
1) To evaluate efficacy of Fluoroscopy-guided Sacroiliac Joint Block versus Conservative Management in Sacroiliitis 2) To measure functional outcome using Visual Analog Scale (VAS), Oswestry Disability Index (ODI), and EQ-5D-5L questionnaire
Dr. Deepesh Laxman Chaudhari, Department of Orthopaedics , Chettinad Hospital and Research Institute, Chettinad Academy of Research And Education , Kelambakkam-603103 , Tamil Nadu , India. E-mail: deepeshchaudhri@gmail.com
Abstract
Introduction: Dysfunction of the sacroiliac joint is a frequently overlooked etiology for lumbosacral and gluteal pain. This study compares the efficacy of fluoroscopy-guided sacroiliac joint (SIJ) blocks versus conservative management in patients with sacroiliitis.
Materials and Methods: A prospective cohort study was done involving 88 patients diagnosed with sacroiliitis. Group I (n = 48) received conservative management, while Group II (n = 40) underwent fluoroscopy-guided SIJ blocks. Outcomes were assessed using Visual Analog Scale (VAS), Oswestry Disability Index (ODI), and EuroQol 5-Dimension 5-Level (EQ-5D-5L) questionnaire at baseline and 6 months.
Results: Significant progress was observed in both groups, but Group II demonstrated superior outcomes. The mean VAS reduction was greater in Group II (5.3 points) compared to Group I (3.1 points). Similarly, functional improvement measured by ODI was higher in Group II (55%) than Group I (39.9%). The EQ-5D-5L index value increased more substantially in Group II (0.42–0.79) than in Group I (0.41–0.67), with statistically significant differences between groups (P = 4.51 × 10−⁸).
Conclusion: Fluoroscopy-guided SIJ blocks provide significantly better pain relief, functional improvement, and life quality enhancement as compared to conservative management in patients diagnosed with sacroiliitis. This intervention should be considered for patients with inadequate response to conservative treatment.
Keywords: Sacroiliitis, sacroiliac joint block, physiotherapy, fluoroscopy.
Dysfunction of the sacroiliac joint (SIJ) is a frequently overlooked etiology of lumbosacral and gluteal pain, despite its significant prevalence in clinical practice [1,2]. Approximately 75% of chronic low back pain is often linked to specific anatomical pathologies upon thorough investigation, with sacroiliitis being a notable contributor [3]. The SIJ has a crucial role in axial load transmission and locomotion, which is considerably compromised in the presence of inflammation. Patients typically present with lumbosacral pain with gluteal radiation and potential femoral referral patterns, creating diagnostic challenges in differentiating sacroiliitis from other lumbopelvic pathologies. While thorough history and clinical examination remain essential for diagnosis, magnetic resonance imaging aids early detection. In suspected seronegative spondyloarthropathies, erythrocyte sedimentation rate, C-reactive protein, and human leukocyte antigen-B27 testing serve as valuable diagnostic adjuncts. Management of sacroiliitis prioritizes pain relief and functional improvement, with conservative therapy as the first-line approach. Physical therapy enhances pelvic stability, posture, and joint flexibility through targeted exercises, mobilization techniques, and electrotherapy. When conservative treatment proves ineffective, SIJ infiltration can be used both for therapeutic relief and diagnostic confirmation of sacroiliitis[4]. The anatomy of the SIJ necessitates image-guided techniques for accurate intra-articular delivery. Freehand injections achieve successful articulation in only 22% of cases, while fluoroscopic guidance significantly improves procedural precision and therapeutic efficacy [5]. Diagnostically, substantial post-procedural analgesia confirms the SIJ as the primary pain generator, while therapeutically, infiltration enables more effective participation in rehabilitation. Fluoroscopy-guided SIJ block is minimally invasive and can be performed as a daycare procedure [6,7]. Despite the dual diagnostic and therapeutic benefits of SIJ infiltration, there remains a significant gap in robust data regarding optimal patient selection, procedural techniques, and outcome assessment. This investigation seeks to address these knowledge gaps by evaluating the key factors influencing the efficacy and clinical outcomes of SIJ interventions.
