
Osteochondroma of D12 is a rare phenomenon, but it should also be kept as a differential diagnosis while treating patients with unexplained back symptoms in a normal X-ray.
Dr. Nitish Kumar, Department of Orthopedics, All India Institute of Medical Sciences, Gorakhpur, Uttar Pradesh, India. E-mail: nitishaiims@gmail.com
Introduction: Osteochondromas are benign bony lesions arising from the metaphysis of long bones, commonly arising from the distal femur, proximal tibia, and proximal humerus, with rare incidence of its presence over the flat bones such as the scapula and pelvis. The spine can be rarely affected by osteochondromas in 1–4% of all cases. The origin of osteochondroma from the mammillary process of the D12 vertebra is very rare. Hence, we are reporting this rare phenomenon.
Case Report: An 11-year-old female presented with the complaints of gradually progressive swelling in the mid-back region with discomfort on lying down in the supine position. Based on clinical and radiological findings, a provisional diagnosis of osteochondroma arising from D12 vertebrae was made and planned for excisional biopsy under general anesthesia. Histopathology of the excised bone mass was consistent with osteochondroma. The patient was followed for 1 year, in which no signs of recurrence were found, and she was carrying out her activities of daily living without any discomfort.
Conclusion: Osteochondroma of D12 is a rare phenomenon, but it should also be kept as a differential diagnosis while treating patients with unexplained back symptoms in a normal X-ray. Surgical excision should be kept reserved for large osteochondromas outside of the neural canal or tumors causing neural symptoms.
Keywords: Osteochondroma, spinal osteochondroma, dorsal spine.
Osteochondromas are benign bony lesions arising from the metaphysis of long bones, having cartilage-capped outgrowths that continue to grow till skeletal maturity. The osteochondromas commonly arise from the distal femur, proximal tibia, and proximal humerus, with rare incidence of their presence over the flat bones like the scapula and pelvis [1]. The spine can be rarely affected by osteochondromas in 1–4% of all cases. The spinal osteochondromas are usually found in cervical and upper dorsal vertebrae [1]. The origin of osteochondroma from the mammillary process of the D12 vertebra is very rare. Hence, we are reporting this rare phenomenon.
An 11-year-old female presented with the complaints of gradually progressive swelling in the mid-back region with discomfort on lying down in the supine position. On physical examination, we found a globular, non-tender bony hard swelling of size 5 cm × 3 cm on the left para-spinal region of D11-D12 vertebra. The surface was smooth, and margins were well defined. The lesion was found to be arising from D12 Vertebrae with normal overlying skin. There was no neurological symptom and no similar swelling elsewhere in the body. The plain X-ray anteroposterior and lateral views of the dorsolumbar spine were unremarkable. The non-contrast magnetic resonance imaging (MRI) of the dorso-lumber region showed a well-defined extra-medullary lesion arising from the left mammillary process of D12 vertebra with a cartilage cap of 2 mm thickness. The medullary cavity of the lesion was found to be in continuity with the parent bone (Fig. 1).
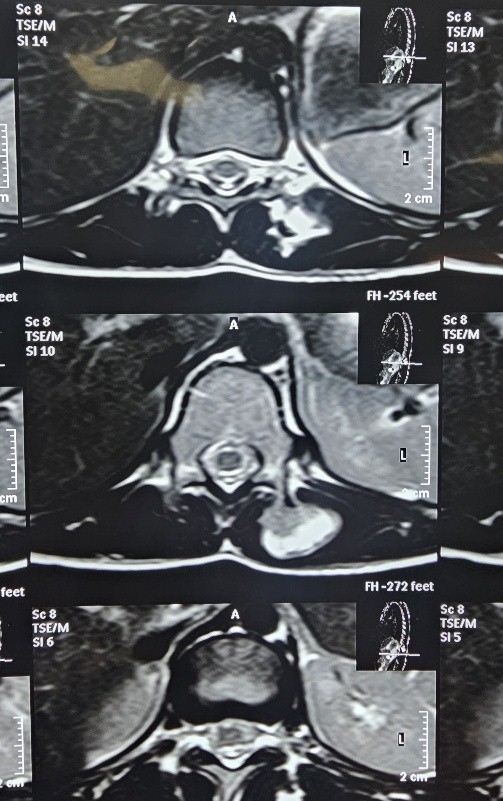
Figure 1:Axial MRI Showing Bony outgrowth
Based on clinic-radiological findings, a provisional diagnosis of osteochondroma arising from D12 vertebrae was made and planned for excisional biopsy. Under general anesthesia, the patient was placed in the prone position (Fig. 2). Around 6–7 cm of midline incision was placed at the D11-D12 region. Deep fascia was cut in the midline in line with the skin incision. Rather than subperiosteal elevation of paraspinal muscle, the tumor was approached through the left paraspinal muscle to remain extra-periosteal while excising the tumor (Fig. 3). En bloc excision of the tumor was done (Fig. 4). The small amount of stock was nibbled off till it felt flat over the lamina. The wound was irrigated and closed in layers. The final subcuticular skin suture was applied for cosmesis (Fig. 5). The patient was mobilized on the next post-operative day.

