
Severe mangled foot injuries with extensive midfoot bone and soft-tissue loss are not absolute indications for amputation. Preservation of even a single major vascular supply, combined with early aggressive debridement, staged skeletal stabilisation, timely soft-tissue coverage, and coordinated ortho-plastic management, can achieve successful limb salvage with a satisfactory functional recovery.
Dr. Purushotham Lingaiah, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: puru@aiimsmangalagiri.edu.in
Abstract
Introduction: Management of a mangled foot remains one of the most challenging situations in orthopaedic trauma. The decision between amputation and limb salvage is controversial, particularly in patients with severe bone and soft-tissue loss. Functional outcomes, patient expectations, vascularity, and available reconstructive expertise play important roles in decision-making. We report a successful case of limb salvage in a young female with a severely mangled foot managed using staged orthopaedic and plastic surgical reconstruction.
Case Report: A 26-year-old female sustained a crush injury to her right foot following a road traffic accident. Clinical examination revealed severe soft-tissue damage with extensive loss of tarsal bones and metatarsals, resulting in an unstable flail foot. The posterior tibial artery was intact and maintained distal vascularity, whereas the tibial nerve could not be identified. Emergency debridement and stabilisation were performed using Kirschner wires and an external fixator. Serial wound debridement was undertaken, and a plastic surgery consultation was obtained early for soft-tissue management. Once a healthy wound bed was achieved, definitive skeletal reconstruction and soft-tissue coverage were performed simultaneously. Progressive rehabilitation was initiated postoperatively, and full weight-bearing ambulation was achieved 16 months after the final procedure. At the latest follow-up, the patient was independently ambulatory with mild residual pain and high satisfaction regarding limb preservation.
Conclusion: Successful limb salvage is possible even in severely mangled feet with extensive bone loss when vascularity is preserved, and multidisciplinary management is instituted early. Appropriate skeletal stabilisation, repeated debridement, soft-tissue coverage, and prolonged rehabilitation are critical for achieving acceptable functional outcomes.
Keywords: Mangled foot, limb salvage, crush injury, reconstruction, soft-tissue coverage.
Mangled extremity injuries represent some of the most severe forms of musculoskeletal trauma encountered in orthopaedic practice. A mangled extremity is classically defined as a limb with a combined injury involving at least three of the following components: bone, soft tissue, vascular structures, and nerves, resulting in severe functional compromise and threat to limb viability [1]. Mangled foot injuries constitute a particularly challenging subset because of the foot’s complex anatomy, unique biomechanical role in weight transmission, and limited soft-tissue envelope. The severity of damage often creates a difficult dilemma between primary amputation and attempts at limb salvage [2]. These injuries usually result from high-energy trauma mechanisms, including road traffic accidents, industrial accidents, crush injuries, machinery-related trauma, blast injuries, and agricultural injuries. Such mechanisms produce varying combinations of open fractures, bone loss, degloving injuries, tendon disruption, vascular compromise, and neurological injury [3]. The foot is particularly vulnerable due to its multiple small articulations and dependence on preservation of skeletal architecture for maintaining normal gait mechanics. Extensive destruction of the midfoot and hindfoot often results in instability and a non-functional flail foot [4]. Decision-making in mangled extremity injuries remains one of the most controversial areas in trauma surgery [5]. Historically, various scoring systems have been developed to assist surgeons in predicting salvage potential and guiding treatment decisions. Among these, the mangled extremity severity score remains the most commonly used and incorporates parameters such as skeletal and soft-tissue injury, limb ischaemia, shock, and patient age. Other scoring systems include the limb salvage index, predictive salvage index, nerve injury, ischaemia, soft-tissue injury, skeletal injury, shock and age score, and Hannover fracture scale. While these scoring systems provide objective assessment frameworks, their predictive value in severe foot injuries remains inconsistent. Several studies have demonstrated limited sensitivity and specificity of these scores in accurately determining the need for amputation, particularly in patients with isolated foot trauma. Consequently, treatment decisions frequently rely more heavily on clinical judgement rather than numerical scoring systems alone [6,7,8]. Advances in orthopaedic fixation techniques, microsurgical soft-tissue reconstruction, and multidisciplinary trauma care have expanded the indications for limb salvage. Nevertheless, salvage procedures are associated with multiple surgeries, prolonged rehabilitation, and uncertain functional outcomes [9]. In this report, we present a case of successful limb salvage in a young female with a devastating crush injury and severe midfoot bone loss managed through staged orthoplastic reconstruction, highlighting important principles that influence decision-making and outcomes in mangled foot injuries.