This forward-looking study was carried out at Chettinad Hospital and Research Institute between May 2023 and May 2024, with 88 patients diagnosed with sacroiliitis. The participants were selected based on predetermined criteria.
Inclusion criteria
- The presence of localized pain over the posterior sacroiliac articulation
- Positive response to minimum one specialized sacroiliac triggering maneuver (Gaenslen’s, Patrick’s, or Yeoman’s test)
- Absence of hip pathology
- No clinical evidence of lumbosacral nerve root compression.
Exclusion criteria
- Age <18 years or more than 75 years
- Presence of seronegative spondyloarthropathies (ankylosing spondylitis or Reiter syndrome)
- Presence of not controlled diabetes
- History giving hypersensitivity reactions for local anesthetics or radiographic contrast materials
- Suspected or confirmed infectious process or osteonecrosis of the femoral head
- Inability to comply with follow-up protocol
- Cutaneous lesions or infections overlying the injection site
- Psychiatric comorbidities precluding reliable questionnaire completion.
Study design
This is a prospective cohort study that compares conservative management to fluoroscopy-guided SIJ block in patients with low back pain. Patients who met the inclusion criteria were selected for participation. Group I, the conservative management cohort, consisted of patients presenting with new-onset SIJ pain who received either no previous treatment or <4 weeks of prior treatment. These patients underwent a standardized conservative management approach for 4 weeks, which included physiotherapy and analgesics. Group II, the interventional management cohort, comprised patients who had persistent SIJ pain despite having already undergone 4 or more weeks of previous conservative treatment. These patients were selected to undergo fluoroscopy-guided SIJ blocks. Pre-procedure assessment was conducted using the Oswestry Disability Index (ODI) [8], visual analog scale (VAS), and EuroQol 5-Dimension 5-Level (EQ-5D-5L) questionnaire [9].
Procedure
Before the procedure, all participants provided informed consent. The patients were positioned prone, and the sacroiliac area was prepared and covered. Using fluoroscopy, the skin over the lower part of the SIJ was marked. A 23-gauge, 3.5-inch spinal needle was inserted at a slight upward angle. The needle’s correct placement was confirmed by injecting 0.5–1.0 mL of non-ionic contrast medium, as depicted in Fig. 1. After confirmation, a combination of 1 mL of either 0.5% bupivacaine or 2% lidocaine, along with 1 mL (40 mg) of triamcinolone acetonide, was injected into the SIJ. For patients with pain in both SIJs, injections were performed in both joints during the same session.

Follow-up and outcome assessment
Patients were monitored for pain levels, functional limitations, and potential complications throughout a 6-month follow-up period. The SIJ block was deemed successful if it led to a reduction in pain by at least 50%. Pain recurrence was defined as a return of pain >50% of the levels experienced before treatment. Treatment failure was noted if recurrence occurred within 6 weeks of the procedure. Follow-up assessments were conducted through outpatient visits or telephone consultations for those unable to attend in person. Pain intensity was recorded using the VAS (0–10), and functional impairment was evaluated using the modified Oswestry low back pain disability questionnaire. In addition, health-related quality of life was measured using the EQ-5D-5L questionnaire. All assessments were recorded pre-procedure and at the final follow-up to determine treatment effectiveness.
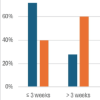
The study included 88 patients, with 48 in Group I (Conservative Management) and 40 in Group II (SIJ block). The patient demographic details are summarized in Table 1. The average age of the participants was 40.3 years, with 36 males and 52 females in the group. Among the participants, 38 complained of right-sided sacroiliitis, 27 had left-sided, and 23 had bilateral sacroiliitis. In Group I, 19 patients had left-sided pain, 17 had right-sided pain, and 12 had pain on both sides, while in Group II, 13 patients experienced left-sided pain, 16 had right-sided pain, and 11 had both-sided pain. The average period of pain before the intervention was 27.2 weeks.

