
This case demonstrates the importance of recognizing intramuscular myxomas in uncommon locations and the role of imaging and histopathology in ensuring an accurate diagnosis. Surgical excision is the definitive treatment that prevents recurrence and optimizes patient outcome.
Dr. Mikail Chatzivasiliadis, Aristotle University School of Medicine, Thessaloniki, Greece. E-mail: mikail@chatzi.com
Abstract
Introduction: Intramuscular myxomas (IMMs) are rare benign tumors of mesenchymal origin, typically occurring in middle-aged women. These tumors are characterized by hypocellular, hypovascular lesions rich in extracellular myxoid stroma. IMMs are most commonly found in the heart but rarely may affect large muscle groups such as the thighs, shoulders, and buttocks. While they are generally isolated lesions, IMMs may be associated with syndromes such as Mazabraud syndrome or McCune–Albright syndrome. Accurate diagnosis relies on imaging and histopathological evaluation, with surgical excision being the definitive treatment.
Case Report: We present the case of a 25-year-old female patient who reported a noticeable dysmorphism in the inner thigh region without pain or functional impairment. Magnetic resonance imaging revealed a smooth-bordered, oval lesion in the vastus medialis muscle measuring 2.8 × 2 cm. A percutaneous biopsy confirmed the diagnosis of an IMM. Eventually, the intramuscular myxoma was surgically removed without complications.
Conclusion: Accurate imaging and histopathological confirmation remain critical for diagnosis, and a case such as ours reinforces the need to consider IMMs in rare locations to optimize patient care.
Keywords: Intramuscular myxoma, vastus medialis, benign tumor, thigh mass, myxoma.
Intramuscular myxomas (IMM) are rare benign tumors that originate from mesenchymal tissue. They are commonly characterized as hypocellular, hypovascular lesions high in extracellular myxoid stroma [1,2,3]. When these tumors are located within muscular tissue, they tend to be more vascularized and have increased cellularity which could lead to a misdiagnosis of sarcoma [2,4]. Virchow was one of the first to encounter these tumors and described them as mucous-rich tissue that resembled the ones found in the umbilical cord, laying the foundation for what we now know as myxoma [5]. However, stout later refined the definition by identifying IMMs as neoplasms composed of undifferentiated stellate cells within a soft, myxoid environment containing fragile reticular fibers [6]. IMMs are mostly diagnosed in middle-aged and older female adults, between the ages of 40 and 70 [7,8]. They have an estimated incidence of 0.1–0.3/100,000 people with women making up 66% of cases. In the present case, we describe a patient with an IMM located in the vastus medialis muscle of the left thigh.
Clinical presentation
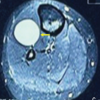
A 25-year-old female patient presented to our clinic in 2022, reporting a noticeable dysmorphism in the inner thigh region. Even though the patient’s thigh had a noticeable irregularity, she did not have any pain or functional impairment. A magnetic resonance imaging (MRI) scan was performed to further investigate this lesion, which revealed a smooth-bordered, oval lesion within the vastus medialis muscle. The lesion measured 2.8 × 2 cm and had a hyperintense T2 signal on imaging, which already showed us that it was of myxomatous or cystic nature. In Fig. 1, we display the MRI images consistent with the described findings. Based on these findings, we had a potential diagnosis of an intramuscular myxoma, but further research was needed.

Initial management and histological findings
The following year, the patient underwent a percutaneous biopsy at a public hospital to confirm the initial diagnosis. A histological analysis of the biopsy sample was done and confirmed the diagnosis of an intramuscular myxoma. The results of this analysis are shown in Fig. 2. The histology revealed dense myxoid tissue with elongated and stellate cells. There was no sign of nuclear atypia or evidence of mitotic activity. Immunohistochemical analysis showed that the tumor cells were positive for CD34 and negative for S100, SOX10, EMA, MUC4, SMA, and CD99. This is in line with our initial diagnosis of an IMM. The Ki-67 proliferation index was estimated at 5%, meaning there was low proliferative activity. It is important to mention that the myxoid tissue extended far beyond the excision borders. The gross pathology described the lesion as white and compact. In addition, it contained cystic foci, which measured around 2.1 × 1.5 × 0.7 cm. Following the biopsy, the patient returned the next year and did another MRI scan which revealed a size reduction of the lesion to 1.2 × 0.8 cm, compared to its initial dimensions of 2.8 × 2 cm. The reduction in size was likely because of tissue sampling following the biopsy procedure. Importantly, no pathological signal changes were detected in the surrounding muscles, soft tissues, or bone.

Surgical intervention
A few months later, the IMM was surgically excised and successfully removed. Postoperatively, the patient had a good recovery without any complications. Regular follow-up was recommended to make sure there was no recurrence. Fig. 3 shows an image taken intraoperatively of the IMM together with its dimensions.
