
A sitting imbalance may suggest the need for surgery in cases of congenital complicated kyphoscoliosis with diastematomyelia, and with appropriate planning and staged management, it is possible to restore sitting balance.
Dr. Jeevan Kumar Sharma, Spine Surgery Unit, Indian Spinal Injuries Centre, Vasantkunj, New Delhi, India. E-mail: jeev208@gmail.com
Abstract
Introduction: Sitting imbalance due to spinal deformity as an indication of surgery is very rarely encountered.
Case Report: We came across a very peculiar case of spinal deformity case who was wandering in search of treatment around multiple centers. The main concern for this 16-year-old boy from Yemen, who was born with congenital deformity with myelomeningocele and paraplegia, was sitting imbalance, which developed 2 months before presentation to our institute. Patient underwent a thorough clinical, radiological and multimodality assessment. Staged procedure of diastematomyelia excision followed by definitive posterior deformity correction was performed. Postoperatively, the patient’s sitting balance was restored with no complications.
Conclusion: Sitting imbalance can be an indication of surgery with congenital complicated kyphoscoliosis. With proper planning and staged management, the sitting balance could be achieved.
Keywords: Sitting imbalance, congenital grotesque deformity, diastematomyelia excision.
Spinal deformity contains spectrums of disorders either in the coronal (scoliosis), sagittal (kyphosis) plane, or both (kyphoscoliosis). It could be congenital, idiopathic, post-traumatic, post-infective, or neuromuscular [1]. If congenital spinal deformity is associated with intraspinal anomalies, staged surgery of intraspinal anomaly excision followed by definitive deformity correction has been a rule [2]. In an extensive study by Reames et al. with 19,360 cases of pediatric scoliosis, complication rates differed significantly among idiopathic, congenital, and neuromuscular cases. Neuromuscular scoliosis had the highest rate of complications (17.9%), followed by congenital scoliosis (10.6%) and idiopathic scoliosis (6.3%). The neurological deficit based on etiology was 2% in congenital cases, 1.1% in neuromuscular type, and 0.8% in idiopathic scoliosis. Neuromuscular scoliosis and congenital scoliosis had the highest rates of mortality (0.3% each), followed by idiopathic scoliosis (0.02%) [3]. Classification of deformity based on sitting stability described in the literature is stable – where the patient can sit normally with both arms in the air and correct balance by the gentle push to the side or forward or backward with normal trunk control. Poor – where the patient can sit without arm support but cannot regain balance if pushed gently. Unstable – cannot sit unsupported [4]. Our patient belonged to unstable sitting stability as he could not maintain to sit unsupported.
A 16-year-old male presented to our institute with a history of inability to control urine and stool and an inability to walk since childhood. He was initially able to sit and do his activities of daily living, which deteriorated for the last 2 months. Now, he needed to take support while sitting and was not able to balance while sitting (Fig. 1).

On examination – He used to drag with the support of the upper limb. His lower limbs were atrophic, with power 0/5 in the lower limbs. Lower limbs were spastic and hypertonic. A surgical scar was seen on the lower back with an associated tuft of hair around the scar of previous surgery discussed below.
He was born with myelomeningocele, which was repaired in Egypt by a neurosurgeon when he was 3 days old. After a thorough clinicoradiological workup, the patient was diagnosed with congenital thoracolumbosacral scoliosis with grotesque deformity with sitting imbalance with paraplegia with diastematomyelia with post-operated status for meningomyelocele. A neurosurgical consultation was done, and the patient was planned for surgery. Initially, the excision of diastematomyelia with posterior release was done by the neurosurgical team. It was followed by halo gravity traction for 4 days with definitive second staged posterior stabilization (Fig. 2 and 3).


Postoperatively, healing was a big challenge, but everything went well, and there were no wound complications.
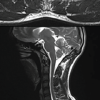
A comprehensive radiological evaluation of the patient was performed. X-ray sitting anteroposterior and lateral, computed tomography scan, and magnetic resonance imaging (MRI) were performed. A sitting X-ray demonstrated a coronal imbalance of 13.08 cm and a sagittal imbalance of 11.43 cm preoperatively (Fig. 4). MRI demonstrated diastematomyelia in addition to the deformity. Post-operative X-ray of the patient showed significantly improved deformity and reduction in coronal (13.08–5.59 cm) and sagittal imbalance (11.43–3.68 cm) (Fig. 5). Patient was able to sit properly without the need for support postoperatively. There was a significant clinical and radiological reduction in kyphoscoliosis (Fig. 6).

