
Schwannomas arising from the deep peroneal nerve are rare and should be considered in patients presenting with chronic leg pain and localized swelling, as early surgical excision leads to excellent outcomes.
Dr. Divesh Jalan, Central Institute of Orthopaedics, VMMC and Safdarjung Hospital, New Delhi, India. E-mail: dvsh_jalan@yahoo.com
Abstract
Introduction: Schwannomas, also known as neurilemmomas, are the most common benign peripheral nerve tumours. Schwannomas arising from deep peroneal nerves are rare and often remain clinically silent until local mass effects cause pain, dysesthesia, or motor/sensory deficits.
Case Report: A 20-year-old female presented with a 6-month history of pain and swelling in her right leg, with difficulty in standing and walking for longer durations. Imaging revealed a well-defined lesion along the deep peroneal nerve. Surgical enucleation of the tumour was performed, and histopathological examination confirmed the diagnosis of schwannoma. Postoperatively, the patient experienced a significant improvement in symptoms with no recurrence at the latest follow-up.
Conclusion: Schwannomas arising from deep peroneal nerves are rare. However, they should be considered in patients with chronic leg pain and swelling with neurological symptoms in the leg and calf region. Surgical excision is the treatment of choice, and complete resection is generally curative.
Keywords: Schwannoma, neurilemmoma, peripheral nerve tumors, peroneal nerve, benign tumor.
Schwannomas, also known as neurilemmomas, are benign tumours of the peripheral nerves arising from Schwann cells. Schwannomas most frequently occur between the third and sixth decades of life without any gender or ethnic preponderance [1]. These tumours typically remain asymptomatic until they cause local mass effects, leading to symptoms such as dysaesthesia, pain, or muscle weakness. Peripheral nerve sheath tumours may arise anywhere along the nerve, from the dorsal root ganglion to the terminal nerve branches. The head and neck, ulnar nerve, and peroneal nerve regions are common sites for these tumours [2]. The common peroneal nerve is vulnerable to injury due to its superficial anatomical course, making it susceptible to trauma or compression. There are multiple reports of schwannoma arising from the common peroneal nerve (citation); however, schwannoma arising from a deep peroneal nerve is extremely rare, with only a few case reports in the literature [3]. We, therefore, present one such case of schwannoma arising from the deep peroneal nerve in a young female affecting her daily activities.
A 20-year-old female presented with pain and localised swelling in her right leg, along with difficulty in prolonged standing and walking for the past 6 months. The patient reported a moderate-intensity, burning pain that was intermittent, radiating distally, along with a feeling of heaviness in the calf. The pain increased on prolonged standing and walking and was relieved with rest and analgesics. On clinical examination, a palpable mass measuring 5 cm × 3 cm was noted over the proximal lateral aspect of the right leg (Fig. 1).
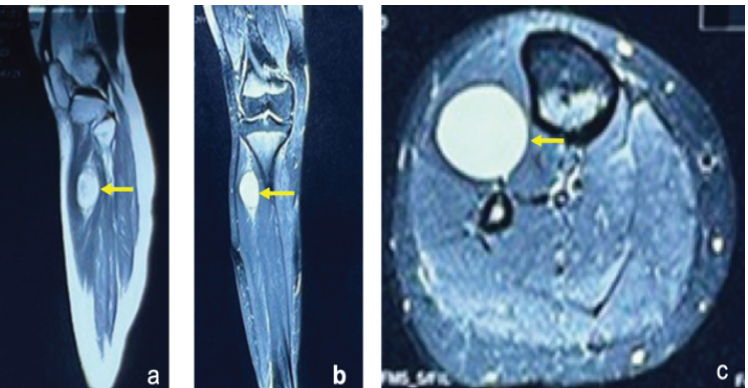
Figure 1: T2 sagittal, STIR coronal, and axial magnetic resonance imaging images (a, b, c) of the left upper leg demonstrate an oval T2-hyperintense encapsulated lesion (arrow) in the anterolateral intermuscular compartment.
The skin overlying the mass appeared normal. The mass was firm in consistency and tender. Manipulation of the swelling triggered sharp, lancinating pain in the leg and foot. Ankle plantar and dorsiflexion were normal, and sensory function remained intact. Magnetic resonance imaging (MRI) of the left leg revealed a well-defined, T2 hyperintense, homogeneously enhancing oval lesion (3 cm × 3 cm × 4 cm) located in the intermuscular plane of the anterolateral compartment of the proximal leg arising from the deep peroneal nerve (Fig. 2).
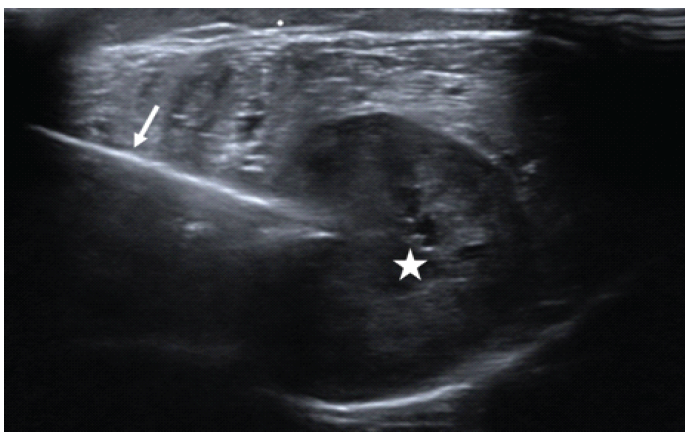
Figure 2: Ultrasound image demonstrating ultrasound-guided core needle biopsy of the lesion. (Arrow: Biopsy needle, Asterisk: Lesion).
Based on clinico-radiological examination, a provisional diagnosis of benign nerve sheath tumour was considered. The patient then underwent core-needle biopsy of the lesion under ultrasound guidance (Fig. 3), which confirmed the diagnosis of a schwannoma with fatty and cystic degeneration.
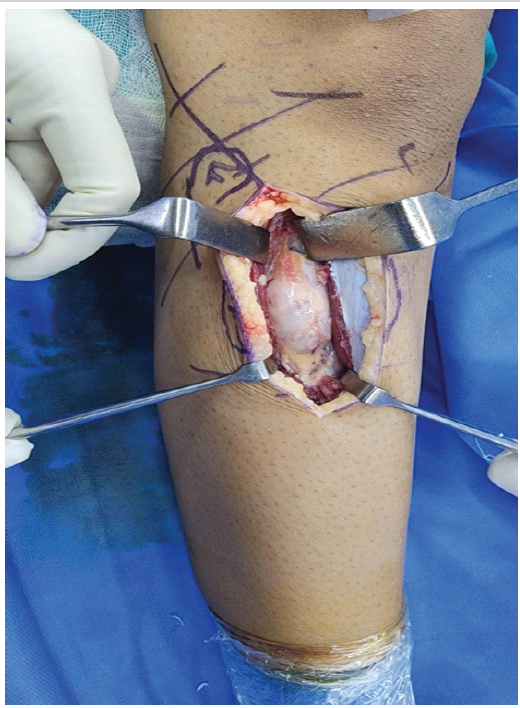
Figure 3: Intraoperative image showing encapsulated tumor in continuity with the deep peroneal nerve.
Immunohistochemical analysis showed that the tumour cells were positive for S100 and negative for CD34 and desmin (Fig. 4).
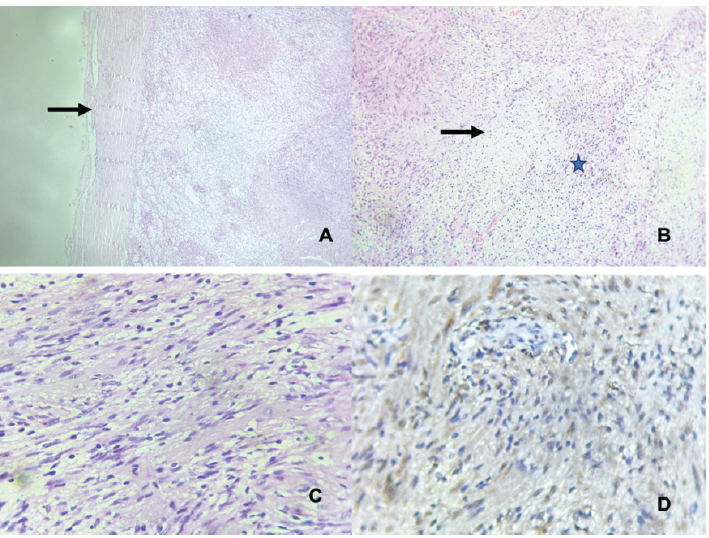
Figure 4: (a) demonstrates the encapsulated lesion (arrow), (b) shows the lesion having alternate hypercellular (asterisk) and hypocellular areas (arrow), (c) shows spindle cells, ill-defined cytoplasm with elongated nuclei, and (d) shows the immunohistochemistry image demonstrating positive S-100.
After informed consent from the patient, she was planned for surgical enucleation. Intraoperatively, the tumour was found to be encapsulated and in continuity with the deep peroneal nerve. The tumour was enucleated, and the remaining sheath was repaired using Ethilon 6-0. Postoperatively, the excised tumour was sent for biopsy, which confirmed it to be a schwannoma. The patient had an uneventful recovery, and her symptoms improved significantly. At the latest follow-up after 1 year, the patient is asymptomatic and has no recurrence of the lesion.
Schwannomas are the most common benign peripheral nerve sheath tumours, arising from the Schwann cells, which are responsible for forming the myelin sheath around peripheral nerves. They are present in the sacral plexus, the brachial plexus, and the sciatic nerve [4,5]. Despite being the most common benign peripheral nerve sheath tumour, its presence in the lower limbs is reported to be only 1% [5]. They are typically solitary, but multiple tumours can be seen in conditions such as schwannomatosis or neurofibromatosis type 2. Since these tumours have a slow-growing pattern, patients are mostly asymptomatic until they cause local mass effects, leading to symptoms such as dysaesthesia, pain, or muscle weakness. The diagnosis involves the triad of clinical history and physical examination, imaging, and histopathological studies. On MRI, a well-circumscribed mass is seen, which is isointense or hypointense on a T1-weighted image, whereas a heterogeneously hyperintense mass with a thin peripheral rim of fat is seen on a T2-weighted image [6]. However, in neurofibroma, the image is hypointense on T1, while on T2, a hyperintense rim with the central area of a low signal may be seen, which is likely due to the dense central area of collagenous stroma. Magnetic resonance neurography is the modality of choice for its ease in confirming clinical suspicion of peripheral neuropathy by directly showing the nerve abnormality or regional muscle denervation changes to assess the extent of the abnormality in nerve injuries or the disease load in diffuse peripheral nerve lesions, such as hereditary neuropathies and neurofibromatosis [7]. However, these modalities cannot differentiate from other benign or malignant tumours with the same consistency, such as ganglion, lipoma, myxoma, neurofibroma, or malignant peripheral nerve sheath tumour; hence, histopathological analysis is crucial [8]. In histopathology, a schwannoma is well circumscribed and surrounded by a capsule. It contains fascicles of Schwann cells with a spindle-cell morphology (Antoni A) or may become loosely arranged (Antoni B pattern). Furthermore, these tumour cells are positive for S100, podoplanin (D2-40), calretinin, and SOX10 and negative for CD34 and desmin [8]. Mutations of the NF2, SMARCE1, SMARCB1, LZTR1, and SUFU genes have been associated with schwannoma formation [9]. Small, solitary schwannomas can be managed conservatively. However, surgical excision is indicated in cases of progressive neurological deficits, persistent pain, suspected malignancy, or tumour growth. Schwannomas can be easily dissected from the nerve without damaging the nerve’s continuity, as they rarely invade into the nerve itself, as seen in our case [10]. Post-operative loss of nerve function is uncommon. Risk factors for complications and postoperative neurological deficits include large tumour volume, proximal location, and involvement of major motor nerves [11]. Studies have reported that post-operative sensory deficits, such as paraesthesia or hypoesthesia, often improve over time [11]. Tumour size, surgical technique, and intraoperative electrophysiological monitoring are critical to reducing the risk of neurological deficits.
Schwannomas are benign peripheral nerve sheath tumours that rarely undergo malignant transformation. Although schwannomas of the lower limb are rare, they should be suspected in patients with chronic leg pain, localised swelling, numbness, or weakness. Evaluating the patient’s clinical condition and the characteristics of the lesion is crucial for determining the most appropriate treatment. For symptomatic schwannomas, surgical excision is the treatment of choice, and complete resection is generally curative.
Deep peroneal nerve schwannoma should be considered in patients with unexplained chronic leg pain and localised swelling, as timely diagnosis and surgical excision result in excellent functional outcomes.
References
- 1. Sheikh MM, De Jesus O. Vestibular schwannoma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 2. Woertler K. Tumors and tumor-like lesions of peripheral nerves. Semin Musculoskelet Radiol 2010;14:547-58. [Google Scholar] [PubMed]
- 3. Sharma RR, Pawar SP, Dey P. An occult schwannoma of the deep peroneal nerve presenting with neuralgia mimicking sciatica: Case report and review of the literature. Ann Saudi Med 2000;20:57-9. [Google Scholar] [PubMed]
- 4. Inoue M, Kawano T, Matsumura H, Mori K, Yoshida T. Solitary benign schwannoma of the brachial plexus. Surg Neurol 1983;20:103-8. [Google Scholar] [PubMed]
- 5. Rafai MA, El Otmani H, Rafai M, Bouhaajaj FZ, Largab A, Trafeh M, et al. Peroneal nerve schwannoma presenting with a peroneal palsy. Rev Neurol (Paris) 2006;162:866-8. [Google Scholar] [PubMed]
- 6. Crist J, Hodge JR, Frick M, Leung FP, Hsu E, Gi MT, et al. Magnetic resonance imaging appearance of schwannomas from head to toe: A pictorial review. J Clin Imaging Sci 2017:7:38. [Google Scholar] [PubMed]
- 7. Chhabra A, Faridian-Aragh N, Chalian M, Soldatos T, Thawait SK, Williams EH, et al. High-resolution 3-T MR neurography of peroneal neuropathy. Skeletal Radiol 2012;41:257-71. [Google Scholar] [PubMed]
- 8. Phalen GS. Neurilemmomas of the forearm and hand. Clin Orthop Relat Res 1976;114:219-22. [Google Scholar] [PubMed]
- 9. Rodriguez FJ, Folpe AL, Giannini C, Perry A. Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathol 2012;123:295-319. [Google Scholar] [PubMed]
- 10. Pathmanaban ON, Sadler KV, Kamaly-Asl ID, King AT, Rutherford SA, Hammerbeck-Ward C, et al. Association of genetic predisposition with solitary schwannoma or meningioma in children and young adults. JAMA Neurol 2017;74:1123-9. [Google Scholar] [PubMed]
- 11. Raj C, Chantelot C, Saab M. Predictive factors of postoperative deficit and functional outcome after surgery for upper limb schwannomas: Retrospective study of 21 patients. Hand Surg Rehabil 2020;39:229-34. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases
February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases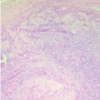 January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report
January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report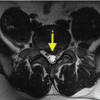 January 1, 2026 Recurrent Symptoms in Lumbar Disc Herniation with Concomitant Schwannoma: The Role of Tumor Microenvironment and Anti-Inflammatory Therapy
January 1, 2026 Recurrent Symptoms in Lumbar Disc Herniation with Concomitant Schwannoma: The Role of Tumor Microenvironment and Anti-Inflammatory Therapy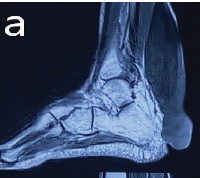 September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report
September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report