IMMs are characterized as oval masses and their fibrous capsule is mostly incomplete, which makes it easier for them to infiltrate into adjacent muscle tissue. When they are cut, they reveal a gelatinous, gray-white appearance with cystic spaces filled with fluid [1]. Histologically, IMMs are hypocellular tumors composed of spindle-shaped or stellate cells embedded in an environment rich in myxoid stroma. In addition, the cells exhibit hyperchromatic pyknotic nuclei with minimal cytoplasm, and their reticulin fibers are loosely distributed throughout the stroma [1,8]. Immunohistochemical studies show that IMMs stain positive for vimentin and variable staining for CD34 and actin, which confirms their mesenchymal origin. When the IMMs are being stained for the S-100 protein, it helps us to differentiate IMMs from neural or Schwann cell-derived tumors [1]. The absence of mitotic activity, nuclear atypia, and necrosis further supports their benign nature [1,3]. IMMs normally present as slow-growing, painless masses that go unnoticed until they cause swelling. These masses are mostly reported in large muscle areas, the most common extracardiac site of manifestation with 51% of all IMM cases is the thigh [3,7]. Other common sites include the arms, calves, and buttocks. IMMs mostly occur as isolated lesions, but they can also arise in association with Mazabraud syndrome, which is when we have multiple myxomas together with fibrous dysplasia [9]. In even more rare cases, they might be linked to McCune–Albright syndrome, which is a condition characterized by fibrous dysplasia, café-au-lait spots, and endocrine dysfunctions [8,10]. It is important to recognize these possible associations to provide the best possible treatment plan for the patient. Although imaging cannot replace histopathology for the definitive diagnosis of an IMM, MRI is the gold standard due to its soft-tissue contrast that accurately characterizes this pathology. On T1-weighted images, the tumor lesion appears to be hypointense and well-circumscribed, whereas on T2-weighted images they tend to be hyperintense [11]. Girish et al. described a distinct feature of IMM that is often seen on MRIs, the “bright caps sign” [12]. This radiologic feature refers to the prominence of peritumoral fat that is located at the superior and inferior poles of the lesion on T1 imaging. In addition, adjacent muscle also tends to have increased signal intensity on T2-weighted imaging or fluid-sensitive sequences [4,12]. Besides MRI, imaging modalities such as ultrasound and computed tomography (CT) scans, may also be used as supplementary tools to diagnose IMM. CT imaging shows them as homogenous, low-attenuation lesions that are clearly delineated from surrounding structures within skeletal muscle [4,13]. A combination of imaging to differentiate the different kinds of malignancies, such as angiomyxoma, myxoid liposarcoma, liposarcoma, or myxoid chondrosarcoma, is very important. However, the only way to get a definitive diagnosis of IMM is by doing a histological examination with a core needle biopsy [8,13]. In the present case, a percutaneous biopsy was preferred over resection to minimize trauma, especially since the patient was young and there were no symptoms present. The exact cause of IMMs still remains unknown. What we do know is that genetically, IMMs have been linked to the R201H and R201C point mutations in the Guanine Nucleotide binding protein, Alpha Stimulating (GNAS) gene. The GNAS gene plays an important role in the intracellular pathways that regulate cell growth and differentiation by encoding the Gαs protein. When normal signaling is disrupted by somatic mutations, which are genetic changes that occur during a person’s life instead of being inherited, it can lead to the development of IMMs [8]. To identify these mutations, highly sensitive sequencing techniques such as TaqMan assays and single-molecule tagged molecular inversion probes have been developed to accurately detect GNAS mutations, which have been proven useful in syndromic and non-syndromic cases [8,14,15]. While the exact role of GNAS mutations in the pathogenesis of IMMs still needs further research, the fact that we can identify these genetic alterations represents a big step toward understanding the etiology of these tumors. In most cases, the primary treatment for IMMs is to surgically excise the tumor along with a wide margin of healthy tissue to minimize the risk of recurrence [1,16]. Recurrence rates are very low, especially in non-syndromic cases, which make surgery the definitive treatment for these benign tumors. IMMs have an excellent prognosis as malignant transformation has not yet been observed in this type of tumor. Patients are expected to fully recover, which favors the long-term outcome [1,16].
In the present case, we described an IMM which was located in the vastus medialis muscle of the left thigh, a site of manifestation that has rarely been mentioned in the literature. The fact that we identified an IMM in the vastus medialis muscle widens our current understanding of where these tumors can occur. This makes it extremely important for physicians to include IMMs in the differential diagnosis of intramuscular masses, especially in uncommon locations. This way, we reduce the risk of misdiagnosing IMMs as aggressive tumors and avoid unnecessary interventions that could negatively alter the patient’s outcomes. As mentioned before, surgical excision remains the definitive treatment of IMM. However, it is crucial to get an accurate diagnosis through imaging and histopathological confirmation to help guide the right surgical planning. Studies such as ours may provide insights and pave the way for better clinical awareness in areas of the body where IMMs are rarely reported.