There were lots of challenging issues in the management of the above-discussed patient. His rejection of surgery at multiple other institutions was proof of the morbidity and challenge of the surgery and other management-related issues for the patient. The challenges discussed and planned by the surgical team at our institution were a history of surgery with surgical scar, gross deformity of the spine with costo-pelvic impingement, osteoporotic pelvic bone due to disuse atrophy, very high pelvic obliquity, and diastematomyelia present along with the deformity. Staged procedure with release, halo gravity traction, and then definitive fixation has shown great results in severe rigid deformity, reducing the risk of neurological complications involved in intraoperative manipulation [5]. Similar issues have been seen in neuropathic (Charcot) spinal arthropathy, where there is a loss of proprioception and pain sensitivity impairs the protective mechanisms of the joint, resulting in repeated stresses and microtrauma, which may initiate degenerative destruction of the affected spine segment and lead to instability and dislocation [6]. One of the main issues in such severe deformity is high pelvic obliquity, where the placement of the screw becomes very difficult, as well as risky due to the osteoporotic pelvic bone due to flailing lower limbs and trunk. It has been advised to extend spinal instrumentation to the pelvis in such cases of high pelvic obliquity. Despite the high rate of infectious complications in patients with such severe deformity, the importance of treating frontal and sagittal spinal and pelvic imbalance to avoid poor sitting posture, minimizing skin, and respiratory, and/or digestive complications has been advocated [7]. Scoliosis with pelvic obliquity is the most common deformity, especially in patients with trunk hypotonia and quadriplegia [8]. Progressive spinal deformity causes difficulty with daily care, walking, and sitting and can lead to back and rib pain, cardiac and pulmonary complications, altered seizure thresholds, and skin compromise [9]. Implementation of a Multi-D conference, multi-modality discussions, and planning led to a significant reduction in mortality in 1 year and is an important safety process to reduce serious complications after non-idiopathic scoliosis surgery [10]. Numerous factors may play a role in the contribution of this complex deformity which include asymmetric paraplegia, imbalance of mechanical forces, intraspinal and congenital anomalies of the spine, altered sensory feedback, and abnormal posture through central pathways. Physiologic impairments resulting from spinal deformity and restrictions associated with an underlying neuromuscular condition significantly impact limb movement, gait, standing and sitting posture, balance, and trunk stability [11]. Bracing has shown sitting balance and stability in most patients with low-grade idiopathic scoliosis, but patients with unstable sitting stability in cases of the neuromuscular component have shown less comorbidities, with surgical procedures with improved postures being the best long-term outcomes [4,12]. Although short-term dreaded complications such as infections and respiratory and cardiovascular complications were absent, there is a need to look for long-term complications in the near future. Elmeshneb et al. have reported the incidence rate of wound complications was the highest among all complications, at 13.3%, closely followed by respiratory complications at 11.8%. Implant failure occurred in 7.1% of cases. Gastrointestinal complications were 5.2%, pseudarthrosis in 4.6%, and neurological deficit in 2.9%. The pooled rate of revision surgery was 9.6% [13]. There have been different approaches described in the literature to manage the combination of diastematomyelia with deformity. A two-stage method encompasses the first stage of the removal of diastematomyelia, and the second stage is the correction of scoliosis after 3–6 months. However, with this method, the total duration of the operation and the total amount of blood loss are much higher [14,15]. Another approach is the one-stage correction in which both diastema resection and deformation correction are executed in one operation. During this operation, the total time of the operation is shortened and the total amount of blood loss is decreased [2,16,17]. Our approach aligns with two staged surgeries where initial diastema excision was performed, and then correction of deformity was undertaken. The previous studies undergoing single-staged surgery usually had a less deformed spine with the presentation at a young age, but taking into consideration the grossly deformed spine along with the patient’s age, we went for staged surgery. Health-care issues and educational and cultural drawbacks have been issues in global patient health care [18]. It was found to be similar in our patient, where he sought treatment at different places since his childhood, with inadequate treatment being offered at his earlier age. Health-care challenges in the place of origin of our patients included pharmacy practices [19], natural disasters [20], epidemics [21], and being resource-poor [22,23]. These might be the ethical and socioeconomic considerations for patients in search of adequate health-care needs. The limitation of our report is being a single case report with a lack of long-term follow-up and not using a functional scoring system such as SF-36, as we were just trying to demonstrate the sitting imbalance correction at the point of time for the complicated spinal deformity.
