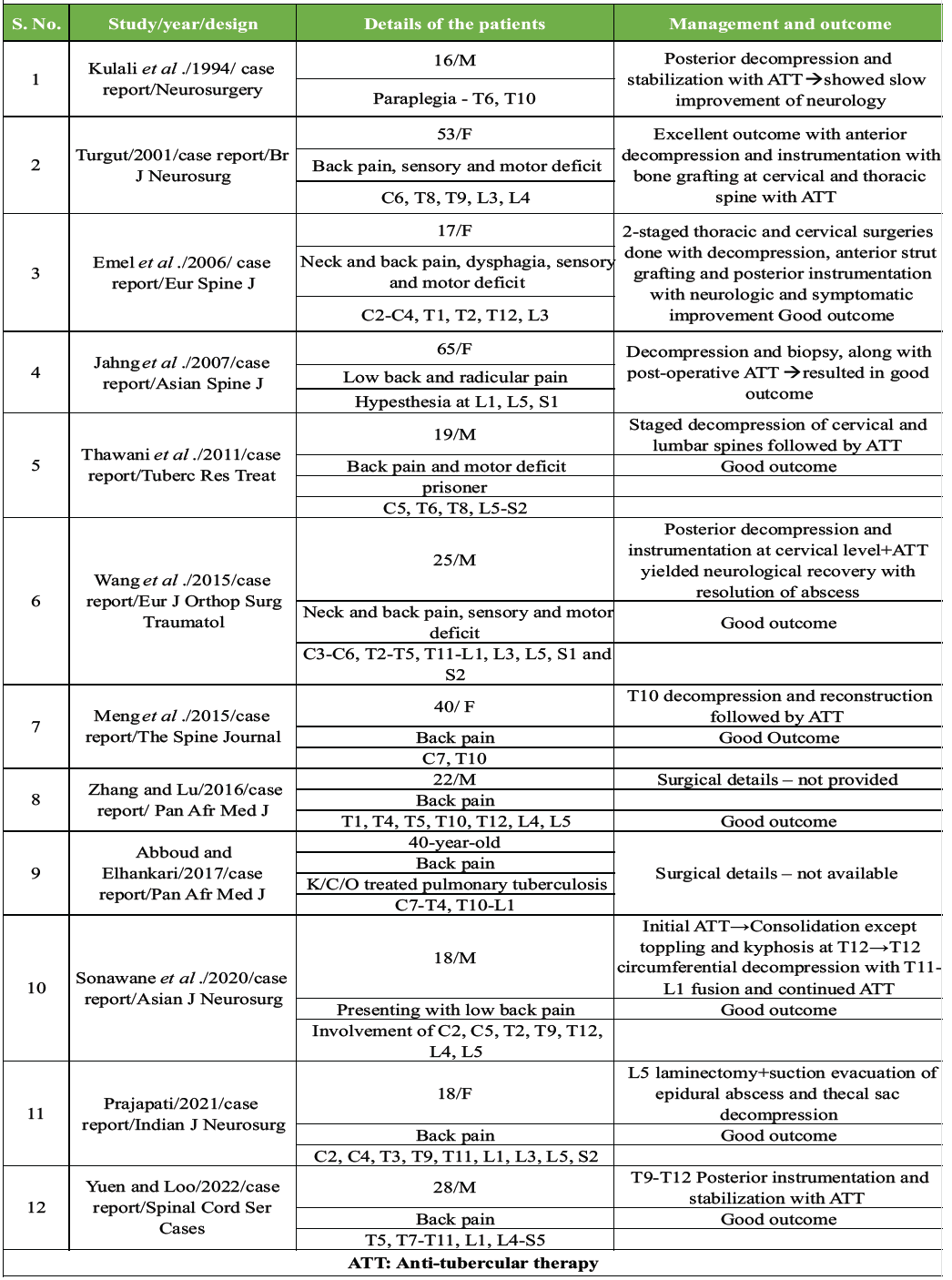
Table 1: Literature review of the case reports published on surgically-treated multifocal tubercular spinal disease
In these patients, considering the extensive nature of the disease, whenever surgical management is planned, multilevel, multistaged, long-segment interventions are typically necessary [2,5,15]. Such surgeries are best performed by highly experienced surgical teams in the best of facilities, since the risks of anaesthesia- and surgery-related morbidity (and even mortality) are high. In fact, most of the reports in the literature have involved patients who were treated with stand-alone medical therapy [5]. As previously discussed, in view of the “narrow window of opportunity” in these patients to recover (in the setting of severe disease in compromised health status), early surgical interventions in the form of thorough debridement (to decrease the bacterial load; and encourage vascularization and healing), wide decompression of spinal canal (to obviate or mitigate neurological adversities), instrumented stabilization (to enable stability and maintain intactness of the spinal column – thereby reduce the occurrence of serious deformities, instability and neurological deterioration); and drainage of any walled abscesses (to enhance drug penetration) are recommended [2,5,10]. These patients are at a high risk for developing multiple complications during the course of their treatment [2,5,12]. Considering that patients at the extremes of age and poor general condition (including immunocompromised status) are predisposed to such severe disease, morbidity and mortality related to anaesthesia and perioperative pain management are well-acknowledged. Apart from surgical-site infections and other local wound complications, implant-related issues like pseudoarthrosis, implant breakage or loosening (especially in osteoporotic bones), junctional failures or kyphosis, as well as implant malpositioning and related problems can be a major concern. Since long-term treatment with ATT (multidrug regimen and additional antibiotic therapy in situations of secondary bacterial infections) is required in all patients, chemotherapy-related adverse events are common.
