
The two-stage arthroscopic approach for MLKIs prioritizes PCL/PLC repair, minimizing stiffness, with early ROM and delayed weight-bearing aiding recovery and stability
Dr. M Aravindan, Department of Orthopedics, Sree Balaji Medical College Hospital, Chromepet, Chennai - 600044, Tamil Nadu, India. E-mail: santhosh.aravind.m@gmail.com
Abstract
Introduction: Multi-ligament knee injuries (MLKIs), involving damage to two or more major knee ligaments, present complex challenges in orthopedic surgery due to the intricacy of the injury and its significant impact on knee stability and function. These injuries often require specialized treatment strategies, with two-stage surgical reconstructions emerging as a viable option. This report examines a case of MLKI and the outcomes of a staged surgical approach to repair and reconstruct the affected knee ligaments.
Case Report: A 55-year-old female sustained a multi-ligament injury to her right knee after a twisting event, resulting in pain, swelling, and instability. The patient underwent a two-stage arthroscopic reconstruction, beginning with repair of the posterior cruciate ligament and posterolateral corner structures, followed by anterior cruciate ligament reconstruction. Autografts, including the bilateral peroneus longus and contralateral hamstrings, were used for the procedure. Her rehabilitation protocol emphasized early passive range of motion exercises, with delayed weight-bearing to promote effective healing.
Conclusion: This case demonstrates the successful restoration of knee stability and function following a two-stage surgical approach to MLKI. The case underscores the need for individualized treatment plans and highlights the potential benefits of a phased procedure. While promising, further research is required to compare single-stage and two-stage approaches and to assess their long-term outcomes in managing complex MLKIs.
Keywords: Instability, arthroscopic repair, ligament injury, reconstruction.
Knee injuries, which are frequently caused by trauma or unexpected twists, can be very difficult for patients and orthopedic surgeons to treat. Multi-ligament knee injury (MLKI) occurs when there is damage to two or more of the four major knee ligaments: The anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), the posteromedial corner including medial collateral ligament, and the posterolateral corner (PLC) including lateral collateral ligament (LCL) [1]. Despite their rarity, these kinds of multi-ligament injuries provide considerable difficulties for orthopedic surgeons. Multi-ligament rips are a particularly uncommon kind of knee injury because of their intricacy and tendency to affect joint stability, leading to significant function loss, discomfort, and long-term instability. The course of treatment for knee injuries involving several ligaments is always changing. Orthopedic surgeons must choose between simultaneous or phased treatments when reconstruction is considered necessary for all ligament groups. The concomitant approach is preferred because it minimizes the overall number and length of surgeries, and it offers early intervention and knee brace rehabilitation benefits. However, patients are exposed to extended periods of invasive surgery, which raises the risk of post-operative complications such as infection and stiffness in the knee joint [2-7]. Conversely, a phased approach improves clinical results following the repair of numerous ligament injuries without reducing knee range of motion (ROM) [2,3]. Research conducted by Bin and Nam [8] has documented favorable functional results for individuals treated with a two-stage surgical procedure. A two-stage technique has produced adequate stability and ROM according to Subbiah et al. [9]. On the other hand, Godin et al. [10] suggest single-stage surgery as a dependable and beneficial treatment. In a similar vein, single-stage reconstruction is regarded by Bagherifard et al. [1] and Billières et al. [11] as a practical and successful treatment approach for these patients. The introduction provides an overview of a method for the phased reconstruction of the ACL, PCL, and PLC. It clarifies the fundamental ideas, steps involved in creating a bone tunnel, inserting a graft, and completing the distal fixation. This article delves into a compelling case involving a 55-year-old female experiencing pain, swelling, and instability in her right knee after a twisting injury. The intricate journey of diagnosis and treatment underscores the nuanced approach necessary for effectively managing MLKIs. From the initial clinical presentation to detailed diagnostic imaging and the subsequent two-stage arthroscopic repair and reconstruction, this case provides valuable insights into the comprehensive care essential for restoring function and stability to a compromised knee joint.