Sitting imbalance can be the indication of surgery with congenital complicated kyphoscoliosis. The surgery may be very challenging due to such grotesque deformity. With a team approach and staged management, regaining a sitting balance, even in a patient with such a grotesque deformity, is very satisfying to the patient and the operating surgeon.
A highly deformed spine can lead to sitting imbalance. The challenges in such cases are the history of surgery with surgical scar, gross deformity of the spine with costo-pelvic impingement, osteoporotic pelvic bone due to disuse atrophy, very high pelvic obliquity, and diastematomyelia present along with the deformity. The staged procedure with diastematomyelia excision, release, halo gravity traction, and then definitive fixation resulted in significant correction of severe rigid deformity with the regain of sitting balance.
References
- 1.Moon MS, Lee BJ, Kim SS. Spinal deformity. Indian J Orthop 2010;44:123-6. [Google Scholar | PubMed]
- 2.Singrakhia M, Malewar N, Deshmukh S, Deshmukh S. Simultaneous surgical treatment of congenital spinal deformity associated with intraspinal anomalies. Asian Spine J 2018;12:466-75. [Google Scholar | PubMed]
- 3.Reames DL, Smith JS, Fu KM, Polly DW Jr., Ames CP, Berven SH, et al. Complications in the surgical treatment of 19,360 cases of pediatric scoliosis: A review of the scoliosis research society morbidity and mortality database. Spine (Phila Pa 1976) 2011;36:1484-91. [Google Scholar | PubMed]
- 4.Smith RM, Emans JB. Sitting balance in spinal deformity. Spine (Phila Pa 1976) 1992;17:1103-9. [Google Scholar | PubMed]
- 5.Kalidindi KK, Sath S, Sharma J, Chhabra HS. Management of severe rigid scoliosis by total awake correction utilizing differential distraction and in situ stabilization. Interdiscip Neurosurg 2020;21:100778. [Google Scholar | PubMed]
- 6.Aebli N, Pötzel T, Krebs J. Characteristics and surgical management of neuropathic (Charcot) spinal arthropathy after spinal cord injury. Spine J 2014;14:884-91. [Google Scholar | PubMed]
- 7.Bouyer B, Bachy M, Zahi R, Thévenin-Lemoine C, Mary P, Vialle R. Correction of pelvic obliquity in neuromuscular spinal deformities using the “T construct”: Results and complications in a prospective series of 60 patients. Eur Spine J 2014;23:163-71. [Google Scholar | PubMed]
- 8.Vialle R, Thévenin-Lemoine C, Mary P. Neuromuscular scoliosis. Orthop Traumatol Surg Res 2013;99:S124-39. [Google Scholar | PubMed]
- 9.Rouissi J, Arvieu R, Dubory A, Vergari C, Bachy M, Vialle R. Intra and inter-observer reliability of determining degree of pelvic obliquity in neuromuscular scoliosis using the EOS-CHAIR® protocol. Child’s Nerv Syst 2017;33:337-41. [Google Scholar | PubMed]
- 10.Deveza L, Heydemann J, Jain M, Liu D, Chhabra B, Spoede E, et al. Reduction in mortality in pediatric non-idiopathic scoliosis by implementing a multidisciplinary screening process. Spine Deform 2021;9:119-24. [Google Scholar | PubMed]
- 11.Allam AM, Schwabe AL. Neuromuscular scoliosis. PM R 2013;5:957-63. [Google Scholar | PubMed]
- 12.Khan F, Khan A, Chinnery L, Loveridge J, Zhang J, Polychronakis T. Surgical management of neuromuscular scoliosis in paediatric patients: Experiences from a tertiary Centre multidisciplinary team. BMJ Paediatr Open 2025;9:e002456. [Google Scholar | PubMed]