Multifocal spinal TB without pulmonary involvement is rare. Early diagnosis, aggressive surgical management, and tailored chemotherapy can yield favorable outcomes. This series highlights the importance of recognising atypical spinal TB presentations and adopting a multidisciplinary treatment approach.
• Multifocal non-contiguous spinal TB is rare and can mimic neoplastic or other spinal pathologies, making early recognition essential to avoid misdiagnosis
• Patients often present with severe neurological deficits due to cord compression, highlighting the need for urgent intervention
• Aggressive surgical management with multilevel decompression, debridement, and stabilization is frequently required to achieve recovery in extensive disease
• Tailored ATT remains the cornerstone of treatment and must be guided by histopathology and molecular confirmation
• A multidisciplinary approach combining surgical expertise, medical therapy, and close follow-up leads to favorable outcomes even in complex atypical spinal TB cases.
References
- 1. Zhou J, Yang X, Hu Y, Li S. Epidemiological and osteoarticular involvement sites’ characteristics of multiple osteoarticular tuberculosis: A scoping review. Epidemiol Infect 2025;153:e26. [Google Scholar] [PubMed]
- 2. Sonawane DV, Garg BK, Jadhav KB. Extend of skipped multifocal noncontiguous spinal tuberculosis beyond imagination: A rare case report and literature review. Asian J Neurosurg 2020;15:136-9. [Google Scholar] [PubMed]
- 3. Erraoui M, Amine B, Tahiri L, El Binoune I, Bahha J, Hajjaj-Hassouni N. Noncontiguous multi-tiered spinal tuberculosis associated with sternal localization: A case report. J Med Case Rep 2017;11:181. [Google Scholar] [PubMed]
- 4. Turgut M. Multifocal extensive spinal tuberculosis (Pott’s disease) involving cervical, thoracic and lumbar vertebrae. Br J Neurosurg 2001;15:142-6. [Google Scholar] [PubMed]
- 5. Na S, Lyu Z, Zhang S. Diagnosis and treatment of skipped multifocal spinal tuberculosis lesions. Orthop Surg 2023;15:1454-67. [Google Scholar] [PubMed]
- 6. Kaila R, Malhi AM, Mahmood B, Saifuddin A. The incidence of multiple level noncontiguous vertebral tuberculosis detected using whole spine MRI. J Spinal Disord Tech 2007;20:78-81. [Google Scholar] [PubMed]
- 7. Jahng J, Kim YH, Lee KS. Tuberculosis of the lower lumbar spine with an atypical radiological presentation – a case mimicking a malignancy. Asian Spine J 2007;1:102-5. [Google Scholar] [PubMed]
- 8. Wang L, Liu L, Song Y. A rare case of atypical noncontiguous multiple spinal tuberculosis. Spine J 2015;15:e5-7. [Google Scholar] [PubMed]
- 9. Abboud H, Elhankari A. A rare case of non-contiguous multifocal spinal tuberculosis. Pan Afr Med J 2017;26:157. [Google Scholar] [PubMed]
- 10. Emel E, Güzey FK, Güzey D, Bas NS, Sel B, Alatas I. Non-contiguous multifocal spinal tuberculosis involving cervical, thoracic, lumbar and sacral segments: A case report. Eur Spine J 2006;15:1019-24. [Google Scholar] [PubMed]
- 11. Kulali A, Cobanoğlu S, Ozyilmaz F. Spinal tuberculosis with circumferential involvement of two noncontiguous isolated vertebral levels: Case report. Neurosurgery 1994;35:1154-8. [Google Scholar] [PubMed]
- 12. Meng Y, Gong Q, Liu H. A case of atypical spinal tuberculosis mimicking metastatic tumor. Spine J 2016;16:e267-70. [Google Scholar] [PubMed]
- 13. Yuen WL, Loo WL. Multifocal tuberculous osteomyelitis mimicking widespread bony metastases: Review of literature and case report. Spinal Cord Ser Cases 2022;8:23. [Google Scholar] [PubMed]
- 14. Zhang H, Lu Z. Atypical imaging of spinal tuberculosis: A case report and review of literature. Pan Afr Med J 2016;24:101. [Google Scholar] [PubMed]
- 15. Thawani M, Hale E, Habte-Gabr E. Multifocal tubercular osteomyelitis: A case with atypical manifestations. Tuberc Res Treat 2011;2011:483802. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center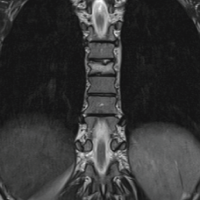 March 1, 2025 Surgical Interventions in Chronic Recurrent Multifocal Osteomyelitis Affecting the Spine: A Case Report with Literature Review
March 1, 2025 Surgical Interventions in Chronic Recurrent Multifocal Osteomyelitis Affecting the Spine: A Case Report with Literature Review December 1, 2024 Tuberculous Tenosynovitis of the Wrist: A Rare Case Report
December 1, 2024 Tuberculous Tenosynovitis of the Wrist: A Rare Case Report August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report
August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report