Pain relief was measured using the VAS, and the results are shown in Table 2. The average VAS scores before treatment were 7.3 for Group I and 8.0 for Group II. At the 6-month follow-up, there was a notable reduction in pain levels in both groups. Group I had a mean reduction of 3.1 points, whereas Group II exhibited a greater reduction of 5.3 points (P = 0.000), indicating that this reduction is statistically significant, suggesting that the SIJ block was more effective in reducing pain compared to conservative treatment (Table 2).

With ODI assessed functional improvement, as shown in Table 3. Pre-treatment ODI scores were 68.31% in Group I and 72.9% in Group II. At 6 months, ODI scores improved to 28.3% in Group I (P = 0.000) and 17.9% in Group II (P < 0.005). The average functional improvement was 39.9% in Group I and 55% in Group II (P = 0.000), indicating superior functional recovery in the injection therapy group (Table 3).
 Quality of life was assessed using the EQ-5D-5L Index and EQ-VAS scores. Improvements were noted across all five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety or depression) at the 6-month follow-up. The EQ-5D-5L index value showed improvement from 0.41 to 0.67 in Group I and from 0.42 to 0.79 in Group II. The EQ-VAS scores increased from 47.8 to 67.2 in Group I and 48.5 to 75.8 in Group II (Table 4 and 5).
Quality of life was assessed using the EQ-5D-5L Index and EQ-VAS scores. Improvements were noted across all five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety or depression) at the 6-month follow-up. The EQ-5D-5L index value showed improvement from 0.41 to 0.67 in Group I and from 0.42 to 0.79 in Group II. The EQ-VAS scores increased from 47.8 to 67.2 in Group I and 48.5 to 75.8 in Group II (Table 4 and 5).


The independent t-test revealed a highly significant difference in EQ-5D-5L Index changes between Group I and Group II (P = 4.51 × 10−⁸). This extremely low P-value provides strong statistical evidence that the life quality improvements measured with the EQ-5D-5L Index differ significantly between the two groups. These findings suggest that the intervention had a substantial and statistically meaningful impact on Health-related life satisfaction.
SIJ blocks have been widely utilized in the managing SIJ-related pain, particularly in patients having spondyloarthropathies [10-12]. Their efficacy in providing symptomatic relief shows their potential as both a diagnostic and therapeutic intervention. However, the extent and duration of pain relief remain variable across different patient populations, necessitating further investigation into their long-term effectiveness and patient selection criteria. Slipman et al. [13] demonstrated that corticosteroid SIJ injections provided prolonged pain relief in patients diagnosed with SIJ dysfunction using a single diagnostic SIJ block. In contrast, Pulisetti and Ebraheim [14] stated that 90% of patients having non-inflammatory SIJ pain had only transient benefits, with symptom relief diminishing within 2 weeks. A key limitation of some similar studies [13,14] was the reliance on a single, uncontrolled SIJ block for patient selection, a method related to a false-positive occurrence of up to 20%. Vallejo et al. [15] addressed this issue by employing a dual-injection protocol with corticosteroids and local anesthetic, yielding a 57.7% rate of sustained pain relief (>50% pain reduction) lasting at least 12 weeks. While this approach likely improved diagnostic precision, the long-term outcomes remain uncertain [16]. In our study, fluoroscopic guidance was employed to enhance procedural accuracy and mitigate the risk of false-positive diagnoses associated with blind injections. Our findings indicate that Both the ODI and VAS scores showed statistically significant improvement in 25 patients at the final follow-up (P = 0.0001). Notably, pain relief persisted for at least 6 weeks in 12 patients, with an average duration of 36.8 ± 9.9 weeks. Among the cohort, three reported only transient relief, suggesting that corticosteroid SIJ blocks may not provide sustained benefits for all individuals. Our comparative analysis revealed important differences