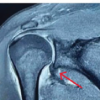
This is a case about a 55-year-old female who presented with complaints of pain and swelling in the right knee for 2 weeks, which was associated with giving away of the knee. The patient had an alleged history of twisting injury to the right knee 2 weeks back followed by complaints of pain and swelling in the right knee. The patient can able to walk after the fall with giving away followed by swelling in the right knee. The patient has a comorbidity of hypertension and diabetes on regular treatment. On local examination of the right knee, the patient had diffuse swelling with tenderness present over the medial joint line, posterolateral aspect, and suprapatellar region. Sag sign was positive. The range of movements was 0–40° in active flexion, and 10° of hyperextension was present. Special test like Lachman test was 2B grade (ACL injury with 5–10 mm translation without an endpoint), varus stress test was grade 3 (complete LCL tear with >10 mm opening of the lateral joint), and patella grind was positive which indicates ACL, PCL, and LCL associated with patellofemoral arthritis. There was no any other associated distal neurovascular deficit. Initially, X-ray of the right knee was taken which showed medial joint space reduction and no other bony abnormalities seen (Fig. 1a). Further investigation of MRI scan (Fig. 1b and c) was taken and found to be a complete tear of ACL, PCL, and LCL with lateral patellofemoral ligament. We planned for arthroscopic repair and reconstruction in a two-way procedure: Stage 1, arthroscopic repair and reconstruction of PCL and PLC and Stage 2, arthroscopic reconstruction of ACL. Surgeons often prefer to reconstruct the PCL first, as it provides a stable foundation for the knee, making it easier to accurately position and tension the ACL graft. This approach supports better biomechanics, balance, and stability for the knee overall. Hence, after routine pre-operative investigation, the patient was posted for surgery.

Graft option
Allografts are not easily available, are expensive, and have delayed incorporation with an increased risk of infection [12-14]. Autografts are available easily, and they incorporate early but have associated donor site morbidity and require judicial usage in MKLI reconstruction [12,15]. Autograft options for ligament reconstruction are limited. The patellar bone tendon-bone graft or quadriceps tendon graft has more chances of anterior knee pain or knee stiffness [14] whereas the contralateral hamstring graft yields good results in MLKI [16]. Moreover, peroneus longus can be used for cruciate ligament reconstruction without any donor site morbidity [17-19]. In this case, bilateral peroneus longus was used and contralateral hamstrings were harvested and found to be inadequate, so a quadriceps graft from the contralateral limb was harvested with no residual morbidity.
Surgical Technique
Stage 1: Arthroscopic repair and reconstruction of PCL and PLC
Under epidural anesthesia, the patient was once again examined for special test which was positive for anterior drawer test, Lachman maneuver, posterior drawer test, pivot shift test, and varus instability. Then, the patient in supine position with tourniquet application over the right proximal thigh, parts painted and draped for both lower libs. The knee is kept in 90° flexion with a foot and side support to maintain in position and prevent external rotation. Initially, peroneus longus graft was harvested from both legs, prepared, quadrupled, and kept ready (Fig. 2a). In the right knee, two portals were made anterolateral for viewing and anteromedial for working (Fig. 3). Empty notch sign was positive (Fig. 4). The meniscus seems was intact and there was complete PCL, ACL tear was noted with LCL and popliteal tear. The remnant of ACL and PCL was removed using a shaver (Fig. 5). For PCL reconstruction, a tibial tunnel of size 9.5 mm with a femoral tunnel of size 9.5 mm was made, and care was taken to prevent posterior blowout. Tunnel in tunnel sign was checked. The harvested peroneal graft was inserted into the tibial tunnel and fixed using a bioabsorbable interferential screw of size 10 × 3.5 mm and into the femoral tunnel and fixed using an adjustable loop endobutton of size 60 mm (Fig. 6). Implant position was checked under C-arm guidance and found to be satisfactory. For posterolateral instability, semitendinosus and gracilis tendons were harvested ipsilaterally and prepared (83.5 × 24 mm).




Then using the Larson procedure, around 10 cm incision was on the lateral aspect of the knee, centering Gerdy’s tubercle (Fig. 2b). Then, skin and subcutaneous tissue with subsequent layers were cut and retracted. There was biceps femoris complete tear, and popliteus muscle partial tear was noted. LCL was visualized, and complete tears were noted. Common peroneal nerve was identified, tagged, isolated, and retracted posteriorly.
Two tunnels were made in the lateral femoral condyle and one tunnel at the fibular head respective to the anatomical insertion of LCL (Fig. 7). Harvested graft was passed through the first tunnel which is created over the lateral femoral epicondyle and fixed with bioabsorbable interferential screw of size 7 × 25 mm (Fig. 8). The second tunnel was made in fibula head, and graft was looped in and fixed using 7.5 mm bioabsorbable interferential screw. At last, a third tunnel was created 1.5 cm below previous femoral tunnel, and graft was inserted and fixed using a 30 × 7 mm size bioabsorbable interferential screw. The stability and range of movements were assessed and found to be satisfactory. Thorough wound wash was given, and the wound closed in layer. Sterile dressing was done, and crepe bandage along with long knee brace was applied.