- 13.Elmeshneb MA, Hassanin MA, Elnady B, Sleem A, Le GT, Patel MS, et al. Surgical complications in neuromuscular scoliosis surgery: Systematic review and meta-analysis of the last ten years. Eur Spine J 2024;33:2666-76. [Google Scholar | PubMed]
- 14.Shen J, Wang Z, Liu J, Xue X, Qiu G. Abnormalities associated with congenital scoliosis: A retrospective study of 226 Chinese surgical cases. Spine (Phila Pa 1976) 2013;38:814-8. [Google Scholar | PubMed]
- 15.Elsebaie HB, Kaptan W, El Miligui Y, El Masry MA, Salaheldine M, Noordeen HM, et al. Anterior instrumentation and correction of congenital spinal deformities under age of four without hemivertebrectomy: A new alternative. Spine (Phila Pa 1976) 2010;35:E218-22. [Google Scholar | PubMed]
- 16.Chen B, Yuan Z, Chang MS, Huang JH, Li H, Yang WZ, et al. Safety and efficacy of one-stage spinal osteotomy for severe and rigid congenital scoliosis associated with split spinal cord malformation. Spine (Phila Pa 1976) 2015;40:E1005-13. [Google Scholar | PubMed]
- 17.Hui H, Tao HR, Jiang XF, Fan HB, Yan M, Luo ZJ. Safety and efficacy of 1-stage surgical treatment of congenital spinal deformity associated with split spinal cord malformation. Spine (Phila Pa 1976) 2012;37:2104-13. [Google Scholar | PubMed]
- 18.United Nations. Department of International Economic and Social Affairs. Population Division, United Nations Fund for Population Activities UNFPA. People’s Democratic Republic of Yemen. Popul Policy Compend 1985 1-8. [Google Scholar | PubMed]
- 19.Al-Worafi YM. Pharmacy practice and its challenges in Yemen. Australas Med J 2014;7:17-23. [Google Scholar | PubMed]
- 20.Al-Hunaishi W, Hoe VC, Chinna K. Factors associated with healthcare workers willingness to participate in disasters: A cross-sectional study in Sana’a, Yemen. BMJ Open 2019;9:e030547. [Google Scholar | PubMed]
- 21.Ng QX, De Deyn ML, Loke W, Yeo WS. Yemen’s cholera epidemic is a one health issue. J Prev Med Public Health 2020;53:289-92. [Google Scholar | PubMed]
- 22.Alshakka M, Hatem NA, Al-Abd N, Badullah W, Alawi S, Ibrahim MI. Knowledge, attitude, and practice toward antibiotic use among the general public in a resource-poor setting: A case of Aden-Yemen. J Infect Dev Ctries 2023;17:345-52. [Google Scholar | PubMed]
- 23.Al-Hatemi N, Al-Nawd E, Alosoufe L, Alhebshi H, Alhroub N, Alkhawaldeh A, et al. Exploring risk factors for undernutrition in children aged under five years in Yemen. Nurs Child Young People 2024; Oct 7. doi: 10.7748/ncyp.2024.e1526 [Google Scholar | PubMed | CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 High-Grade Pancreatic Neuroendocrine Carcinoma Presenting as Dorsal Spinal Cord Compression: A Diagnostic and Surgical Challenge for the Orthopedic Oncologist
December 1, 2025 High-Grade Pancreatic Neuroendocrine Carcinoma Presenting as Dorsal Spinal Cord Compression: A Diagnostic and Surgical Challenge for the Orthopedic Oncologist August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series
August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series September 1, 2025 Asymmetrical Bilateral Complex Dislocations of the Hips: A Rare Case Report
September 1, 2025 Asymmetrical Bilateral Complex Dislocations of the Hips: A Rare Case Report August 10, 2021 Dissociation of the Glenosphere: A rare Post-operative Complication of Reverse shoulder Replacement
August 10, 2021 Dissociation of the Glenosphere: A rare Post-operative Complication of Reverse shoulder Replacement