between conservative management (Group I) and SIJ block intervention (Group II). While both groups showed improvements across all aspects of health-related quality of life assessed by the EQ-5D-5L questionnaire, the SIJ block group demonstrated superior outcomes at 6 months. The EQ-5D-5L index value increased more substantially in Group II (0.42–0.79, an improvement of 0.37) than in Group I (0.41–0.67, an improvement of 0.26). Similarly, the EQ-VAS score showed greater improvement in Group II (48.5–75.8, a 27.3-point increase) compared to Group I (47.8–67.2, a 19.4-point increase). The most significant improvements were observed in pain/discomfort and mobility dimensions, which directly impact patients’ functional capabilities and quality of life. Although our study established the efficacy of SIJ blocks compared to conservative management, it is important to acknowledge that patient selection for SIJ blocks was based on initial non-responsiveness to conservative treatment. The factors contributing to treatment failure in certain individuals, while others, such as those in Group I, who responded favorably to conservative management, remain unclear. The variability in treatment response may be attributed to multiple factors, including patient demographics and underlying pathology. Advanced age , elevated body mass index, and prior lumbar or lumbosacral fusion [17-20] have been implicated in the progression of SIJ arthropathy and may contribute to diminished treatment efficacy. Additionally, anatomical variations such as a narrow joint space or osteophyte formation can complicate injection procedures, as observed in five patients who were excluded due to unsuccessful SIJ block attempts. Although this study provides valuable insights into the efficacy of corticosteroid SIJ blocks compared to conservative management in a select patient population, certain limitations warrant consideration. The lack of a control group, a relatively small sample size, and the absence of long-term follow-up data are to be addressed in future studies. Overall, our findings align with existing literature suggesting that corticosteroid SIJ blocks can offer meaningful pain relief in appropriately selected patients [21]. The superior progress in functional health and life quality in functional status and quality of life measures observed in the SIJ block group support its consideration as an effective intervention for patients who have had inadequate response to conservative management. However, given the heterogeneity in treatment response, future studies. It should emphasize enhancing the criteria for patient selection and exploring adjunctive strategies to optimize long-term outcomes.
This prospective study demonstrates that fluoroscopy-guided SIJ blocks offer superior clinical outcomes compared to conservative management in patients with sacroiliitis. While both treatment approaches resulted in significant improvements, the SIJ block group consistently showed greater enhancement across all measured parameters, including pain reduction, functional recovery, and health-related well-being. These findings support the application of SIJ blocks as an efficient intervention to the patients having inadequate outcome to conservative treatment. Future studies should focus on refining patient selection and assessing long-term consequences to optimize clinical practice.
Fluoroscopy-guided SIJ blocks outperform conservative management in sacroiliitis, providing greater pain relief, functional recovery, and well-being.
References
- 1.Daum WJ. The sacroiliac joint: An underappreciated pain generator. Am J Orthop (Belle Mead NJ) 1995;24:475-8. [Google Scholar | PubMed]
- 2.LeBlanc KE. Sacroiliac sprain: An overlooked cause of back pain. Am Fam Physician 1992;46:1459-63. [Google Scholar | PubMed]
- 3.Verrills P, Vivian D. Interventions in chronic low back pain. Aust Fam Physician 2004;33:421-6. [Google Scholar | PubMed]
- 4.Al-Subahi M, Alayat M, Alshehri MA, Helal O, Alhasan H, Alalawi A, et al. The effectiveness of physiotherapy interventions for sacroiliac joint dysfunction: A systematic review. J Phys Ther Sci 2017;29:1689-94. [Google Scholar | PubMed]
- 5.Rosenberg JM, Quint TJ, De Rosayro AM. Computerized tomographic localization of clinically-guided sacroiliac joint injections. Clin J Pain 2000;16:18-21. [Google Scholar | PubMed]
- 6.Gaillard F, Hng J, Kaya H. Sacroiliitis Grading (New York Criteria). Available from: https://radiopaedia.org [Last accessed on 2025 Jan 02]. [Google Scholar | PubMed]
- 7.Ogduk N. Practice Guidelines for Spinal Diagnostic and Treatment Procedures: Sacroiliac Joint Blocks. Kentfield, CA: International Spine Intervention Society; 2004. p. 66-85. [Google Scholar | PubMed]
- 8.Hudson-Cook N, Tomes-Nicholson K, Breen A. A revised Oswestry disability questionnaire. In: Roland MO, Jenner JR, editors. Back Pain: New Approaches to Rehabilitation and Education. New York, NY: Manchester University Press; 1989. p. 187-204 [Google Scholar | PubMed]
- 9.Garratt AM, Furunes H, Hellum C, Solberg T, Brox JI, Storheim K, et al. Evaluation of the EQ-5D-3L and 5L versions in low back pain patients. Health Qual Life Outcomes 2021;19:155. [Google Scholar | PubMed]
- 10.Fritz JM, Irrgang JJ. A comparison of a modified Oswestry low back pain disability questionnaire and the Quebec back pain disability scale. Phys Ther 2001;81:776-88. [Google Scholar | PubMed]
- 11.Maugars Y, Mathis C, Berthelot JM, Charlier C, Prost A. Assessment of the efficacy of sacroiliac corticosteroid injections in spondylarthropathies: A double-blind study. Br J Rheumatol 1996;35:767-70. [Google Scholar | PubMed]
- 12.Maugars Y, Mathis C, Vilon P, Prost A. Corticosteroid injection of the sacroiliac joint in patients with seronegative spondylarthropathy. Arthritis Rheum 1992;35:564-8. [Google Scholar | PubMed]
- 13.Slipman CW, Lipetz JS, Plastaras CT, Jackson HB, Vresilovic EJ, Lenrow DA, et al. Fluoroscopically guided therapeutic sacroiliac joint injections for sacroiliac joint syndrome. Am J Phys Med Rehabil 2001;80:425-32. [Google Scholar | PubMed]
- 14.Pulisetti D, Ebraheim NA. CT-guided sacroiliac joint injections. J Spinal Disord 1999;12:310-2. [Google Scholar | PubMed]
- 15.Vallejo R, Benyamin RM, Kramer J, Stanton G, Joseph NJ. Pulsed radiofrequency denervation for the treatment of sacroiliac joint syndrome. Pain Med 2006;7:429-34. [Google Scholar | PubMed]
- 16.Chakraverty R, Dias R. Audit of conservative management of chronic low back pain in a secondary care setting--part I: Facet joint and sacroiliac joint interventions. Acupunct Med 2004;22:207-13. [Google Scholar | PubMed]
- 17.Katz V, Schofferman J, Reynolds J. The sacroiliac joint: A potential cause of pain after lumbar fusion to the sacrum. J Spinal Disord Tech 2003;16:96-9. [Google Scholar | PubMed]
- 18.Maigne JY, Planchon CA. Sacroiliac joint pain after lumbar fusion. A study with anesthetic blocks. Eur Spine J 2005;14:654-8. [Google Scholar | PubMed]
- 19.Jee H, Lee JH, Park KD, Ahn J, Park Y. Ultrasound-guided versus fluoroscopy-guided sacroiliac joint intra-articular injections in the noninflammatory sacroiliac joint dysfunction: A prospective, randomized, single-blinded study. Arch Phys Med Rehabil 2014;95:330-7. [Google Scholar | PubMed]
- 20.Ha KY, Lee KS, Jim KW. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: A prospective cohort study over five-year follow-up. Spine (Phila Pa 1976) 2008;33:1192-8. [Google Scholar | PubMed]
- 21.Scholten PM, Patel SI, Christos PJ, Singh JR. Short-term efficacy of sacroiliac joint corticosteroid injection based on arthrographic contrast patterns. PM R 2015;7:385-91. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction
June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes October 1, 2025 Effectiveness of Epidural Methylprednisolone Injection in Management of Lumbar Prolapsed Intervertebral Disc: A Comparison of Caudal, Transforaminal and Interlaminar Routes
October 1, 2025 Effectiveness of Epidural Methylprednisolone Injection in Management of Lumbar Prolapsed Intervertebral Disc: A Comparison of Caudal, Transforaminal and Interlaminar Routes December 1, 2024 Role of Image-guided Platelet-rich Plasma Injection in the Management of Patients of Supraspinatus Tendon Tear
December 1, 2024 Role of Image-guided Platelet-rich Plasma Injection in the Management of Patients of Supraspinatus Tendon Tear