Stage 2: Arthroscopic reconstruction of ACL
After 2 weeks post-operative care and awaited for surgical wound healing, the patient was planned for second-stage procedure. A 2-week interval between PCL and ACL reconstructions may allow for a quicker overall recovery and reduced time spent in knee instability, which is useful for patients needing rapid functional stability. It also enables a streamlined rehabilitation process, as both surgeries can be addressed earlier and may lower the risk of muscle atrophy and joint stiffness by minimizing inactivity. However, these benefits come with higher risks, including inadequate healing and potential complications.
Under sterile aseptic precaution, under spinal anesthesia, under tourniquet control, the patient in supine position, with knee in 90o flexion, two portals were made over previous surgical scar, anteromedial for working and anterolateral for viewing. Previous PCL and PLC reconstructions were checked and found to be intact. Lateral gutter, medial gutter, and meniscus were found to be normal. Hamstring graft of contralateral limb was harvested and found to be inadequate. Hence, a quadriceps graft of 9 cm from the contralateral limb was harvested, prepared, and kept ready. A femoral tunnel was made, and care was taken to prevent posterior blowout. For tibial tunnel, a 55° tibial guide was taken and tunnel was created (Fig. 9a). Tunnel in tunnel sign was checked. Harvested quadriceps graft from the contralateral limb was inserted into the tibial side and fixed with a 9 × 30 mm bioabsorbable interferential screw and the femoral side with a 7 × 25 mm bioabsorbable interferential screw (Fig. 9b and c). The range of movements was checked and found to be satisfactory. A thorough wound wash was given, and the wound closed in layers. Sterile dressing was done, and crepe bandage long knee brace was applied.

Rehabilitation protocol
Physiotherapy started from day 1 with quadriceps muscle building and early progressive passive ROM exercises. For patients with reconstructed PCL, active knee flexion was delayed for 6 weeks. Non-weight-bearing was advised from first post-operative day keeping the knee brace locked in extension which progressed to partial weight-bearing walk after 6 weeks followed by full weight-bearing walking. Once a patient developed adequate neuromuscular control without any pain, a return to normal day-to-day life activities was allowed. Precautious movements such as sitting crossed legs, climbing stairs, and squatting were started after 12 months (1). The patient was followed up for 1½ years and was finally assessed using the Lysholm Knee Scoring Scale, which resulted in a score of 84. This score is considered good for our patient, indicating a favorable outcome in terms of knee function and recovery.
High-energy processes can lead to multiple ligament injuries, with motor vehicle and motorbike accidents accounting for the majority of documented instances [20-23]. Older adults are less likely to be injured, and if they are, the course of therapy will usually be conservative because of the poor condition of their bones, the length of time it takes for them to heal, and their daily activities. A main solution was deemed necessary for the 55-year-old obese patient in our case, who was physically active prior to the injury, had no past knee ligament injuries, and had a knee flexion of more than 90° associated with high bone quality based on the results of the radiographic investigation and bone density scan. Due to the fact that posterior tibial sagging inhibits the recovery of the restored ligaments, we thus planned for two stages of reconstruction: First, the PCL and collateral, and then, the ACL. The basis of the surgery’s duration, hemodynamic stability during the process, and tourniquet time are further indications for selecting the two-stage technique. According to Mook et al. [24], patients who underwent single-stage surgery following knee dislocations were more likely to experience joint stiffness as opposed to those who underwent staged surgery. On the other hand, Levy et al. [25] did not discover any variation in ROM between individuals treated with single surgery and those treated with phased surgery. However, single-stage surgery exposes patients to long hours of invasive surgery which increases the chance of post-operative complications such as knee joint stiffness, infection, and recurrent knee joint instability [2,6,7]. Single-stage surgery has been favored for reducing the overall number and period of surgery as well as its benefits of early intervention and rehabilitation [2-5]. In this case we came across a blister at the wound site was one the complication for the patient that eventually turned into an ulcer wound (Fig. 10). However, the patient desires conservative care; the ulcer healed with periodic dressings. On the other hand, a phased approach not only results in better clinical outcomes following the repair of multiple ligament injuries, but it also avoids any knee surgery that could reduce knee ROM [2,3]. In the adult population, there is a high frequency of meniscal and chondral lesions linked to MLKIs [25]. To enhance the prognosis for these individuals, a thorough diagnosis and treatment strategy are essential. Insufficient PLC has been linked to higher stresses on the ACL and PCL according to biomechanical investigations [26,27]. By reestablishing varus stability, the LCL plays a crucial role in relieving the strain on the cruciate ligaments [26,27]. These results imply that non-physiologic stresses and eventual failure may result from neglecting to treat all ligamentous anomalies. Hence, every ligament should be repaired, but decision of making single- or two-stage procedure is hypothetical.