IMM should be recognized as a potential diagnosis for soft-tissue masses, even when they are encountered in uncommon locations such as the vastus medialis. In addition, this report discusses the importance of various imaging modalities in accurately diagnosing these lesions.
References
- 1.Sağlam S, Orhan Ş, Orhan Z, Turhan Y, Arıcan M. Intramuscular myxoma in the gluteus maximus muscle after continuous intramuscular injections. Jt Dis Relat Surg Case Rep 2022;1:31-4. [Google Scholar | PubMed]
- 2.Granel-Villach L, Alcalde-Sánchez M, Salvador-Marín M, García-Calvo R, Santonja-López N, Salvador-Sanchís JL. Diagnóstico diferencial y manejo de mixomas intramusculares: Revisión de nuestra experiencia [Differential diagnosis and management of intramuscular myxomas: A review of our experience]. Cir Cir 2017;85:356-60. [Google Scholar | PubMed]
- 3.Özbek N, Danaci M, Okumus B, Gürsel B, Çakir Š, Dabak N, et al. Recurrent intramuscular myxoma: Review of the literature, diagnosis and treatment options. Turk J Cancer 2006;36:75-8. [Google Scholar | PubMed]
- 4.El Aissaoui T, Lachkar A, Abdeljaouad N, Yacoubi H. Right adductor compartment intramuscular myxoma: A rare case report. Int J Surg Case Rep 2024;116:109402. [Google Scholar | PubMed]
- 5.Virchow R. Cellular Pathology as Based Upon Physiological and Pathological Histology. United States: J. B. Lippincott; 1863. p. 525-6. [Google Scholar | PubMed]
- 6.Stout AP. Myxoma, the tumor of primitive mesenchyme. Ann Surg 1948;127:706-19. [Google Scholar | PubMed]
- 7.Murphey MD, McRae GA, Fanburg-Smith JC, Temple HT, Levine AM, Aboulafia AJ. Imaging of soft-tissue myxoma with emphasis on CT and MR and comparison of radiologic and pathologic findings. Radiology 2002;225:215-24. [Google Scholar | PubMed]
- 8.Jabbar S, Jamil OBK, Ali R, Zulfikar I, Tharwani ZH. Intramuscular myxoma of the thigh: A case report. SAGE Open Med Case Rep 2023;11:2050313X231200120. doi: 10.1177/2050313X231200120. [Google Scholar | PubMed | CrossRef]
- 9.Kabukcuoglu F, Kabukcuoglu Y, Yilmaz B, Erdem Y, Evren I. Mazabraud’s syndrome: Intramuscular myxoma associated with fibrous dysplasia. Pathol Oncol Res 2004;10:121-3. [Google Scholar | PubMed]
- 10.Logel RJ. Recurrent intramuscular myxoma associated with Albright’s syndrome. J Bone Joint Surg Am 1976;58:565-8. [Google Scholar | PubMed]
- 11.Bancroft LW, Kransdorf MJ, Menke DM, O’Connor MI, Foster WC. Intramuscular myxoma: Characteristic MR imaging features. AJR Am J Roentgenol 2002;178:1255-9. [Google Scholar | PubMed]
- 12.Girish G, Jamadar DA, Landry D, Finlay K, Jacobson JA, Friedman L. Sonography of intramuscular myxomas: The bright rim and bright cap signs. J Ultrasound Med 2006;25:865-9; quiz 870-1. [Google Scholar | PubMed]
- 13.Yaligod V, Ajoy SM. Intramuscular myxoma - a rare tumor. J Orthop Case Rep 2013;3:38-41. [Google Scholar | PubMed]
- 14.Al Abdulsalam A, Al Safi S, Aldaoud S, Al-Shadidi N, Dhar PM. Intramuscular myxoma of the left thigh: A case report. Int J Surg Case Rep 2022;100:107710. [Google Scholar | PubMed]
- 15.Bekers EM, Eijkelenboom A, Rombout P, van Zwam P, Mol S, Ruijter E, et al. Identification of novel GNAS mutations in intramuscular myxoma using next-generation sequencing with single-molecule tagged molecular inversion probes. Diagn Pathol 2019;14:15. [Google Scholar | PubMed]
- 16.Lawan Abdou A, Barrached M, Lachkar A, Abdeljaouad N, Yacoubi H. The clinical, radiological, and histopathological characteristics of intramuscular myxoma: A case report. Cureus 2024;16:e63144. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report
July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases
February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases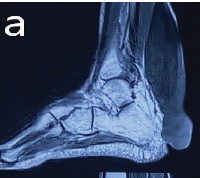 September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report
September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report August 1, 2025 Solitary Langerhans Cell Histiocytosis of the Distal Radius in an 11-Month-Old Infant: A Case Report
August 1, 2025 Solitary Langerhans Cell Histiocytosis of the Distal Radius in an 11-Month-Old Infant: A Case Report