A 26-year-old female presented to the emergency department following a road traffic accident involving a heavy vehicle running over her right foot. She sustained a severe crush injury to the foot with gross contamination and extensive soft-tissue damage. On examination, the patient was haemodynamically stable. Local examination revealed extensive degloving injury over the dorsum and plantar aspect of the foot with exposed tendons and bones. Multiple tarsal bones and metatarsals were severely comminuted or absent due to extrusion at the injury site. The foot appeared frail and unstable. Distal vascularity was maintained through the posterior tibial artery with preserved capillary refill. The dorsalis pedis artery was not palpable. Sensory examination was difficult because of pain and tissue destruction, and the tibial nerve could not be identified intraoperatively. Plain radiographs demonstrated severe destruction of the midfoot architecture with loss of multiple tarsal bones and metatarsals. The patient and family were counselled regarding the severity of injury, the possibility of multiple procedures, the uncertain functional outcome, and the option of primary amputation. Considering the preserved vascularity, young age of the patient, and strong patient preference for limb preservation, limb salvage was planned. Emergency surgery was performed on the day of injury. Extensive irrigation and meticulous debridement of contaminated and non-viable tissues were carried out. Skeletal stabilisation was achieved using Kirschner wires across the residual foot architecture, along with spanning external fixation to maintain alignment and length. Broad-spectrum intravenous antibiotics were administered, and serial wound inspections were planned (Figs. 1 and 2).

Figure 1: Mangled foot with extensive dorsum soft tissue and bone loss.
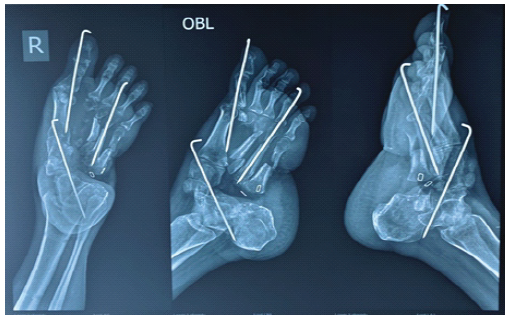
Figure 2: Radiograph showing the extensive tarsal, metatarsal bone loss and discontinuity between hind foot and mid-foot fixed with K-wires.
The patient subsequently underwent repeated debridement procedures to obtain a healthy wound bed (Fig. 3).
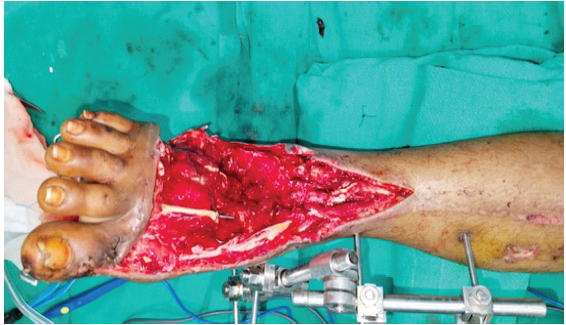
Figure 3: Serial debridement led to a healthy bed with bleeding margins.
Early involvement of plastic surgeons facilitated planning for definitive soft-tissue coverage. After adequate control of contamination and satisfactory granulation tissue formation, definitive reconstruction was undertaken. Simultaneous skeletal reconstruction and soft-tissue coverage were performed using staged reconstructive principles (Figs. 4 and 5).

Figure 4: Peroneal artery-based transposition flap to cover the defect and Skin grafting to the donor area.
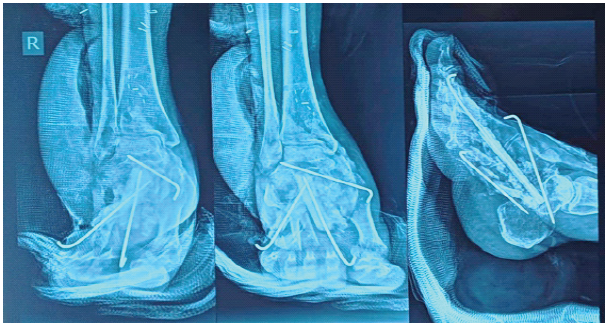
Figure 5: Post-operative radiographs showing fibula strut graft used to reconstruct the pillars of the foot.

Figure 6: Weight-bearing clinical picture after 3 years of the last surgery.
The foot was reconstructed using the fibula strut graft for the lost 2nd and 5th metatarsals. Peroneal artery-based flap coverage was done. Stable alignment of the residual foot was restored to provide a foot suitable for ambulation. Postoperatively, the limb was protected in a plaster-of-Paris slab, and gradual rehabilitation was initiated. Regular wound monitoring and physiotherapy were continued. Progressive weight-bearing was delayed until satisfactory soft-tissue healing and radiological evidence of stability were achieved. Sixteen months following the final reconstructive procedure, the patient began full weight-bearing ambulation using modified footwear (Fig. 6). At the latest follow-up, she was able to walk independently without support. Mild pain during prolonged walking persisted, but the patient reported high satisfaction with the salvaged limb and had resumed most activities of daily living. The salvaged foot was stable and cosmetically acceptable.
Management of mangled foot injuries continues to remain controversial [1]. While primary amputation may provide earlier rehabilitation and avoid repeated procedures, limb salvage offers psychological and functional advantages in selected patients. Multiple factors complicate the decision-making process. Vascular status remains one of the strongest determinants of limb salvage potential, and preservation of even a single major arterial supply may permit successful reconstruction. Neurological injury, particularly loss of plantar sensation, was traditionally considered an indication for amputation; however, contemporary evidence suggests that sensory deficits alone should not necessarily preclude salvage attempts [2]. Other important considerations include patient age, occupation, comorbidities, psychosocial factors, expected functional demands, rehabilitation potential, available surgical expertise, and patient preference. Furthermore, limb salvage often requires multiple operations, a prolonged hospital stay, repeated debridement procedures, and extensive rehabilitation with uncertain functional outcomes [9]. The final decision should be individualised after considering patient factors, injury characteristics, and available reconstructive expertise. One of the major determinants favouring salvage in the present case was preserved vascularity through the posterior tibial artery. Previous studies have shown that the presence of at least one intact major artery can permit successful limb salvage. Although neurological injury is traditionally considered a poor prognostic factor, loss of plantar sensation alone should not be regarded as an absolute indication for amputation. Current management strategies for mangled foot injuries emphasise a staged multidisciplinary approach [10]. Initial treatment focuses on Advanced Trauma Life Support principles, followed by urgent irrigation, aggressive debridement, infection control, and temporary skeletal stabilisation using external fixation or Kirschner wire fixation. Early ortho-plastic collaboration has become increasingly important in optimising outcomes. Definitive treatment may involve vascular repair, skeletal reconstruction, bone grafting, arthrodesis procedures, and soft-tissue coverage using local or free flaps. The principle of “fix and flap”, involving simultaneous skeletal stabilisation and soft-tissue reconstruction, has shown improved outcomes in selected patients [11]. Another important principle highlighted in this case is staged reconstruction. Initial aggressive debridement and temporary stabilisation helped prevent further soft-tissue damage while maintaining foot alignment. External fixation remains particularly useful in such injuries because it permits wound access and minimises additional soft-tissue insult. Despite successful salvage, functional limitations may persist. Salvaged limbs often require prolonged rehabilitation and may be associated with chronic pain, stiffness, altered gait mechanics, and multiple secondary procedures [12]. However, many patients prefer preservation of the native limb even when functional outcomes are imperfect. The present case demonstrates that even severe foot injuries with extensive midfoot bone loss can be salvaged successfully when vascularity is maintained, the patient’s perspectives are valued, and multidisciplinary expertise is available.
Limb salvage in severely mangled feet with extensive skeletal and soft-tissue loss is challenging but achievable in carefully selected patients. Preservation of vascularity, early aggressive debridement, stable skeletal fixation, timely soft-tissue coverage, and coordinated Ortho-Plastic management are essential for successful outcomes. A multidisciplinary approach and shared decision-making with the patient remain the cornerstones of treatment.
- Understand the patient and the injury
- Understand the variables involved in the decision for salvage vs amputation
- Analyze current evidence associated with limb salvage and amputation
- Discuss patient-derived outcomes
- Identify factors that influence decision-making, including economic, social, and cultural differences.
References
- 1. Higgins TF, Klatt JB, Beals TC. Lower Extremity Assessment Project (LEAP)–the best available evidence on limb-threatening lower extremity trauma. Orthop Clin North Am 2010;41:233-9. [Google Scholar] [PubMed]
- 2. Mackenzie EJ, Bosse MJ. Factors influencing outcome following limb-threatening lower limb trauma: Lessons learned from the Lower extremity assessment project (LEAP). J Am Acad Orthop Surg 2006;14:S205-10. [Google Scholar] [PubMed]
- 3. Kaul R, Iqbal MS, Akhoon N. Limb salvage in a mangled foot using combined external and internal fixation. J Limb Lengthening Reconstruction 2023;9:92-7. [Google Scholar] [PubMed]
- 4. Oda T, Oe K, Sakurai A, Fukui T, Niikura T, Kuroda R. Limb salvage for a mangled foot: A case report. J Orthop Case Rep 2020;9:58-61. [Google Scholar] [PubMed]
- 5. Ly TV, Travison TG, Castillo RC, Bosse MJ, MacKenzie EJ, LEAP Study Group. Ability of lower-extremity injury severity scores to predict functional outcome after limb salvage. J Bone Joint Surg Am 2008;90:1738-43. [Google Scholar] [PubMed]
- 6. Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. A prospective evaluation of the clinical utility of the lower-extremity injury-severity scores. J Bone Joint Surg Am 2001;83:3-14. [Google Scholar] [PubMed]
- 7. Fodor L, Sobec R, Sita-Alb L, Fodor M, Ciuce C. Mangled lower extremity: Can we trust the amputation scores? Int J Burns Trauma 2012;2:51-8. [Google Scholar] [PubMed]
- 8. Bosse MJ, McCarthy ML, Jones AL, Webb LX, Sims SH, Sanders RW, et al. The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-8. [Google Scholar] [PubMed]
- 9. Mackenzie EJ, Bosse MJ, Castillo RC, Smith DG, Webb LX, Kellam JF, et al. Functional outcomes following trauma-related lower-extremity amputation. J Bone Joint Surg Am 2004;86:1636-45. [Google Scholar] [PubMed]
- 10. Heitmann C, Levin LS. The orthoplastic approach for management of the severely traumatized foot and ankle. J Trauma 2003;54:379-90. [Google Scholar] [PubMed]
- 11. Zeiderman MR, Pu LL. Contemporary approach to soft-tissue reconstruction of the lower extremity after trauma. Burns Trauma 2021;9:tkab024. [Google Scholar] [PubMed]
- 12. Castillo RC, MacKenzie EJ, Wegener ST, Bosse MJ, LEAP Study Group. Prevalence of chronic pain seven years following limb threatening lower extremity trauma. Pain 2006;124:321-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report
February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report
August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization
August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series