Two-stage multi-ligament knee reconstruction is a dependable technique that, after a 2-year follow-up, improved patient-reported outcomes and knee function without experiencing any problems. Our aim of having the patient be able to walk steadily was accomplished. Single- and two-stage operations are used to treat these injuries; however, there is disagreement about the optimal ways to treat them. To ascertain the long-term advantages of multiple ligament reconstructive surgery in this patient population, a longer follow-up in a larger series of patients is necessary.
A two-stage arthroscopic approach for MLKIs offers a reliable method for restoring joint stability and function. By addressing the PCL and PLC first, followed by ACL reconstruction, this approach minimizes complications such as joint stiffness. Early passive motion and delayed weight-bearing are crucial for optimal recovery, making this strategy a promising option for complex MLKI.
References
- 1.Bagherifard A, Jabalameli M, Ghaffari S, Rezazadeh J, Abedi M, Mirkazemi M, et al. Short to mid-term outcomes of single-stage reconstruction of multiligament knee injury. Arch Bone Jt Surg 2019;7:346-53. [Google Scholar | PubMed]
- 2.Liow RY, McNicholas MJ, Keating JF, Nutton RW. Ligament repair and reconstruction in traumatic dislocation of the knee. J Bone Joint Surg Br 2003;85:845-51. [Google Scholar | PubMed]
- 3.Wascher DC, Becker JR, Dexter JG, Blevins FT. Reconstruction of the anterior and posterior cruciate ligaments after knee dislocation. Results using fresh-frozen nonirradiated allografts. Am J Sports Med 1999;27:189-96. [Google Scholar | PubMed]
- 4.Fanelli GC, Giannotti BF, Edson CJ. Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction. Arthroscopy 1996;12:5-14. [Google Scholar | PubMed]
- 5.Fanelli GC, Orcutt DR, Edson CJ. The multiple-ligament injured knee: Evaluation, treatment, and results. Arthroscopy 2005;21:471-86. [Google Scholar | PubMed]
- 6.Almekinders LC, Logan TC. Results following treatment of traumatic dislocations of the knee joint. Clin Orthop Relat Res 1992;284:203-7. [Google Scholar | PubMed]
- 7.Hegyes MS, Richardson MW, Miller MD. Knee dislocation. Complications of nonoperative and operative management. Clin Sports Med 2000;19:519-43. [Google Scholar | PubMed]
- 8.Bin SI, Nam TS. Surgical outcome of 2-stage management of multiple knee ligament injuries after knee dislocation. Arthroscopy 2007;23:1066-72. [Google Scholar | PubMed]
- 9.Subbiah M, Pandey V, Rao SK, Rao S. Staged arthroscopic reconstructive surgery for multiple ligament injuries of the knee. J Orthop Surg (Hong Kong) 2011;19:297-302. [Google Scholar | PubMed]
- 10.Godin JA, Cinque ME, Pogorzelski J, Moatshe G, Chahla J, LaPrade RF. Multiligament knee injuries in older adolescents: A 2-year minimum follow-up study. Orthop J Sports Med 2017;5:2325967117727717. [Google Scholar | PubMed]
- 11.Billières J, Labruyère C, Steltzlen C, Gonzalez A, Boisrenoult P, Beaufils P, et al. Multiligament knee injuries treated by one-stage reconstruction using allograft: Postoperative laxity assessment using stress radiography and clinical outcomes. Orthop Traumatol Surg Res 2020;106:937-44. [Google Scholar | PubMed]
- 12.Carey JL, Dunn WR, Dahm DL, Zeger SL, Spindler KP. A systematic review of anterior cruciate ligament reconstruction with autograft compared with allograft. J Bone Joint Surg Am 2009;91:2242-50. [Google Scholar | PubMed]
- 13.Romanini E, D’Angelo F, De Masi S, Adriani E, Magaletti M, Lacorte E, et al. Graft selection in arthroscopic anterior cruciate ligament reconstruction. J Orthop Traumatol 2010;11:211-9. [Google Scholar | PubMed]
- 14.Weiss NG, Kaplan LD, Graf BK. Graft selection in surgical reconstruction of the multiple-ligament-injured knee. Oper Tech Sports Med 2003;11:218-25. [Google Scholar | PubMed]