Figure 2:Prone position

Figure 3: Extraperiosteal Excision of Tumor

Figure 4: Excised Tumor mass

Figure 5: Wound Closure
Histopathology showed mature trabecular bone with a thin hyaline cartilage cap without any undifferentiated cells, confirming the diagnosis of osteochondroma. The patient was followed for 1 year, in which no signs of recurrence were found, and she was carrying out her activities of daily living without any discomfort.
Overall, the predominance of osteochondromas has a male predominance with a male: female ratio of 1.74:1, with around 60% affection for long bones [2]. The incidence of spinal osteochondromas is rare, with the reported incidence in literature ranging from 1 to 4% of all osteochondromas [3,4]. The cervical spine is the most common site to have osteochondroma in the spine and accounts for around 50% cases [5]. The second cervical vertebrae are the most common site, followed by C3 and C6 [6,7,8]. Lin et al. [9], on reviewing 207 articles, have also reported male predominance in the overall incidence of osteochondroma. They have also reported the cervical region (51.8%) to be most commonly involved, followed by lumbar (25%), then thoracic (20.2%), then sacral (8.3%), and coccyx (1.2%). In their series, only two cases of osteochondromas were present at the thoracolumbar junctions. We are reporting a case of osteochondroma in a female patient found at the level of D12 vertebrae, which is an extremely rare finding and worth reporting. The most agreed-upon theory regarding the development of osteochondroma is supposed to be due to abnormal development of the epiphyseal plate or repeated trauma to the epiphyseal plate. The cervical spines have the highest mobility among all the segments and hence have higher chances of trauma to the epiphyseal plate of vertebrae [10]. Further areas having secondary ossification centres, which undergo rapid growth and development, have a higher chance of cartilage malformation leading to the formation of osteochondroma. This all probably explains the higher incidence of osteochondroma in comparison to other vertebral segments. Spinal osteochondromas are found in the appendages of the vertebral body, with literature reporting up to 70.8% cases found in the posterior column of the vertebrae. In our case, the osteochondroma was found to be arising from the mammillary process of the D12 vertebrae. The clinical manifestation due to the tumor depends on its location in the vertebrae, its rate of growth, and the amount of compression on the cord/nerve. The common neural symptoms are those of radiculopathy, sensory disturbances, or features due to myelopathy. There is no consensus about the exact incidence of neural symptoms in spinal osteochondroma [11]. The reported incidence varies from 1% to 30% [1,7,8]. In our case, due to an extra medullary location, the patient presented with discomfort while lying in a supine position. Routine X-ray has a low diagnostic yield for osteochondroma of the spine due to complex orientation, and its value remains for screening purposes only. Computed tomography (CT) scan and MRI examinations offer better visualization of the tumor and its relationship with the cord. CT, on one hand, shows osteochondroma as cortical bone connected with normal bone with continuity of medullary cavity, whereas MRI, on the other hand, also offers the status of cord in relation to the tumor [12]. In our case, the X-ray of the dorsolumbar spine was unremarkable, whereas the MRI showed a tumor arising from the mammillary process with a medullary cavity of the tumor in continuity with the parent bone. We are of the opinion that MRI is a better diagnostic modality for spinal osteochondroma in comparison to CT scan, which is also supported by the study of Lotfinia et al. [2]. Investigations in the form of a CT scan or MRI are not only essential for establishing a diagnosis but also for planning further treatment in the form of surgical excision. The majority of authors have concluded that small osteochondromas growing outside the spinal canal can be managed non-operatively if there are no clinical symptoms. However, large tumors growing outside or encroaching on the canals should be removed surgically [13]. In our case, the tumor was affecting her normal function by causing discomfort when lying supine; hence, it was surgically removed [14].
Osteochondroma of D12 is a rare phenomenon, but it should also be kept as a differential diagnosis while treating patients with unexplained back symptoms in a normal X-ray. The condition needs to be investigated further with an MRI. Surgical excision should be kept reserved for large osteochondromas outside of the neural canal or tumors causing neural symptoms.
Osteochondroma of D12 is a rare phenomenon. Surgical excision should be kept reserved for large osteochondromas outside of the neural canal or tumors causing neural symptoms.
References
- 1. Gille O, Pointillart V, Vital JM. Course of spinal solitary osteochondromas. Spine (Phila Pa 1976) 2005;30:E13-9. [Google Scholar] [PubMed]
- 2. Albrecht S, Crutchfield JS, SeGall GK. On spinal osteochondromas. J Neurosurg 1992;77:247-52. [Google Scholar] [PubMed]
- 3. Gigi R, Kurian BT, Cole A, Fernandes JA. Late presentation of spinal cord compression in hereditary multiple exostosis: Case reports and review of the literature. J Child Orthop 2019;13:463-70. [Google Scholar] [PubMed]
- 4. Rajakulasingam R, Murphy J, Botchu R, James SL. Osteochondromas of the cervical spine-case series and review. J Clin Orthop Trauma 2020;11:905-9. [Google Scholar] [PubMed]
- 5. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar] [PubMed]
- 6. Garg B, Batra S, Dixit V. Solitary anterior osteochondroma of cervical spine: An unusual cause of dysphagia and review of literature. J Clin Orthop Trauma 2018;9 Suppl 2:S5-7. [Google Scholar] [PubMed]
- 7. Raswan US, Bhat AR, Tanki H, Samoon N, Kirmani AR. A solitary osteochondroma of the cervical spine: A case report and review of literature. Childs Nerv Syst 2017;33:1019-22. [Google Scholar] [PubMed]
- 8. Chang DG, Park JB. Osteochondroma arising from the transverse process of the lower cervical spine in an elderly patient. World Neurosurg 2019;130:450-3. [Google Scholar] [PubMed]
- 9. Lin GX, Wu HJ, Chen CM, Rui G, Hu BS. Osteochondroma arising from the inferior articular process of the lumbar spine in a geriatric patient: A case report and literature review. Geriatr Orthop Surg Rehabil 2022;13:21514593211073028. [Google Scholar] [PubMed]
- 10. Fowler J, Takayanagi A, Siddiqi I, Ghanchi H, Siddiqi J, Veeravagu A, et al. Cervical osteochondroma: Surgical planning. Spinal Cord Ser Cases 2020;6:44. [Google Scholar] [PubMed]
- 11. Ganesh S, Jonathan GE, Patel B, Prabhu K. Solitary facet joint osteochondroma of the upper thoracic spine: An unusual cause of cord compression in the pediatric age group. Neurol India 2018;66:555-6. [Google Scholar] [PubMed]
- 12. Kumar R, Kumar S, Vijay T, Verma D. Approach to the management of solitary osteochondroma of the body of the pubis. J Orthop Dis Traumatol 2019;2:58-60. [Google Scholar] [PubMed]
- 13. Du K, Lou Z, Zhang C, Guo P, Chen L, Wang B, et al. Transpedicular excision of a thoracic intraspinal osteochondroma in a patient with hereditary multiple exostoses and brown-séquard syndrome. World Neurosurg 2018;111:94-8. [Google Scholar] [PubMed]
- 14. Akhaddar A, Boucetta M. Solitary osteochondroma of the cervical spine presenting as recurrent torticollis. Pan Afr Med J 2014;17:271. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Osteochondroma Arising from Dorsal Pedicle Causing Compressive Myelopathy
January 1, 2026 Osteochondroma Arising from Dorsal Pedicle Causing Compressive Myelopathy February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases
February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report
February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report