
• To access the functional outcome following hydrodilation in adhesive capsulitis of shoulder • To compare the pre-procedure range of movements and the post-procedure range of movements
Dr. Arun Kumar K V, 1Department of Orthopaedics, Chettinad Hospital And Research Institute, Chettinad Academy of Research and Education, Kelambakkam-603103, Tamil Nadu, India. E-mail: arun5684@gmail.com
Abstract
Introdcution: Adhesive capsulitis, or frozen shoulder, is a painful and disabling condition characterized by progressive restriction of shoulder movement. Hydrodilatation, a minimally invasive procedure involving joint capsule distension, has been proposed as an effective treatment option. This study evaluates the functional outcomes of hydrodilatation in patients with adhesive capsulitis using the Constant-Murley score (CMS) and American Shoulder and Elbow Surgeons (ASES) score, along with pre- and post-procedure range of motion (ROM) assessments.
Materials and Methods: A prospective observational study was conducted on 30 patients diagnosed with adhesive capsulitis who underwent hydrodilatation. Functional and ROM improvements were assessed at baseline, post-procedure, 1 month, 3 months, 6 months, and 1 year. Data were analyzed using paired t-tests, and P < 0.05 was considered statistically significant.
Results: The mean age of participants was 47.7 ± 9.8 years. The study population comprised 14 males (46.7%) and 16 females (53.3%), indicating a slightly higher prevalence among females. Significant improvements were observed in active and passive abduction, adduction, forward flexion, and external rotation (P < 0.001). Internal rotation restriction reduced from 59.1% to 40.9% (P < 0.001). Functional scores (ASES and CMS) showed progressive improvement, with ASES increasing from 41.1 ± 6.1 to 65.9 ± 8.4 and CMS from 44.4 ± 5.8 to 64.8 ± 9.1 at 1 year (P < 0.001).
Conclusion: Hydrodilatation is an effective and well-tolerated intervention for improving shoulder function in adhesive capsulitis, with sustained benefits up to 1 year. Future studies should focus on standardizing treatment protocols and optimizing patient selection criteria.
Keywords: Adhesive capsulitis, frozen shoulder, hydrodilatation, range of motion.
Adhesive capsulitis, commonly known as “frozen shoulder,” is a prevalent condition characterized by shoulder pain and restricted range of motion (ROM), especially in external rotation. While often idiopathic, its occurrence is notably higher in individuals with diabetes mellitus and hypothyroidism. Historically, it was believed that adhesive capsulitis progresses through phases – freezing, frozen, and thawing – resolving spontaneously over 1–2 years. However, recent evidence suggests that without treatment, patients may experience enduring functional limitations [1]. Hydrodilatation has emerged as a therapeutic intervention for this condition. This procedure entails the injection of a solution, typically comprising normal saline, local anesthetics, and corticosteroids, into the glenohumeral joint under imaging guidance. The goal is to distend the joint capsule, thereby disrupting adhesions and delivering anti-inflammatory agents directly to the affected area. Clinical studies have demonstrated that hydrodilatation can lead to significant improvements in pain relief and shoulder mobility. For instance, a randomized clinical trial reported that patients receiving hydrodilatation experienced greater enhancements in ROM and functional scores at 1 and 3 months post-treatment compared to other injection methods [2]. Investigating the functional outcomes of hydrodilatation in adhesive capsulitis is essential to identify effective treatments that expedite recovery and restore shoulder function. Given the potential for prolonged disability if left untreated, evaluating interventions that offer rapid and sustained benefits is imperative. Hydrodilatation combines mechanical stretching of the capsule with targeted anti-inflammatory therapy, addressing the disorder’s structural and inflammatory aspects. Assessing its efficacy will provide valuable insights into its role in managing adhesive .
- To evaluate the functional outcomes of hydrodilatation in patients with shoulder adhesive capsulitis using the Constant-Murley score (CMS) and ASES score.
- To compare the ROM before and after the procedure.
Study design and setting
This study was a prospective observational study conducted at Chettinad Hospital and Research Institute from December 2021 to December 2023. Ethical approval was obtained from the Institutional Ethics Committee, and written informed consent was obtained from all participants before the study.
Study population
A total of 30 who came to the out-patient department and diagnosed with adhesive capsulitis of the shoulder were included in the study. Patients were selected based on predefined inclusion and exclusion criteria.
Inclusion criteria
- Patients aged between 30 and 70 years
- Clinically diagnosed cases of adhesive capsulitis with restricted active and passive ROM for at least 3 months
- Patients who failed to respond to conservative treatment, including physiotherapy and oral analgesics, for at least 6 weeks
- Willingness to participate in the study with signed informed consent.
Exclusion criteria
- Patients with a history of prior shoulder surgery or fracture
- Presence of rotator cuff tear confirmed by ultrasound or magnetic resonance imaging
- Patients with inflammatory arthritis (e.g., rheumatoid arthritis)
- Patients with systemic infections or local skin infections at the injection site
- Patients on anticoagulant therapy with a high risk of bleeding.
Procedure: Hydrodilatation under short general anesthesia
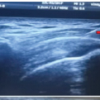
Hydrodilatation was performed under fluoroscopic guidance by an experienced orthopedician. The patient was kept in supine with the affected shoulder exposed.
Preparation and anesthesia
The skin over the shoulder joint was painted and draped. General anesthesia was administered. Local anesthesia (1–2 mL of 2% lignocaine) was infiltrated at the injection site.
Injection composition and administration
50 mL of normal saline, 5 mL of 1% lignocaine, and 40 mg of methylprednisolone were prepared. A 22 G or 23 G needle was inserted into the glenohumeral joint under fluoroscopic guidance. The prepared solution was injected gradually until capsular distension was achieved. Intraoperative range of movements achieved.
Post-procedure care
Patients were advised to rest for 24 h and then begin a structured physiotherapy program. Ice application and oral analgesics (if needed) were prescribed for pain management.
Physiotherapy regimen
Shoulder pendulum exercise and supine external rotation stretches for 7–10 days. One exercise is added every 5 days in the following order: Wall climbing or supine passive forward flexion, internal rotation, supine external rotation with abduction, and horizontal adduction stretches, followed by standing external rotation, external rotation in the corner, and internal rotation in abduction stretches.
Outcome measures
- Primary outcome
- Functional improvement was assessed using the CMS and the American Shoulder and Elbow Surgeons (ASES) score.
- These scores were recorded before the procedure, immediate post-procedure, and follow-ups (1 month, 3 months, 6 months, and 1 year post-procedure).
- Secondary outcome
- ROM of the shoulder was measured using a goniometer before the procedure, immediate post-procedure, and at follow-ups (1 month, 3 months, 6 months and 1 year).
- Parameters assessed:
- Forward flexion
- Abduction
- External rotation
- Internal rotation.
Statistical analysis
Data were analyzed using the Statistical Packages for the Social Sciences software version 26. Continuous variables (e.g., CMS, ASES scores, and ROM measurements) were expressed as mean ± standard deviation. A paired t-test was used to compare pre-procedure and post-procedure scores. P < 0.05 was considered statistically significant.
A total of 30 patients diagnosed with adhesive capsulitis of the shoulder were included in the study. The mean age of participants was 47.7 ± 9.8 years. The study population comprised 14 males (46.7%) and 16 females (53.3%), indicating a slightly higher prevalence among females. Regarding occupation, the majority of participants were homemakers (43.3%), followed by farmers (10.0%) and retired individuals (10.0%). The affected shoulder was right-sided in 18 patients (60.0%) and left-sided in 12 patients (40.0%). Among comorbidities, 23.3% of patients had hypertension, 23.3% had type 2 diabetes mellitus, and 16.7% had both hypertension and diabetes, while 36.7% had no comorbid conditions (Table 1).

Functional and ROM outcomes
Significant improvements were observed in active and passive ROM following hydrodilatation. Abduction: Active: Improved from 84.7° ± 13.6 pre-procedure to 121.3° ± 20.3 post-procedure (P < 0.001). Passive: Increased from 94.7° ± 13.6 to 137.3° ± 20.5 (P < 0.001). Adduction: Active: Increased from 17.3° ± 4.5 to 22.3° ± 4.3 (P < 0.001). Passive: Improved from 18.0° ± 4.8 to 22.3° ± 4.3 (P < 0.001). Forward flexion: Active: Increased from 95.7° ± 12.2 to 126.7° ± 15.4 (P < 0.001). Passive: Improved from 106.7° ± 11.8 to 142.7° ± 14.4 (P < 0.001). External rotation: Active: Increased significantly from 12.0° ± 4.1 to 24.3° ± 6.8 (P < 0.001). Passive: Improved from 12.0° ± 4.1 to 26.3° ± 6.7 (P < 0.001). Internal rotation: Pre-procedure: 59.1% of patients had restricted internal rotation. Post-procedure: This decreased to 40.9%, indicating a significant improvement (P < 0.001). No significant change was noted in extension movement, with active extension remaining at 23.0° ± 7.0 pre-procedure and 23.0° ± 4.7 post-procedure (P = 0.999) (Table 2 and Fig. 1) (Clinical Image 1).



Functional scores (ASES and CMS)
Both the ASES score and CMS demonstrated significant functional improvements following hydrodilatation.
ASES score
Increased from 41.1 ± 6.1 pre-injection to 60.9 ± 9.1 post-injection (P < 0.001). Continued to improve progressively over follow-ups, reaching 65.9 ± 8.4 at 1 year. Mean change from pre-injection to 1 year: +24.81 (95% confidence interval [CI]: 22.82, 26.8) (P < 0.001) (Fig. 2).
CMS
Improved from 44.4 ± 5.8 pre-injection to 60.7 ± 9.2 post-injection (P < 0.001). Increased steadily, reaching 64.8 ± 9.1 at 1 year. Mean change from pre-injection to 1 year: +20.46 (95% CI: 18.51, 22.41) (P < 0.001) (Fig. 2).
Active internal rotation: The number of patients with restricted movement decreased from 59.1% to 40.9% (P < 0.001), demonstrating enhanced mobility post-procedure. Passive internal rotation: Similar improvement was observed in passive movement, with a reduction in restriction from 59.1% to 40.9% (P < 0.001). Up to L5 movement: The proportion of patients achieving internal rotation up to L5 remained unchanged at 50.0% pre- and post-procedure, suggesting this subgroup may require additional interventions for further improvement (Fig. 3).

Adhesive capsulitis, commonly known as frozen shoulder, is a condition characterized by pain and restricted ROM in the shoulder joint. Hydrodilatation, a treatment involving the distension of the joint capsule with fluid, has been explored as a therapeutic option for this condition. This study aimed to evaluate the efficacy of hydrodilatation in improving shoulder function and ROM over a 1-year period. The findings indicate significant improvements, aligning with some existing literature, though discrepancies persist regarding the magnitude and duration of benefits reported across studies. The present study demonstrated substantial enhancements in shoulder movement’s post-hydrodilatation. Specifically, significant gains were observed in abduction, adduction, forward flexion, and external rotation, with P < 0.001. Internal rotation restrictions decreased notably from 59.1% to 40.9% post-procedure. These outcomes are consistent with the findings of Elnady et al., who reported significant improvements in external rotation and overall shoulder function following ultrasound-guided hydrodilatation through the anterior approach. Their study highlighted that targeting the rotator interval could effectively alleviate motion restrictions associated with adhesive capsulitis [3]. However, the literature presents mixed evidence regarding the efficacy of hydrodilatation. A systematic review and meta-analysis by Poku et al. concluded that hydrodilatation leads to at least transient improvements in shoulder disability and passive external rotation compared with intra-articular corticosteroid injections. The review suggested that while hydrodilatation may offer short-term benefits, its long-term superiority over other treatments remains uncertain [4]. Functional assessments in this study utilized the ASES and CMSs, revealing progressive improvement up to 1 year post-intervention. This sustained recovery suggests that hydrodilatation offers long-term benefits in managing adhesive capsulitis. Similarly, Catapano et al. found that combining hydrodilatation with corticosteroid injections expedited the recovery of pain-free ROM, particularly within the first 3 months. Their systematic review indicated that the greatest benefit is experienced within the initial 3 months of intervention, emphasizing the potential of hydrodilatation to accelerate early recovery [5]. In contrast, a meta-analysis by Saltychev et al. suggested that hydrodilatation has only a small, clinically insignificant effect when treating adhesive capsulitis. This discrepancy may stem from variations in study design, patient populations, and hydrodilatation techniques. The authors emphasized the need for further research to establish standardized protocols and to determine the true efficacy of hydrodilatation in comparison to other treatment modalities [6]. Comparative studies have explored the efficacy of hydrodilatation relative to other interventions. A randomized controlled trial by Swaroop et al. compared intra-articular steroid injections alone to hydrodilatation combined with intra-articular steroids in patients with frozen shoulder. The study found that better clinical results were obtained at 6 weeks and 3 months with the group receiving corticosteroid only, suggesting that intra-articular steroid injection alone may be a more desirable method of management during the frozen phase of frozen shoulder than hydrodilatation with intra-articular steroid injection [7]. Another study by Latzka et al. compared hydrodilatation to corticosteroid injections in the treatment of adhesive capsulitis. The findings indicated that hydrodilatation was not superior to corticosteroid injections in terms of pain reduction and functional improvement. This aligns with the results of the present study, which demonstrated significant improvements with hydrodilatation, but does not conclusively establish its superiority over corticosteroid injections [8]. The technique and approach used during hydrodilatation may influence outcomes. A systematic review with meta-analysis by Rhim et al. compared anterior and posterior approaches for hydrodilatation. The study found that while pain reduction was similar between the two approaches, the anterior approach resulted in greater improvements in external rotation and abduction at 12 weeks. This suggests that the choice of approach can impact the efficacy of hydrodilatation in restoring specific shoulder movements [9]. In addition, the inclusion of corticosteroids in the hydrodilatation procedure has been examined. A study by Catapano et al. indicated that combining hydrodilatation with corticosteroid injections potentially expedites recovery of pain-free ROM, with the greatest benefit experienced within the first 3 months. This highlights the potential advantage of incorporating corticosteroids to enhance the therapeutic effects of hydrodilatation [5]. The present study’s strengths include a prospective design and a 1-year follow-up period, providing robust data on the long-term effects of hydrodilatation. Nonetheless, limitations such as the lack of a control group and a relatively small sample size may affect the generalizability of the findings. In addition, variations in hydrodilatation techniques, including the volume of fluid injected and the anatomical approach, were not standardized, which could influence the outcomes. Future studies should aim to address these limitations by incorporating larger, randomized controlled trials with standardized protocols to validate the efficacy of hydrodilatation in managing adhesive capsulitis. This study supports hydrodilatation as an effective intervention for improving shoulder mobility and function in patients with adhesive capsulitis, with benefits persisting up to 1 year. The findings align with some existing literature, though discrepancies highlight the need for further research to standardize hydrodilatation protocols and to compare its effectiveness with other treatment modalities[10].Understanding the optimal patient selection, procedural techniques, and combination therapies will be crucial in establishing hydrodilatation as a definitive treatment for adhesive capsulitis.
The present study evaluated the functional outcomes of hydrodilatation in patients with adhesive capsulitis, demonstrating significant improvements in shoulder ROM and functional scores (ASES and CMSs) over a 1-year follow-up period, highlighting the long-term effectiveness of hydrodilatation in restoring shoulder function. Post-procedure, there was a marked increase in abduction, adduction, forward flexion, and external rotation, with a statistically significant reduction in movement restriction, particularly in internal rotation (P < 0.001). Comparative analysis with previous studies suggests that hydrodilatation offers superior short-term relief compared to corticosteroid injections alone, especially within the first 3 months post-treatment. Despite its efficacy, hydrodilatation is not a definitive cure for adhesive capsulitis and should be integrated into a comprehensive treatment plan, including physiotherapy and patient education. Hydrodilatation is a safe, minimally invasive, and effective intervention for improving shoulder mobility and function in adhesive capsulitis, with sustained benefits. Future research should focus on standardizing hydrodilatation protocols, optimizing combination therapies, and identifying ideal patient profiles for maximal therapeutic benefit.
Limitations
The lack of a control group and relatively small sample size in this study are limitations, emphasizing the need for larger, multi-center randomized controlled trials to further validate its role in clinical practice.
An minimally invasive procedure for adhesive capsulitis with good clinical and functional outcome which can be incorporated into the protocol for management of adhesive capsulitis.
References
- 1.Ramirez J. Adhesive capsulitis: Diagnosis and management. Am Fam Physician 2019;99:297-300. [Google Scholar | PubMed]
- 2.Yoon JP, Chung SW, Kim JE, Kim HS, Lee HJ, Jeong WJ, et al. Intra-articular injection, subacromial injection, and hydrodilatation for primary frozen shoulder: A randomized clinical trial. J Shoulder Elbow Surg 2016;25:376-83. [Google Scholar | PubMed]
- 3.Elnady B, Rageh EM, Hussein MS, Abu-Zaid MH, Desouky DE, Ekhouly T, et al. In shoulder adhesive capsulitis, ultrasound-guided anterior hydrodilatation in rotator interval is more effective than posterior approach: A randomized controlled study. Clin Rheumatol 2020;39:3805-14. [Google Scholar | PubMed]
- 4.Poku D, Hassan R, Migliorini F, Maffulli N. Efficacy of hydrodilatation in frozen shoulder: A systematic review and meta-analysis. Br Med Bull 2023;147:121-47. [Google Scholar | PubMed]
- 5.Catapano M, Mittal N, Adamich J, Kumbhare D, Sangha H. Hydrodilatation with corticosteroid for the treatment of adhesive capsulitis: A systematic review. PM R 2018;10:623-35. [Google Scholar | PubMed]
- 6.Saltychev M, Laimi K, Virolainen P, Fredericson M. Effectiveness of hydrodilatation in adhesive capsulitis of shoulder: A systematic review and meta-analysis. Scand J Surg 2018;107:285-93. [Google Scholar | PubMed]
- 7.Swaroop VT, Patil SS, Katti G, Katti C. Intra-articular steroid injection alone versus hydrodilatation with intra-articular steroid injection in patients with frozen shoulder: A randomized clinical trial. Cureus 2023;15:e37560. [Google Scholar | PubMed]
- 8.Latzka E, Cali M, Ishii H, Portugal S, Soo Hoo J. Hydrodilatation versus corticosteroid injection in treatment for adhesive capsulitis. PM R 2023;15:1580-7. [Google Scholar | PubMed]
- 9.Rhim HC, Schon JM, Xu R, Schowalter S, Ha J, Hsu C, et al. Targeting the sweet spot: A systematic review with meta-analysis of anterior versus posterior glenohumeral joint injections for adhesive capsulitis. Clin J Sport Med 2025;35:1-12. [Google Scholar | PubMed]
- 10.Bell S, Coghlan J, Richardson M. Hydrodilatation in the management of shoulder capsulitis. Australas Radiol 2003;47:247-51. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 A Prospective Randomized Study Comparing the Efficacy of Electrotherapy to Ultrasound – Guided Intra-Articular Steroid Injections for Frozen Shoulder
August 1, 2025 A Prospective Randomized Study Comparing the Efficacy of Electrotherapy to Ultrasound – Guided Intra-Articular Steroid Injections for Frozen Shoulder February 1, 2026 Outcomes of Clinico-radiologically Predetermined Patient-specific Multi-site Steroid Injection in Primary Frozen Shoulder: A Prospective Study
February 1, 2026 Outcomes of Clinico-radiologically Predetermined Patient-specific Multi-site Steroid Injection in Primary Frozen Shoulder: A Prospective Study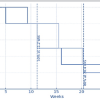 December 1, 2025 Functional Outcome of Intra-articular Platelet-Rich Plasma in the Treatment of Frozen Shoulder
December 1, 2025 Functional Outcome of Intra-articular Platelet-Rich Plasma in the Treatment of Frozen Shoulder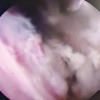 November 1, 2025 Comparative Efficacy of Manipulation Under Anaesthesia Versus Arthroscopic Capsular Release in Primary Frozen Shoulder: A Prospective Randomized Study
November 1, 2025 Comparative Efficacy of Manipulation Under Anaesthesia Versus Arthroscopic Capsular Release in Primary Frozen Shoulder: A Prospective Randomized Study