- 15.Goyal T, Paul S, Das L, Choudhury AK. Correlation between anthropometric measurements and activity level on length and diameter of semitendinosus tendon autograft in knee ligament surgery: A prospective observational study. SICOT J 2020;6:23. Khan MJ, Asif N, Sharma A, Siddiqui YS, Khan AQ. Single-stage versus two-stage reconstruction in chronic multi ligament knee injury. Int J Burns Trauma 2022;12:35-44. [Google Scholar | PubMed]
- 16.McCarthy M, Ridley TJ, Bollier M, Cook S, Wolf B, Amendola A. Posterolateral knee reconstruction versus repair. Iowa Orthop J 2015;35:20-5. [Google Scholar | PubMed]
- 17.Setyawan R, Soekarno NR, Asikin AI, Rhatomy S. Posterior cruciate ligament reconstruction with peroneus longus tendon graft: 2-years follow-up. Ann Med Surg (Lond) 2019;43:38-43. [Google Scholar | PubMed]
- 18.Rhatomy S, Wicaksono FH, Soekarno NR, Setyawan R, Primasara S, Budhiparama NC. Eversion and first ray plantarflexion muscle strength in anterior cruciate ligament reconstruction using a peroneus longus tendon graft. Orthop J Sports Med 2019;7:2325967119872462. [Google Scholar | PubMed]
- 19.Rhatomy S, Asikin AI, Wardani AE, Rukmoyo T, Lumban-Gaol I, Budhiparama NC. Peroneus longus autograft can be recommended as a superior graft to hamstring tendon in single-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2019;27:3552-9. [Google Scholar | PubMed]
- 20.Voos JE, Heyworth BE, Piasecki DP, Henn RF, MacGillivray JD. Traumatic bilateral knee dislocations, unilateral hip dislocation, and contralateral humeral amputation: A case report. HSS J 2009;5:40-4. [Google Scholar | PubMed]
- 21.Foad A, LaPrade RF. Bilateral luxatio erecta humeri and bilateral knee dislocations in the same patient. Am J Orthop Belle Mead 2007;36:611-3. [Google Scholar | PubMed]
- 22.Colen S, Van Den Bekerom MP, Truijen J. High-energy bilateral knee dislocations in a young man: A case report. J Orthop Surg (Hong Kong) 2013;21:396-400. [Google Scholar | PubMed]
- 23.Burrus MT, Werner BC, Cancienne JM, Miller MD. Simultaneous bilateral multiligamentous knee injuries are associated with more severe multisystem trauma compared to unilateral injuries. Knee Surg Sports Traumatol Arthrosc 2015;23:3038-43. [Google Scholar | PubMed]
- 24.Mook WR, Miller MD, Diduch DR, Hertel J, Boachie-Adjei Y, Hart JM. Multiple-ligament knee injuries: A systematic review of the timing of operative intervention and postoperative rehabilitation. J Bone Joint Surg Am 2009;91:2946-57. [Google Scholar | PubMed]
- 25.Levy BA, Dajani KA, Whelan DB, Stannard JP, Fanelli GC, Stuart MJ, et al. Decision making in the multiligament-injured knee: An evidence-based systematic review. Arthroscopy 2009;25:430-8. [Google Scholar | PubMed]
- 26.LaPrade RF, Muench C, Wentorf F, Lewis JL. The effect of injury to the posterolateral structures of the knee on force in a posterior cruciate ligament graft: A biomechanical study. Am J Sports Med 2002;30:233-8. [Google Scholar | PubMed]
- 27.LaPrade RF, Resig S, Wentorf F, Lewis JL. The effects of grade III posterolateral knee complex injuries on anterior cruciate ligament graft force. A biomechanical analysis. Am J Sports Med 1999;27:469-75. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations
July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations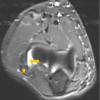 July 1, 2026 Dual Ligament Reconstruction in a Neglected Medio-Lateral Instability of the Elbow: A Case Report and Surgical Technique
July 1, 2026 Dual Ligament Reconstruction in a Neglected Medio-Lateral Instability of the Elbow: A Case Report and Surgical Technique July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study
July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction
June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction