
Three-dimensional computed tomography can accurately diagnose and guide treatment planning for impinged surgical drains in knee arthroplasty patients.
Dr. Ashwani Mudgil, Department of Orthopaedics, Civil Hospital, Ambala Cantt, Haryana, India. E-mail: docashwanimudgil@gmail.com
Introduction: Total knee arthroplasty is one of the most common orthopedic surgeries performed worldwide. As a major surgery, it has its own spectrum of complications, one of which is a retained surgical drain requiring prompt management. While traditional imaging modalities have limitations in localizing retained drain segments, 3D computed tomography (CT) offers enhanced visualization capabilities.
Case Report: We report two cases with retained segments of surgical drains after total knee arthroplasty. In the first case, a 56-year-old female had a retained drain segment that broke after an attempt to remove it. In the second case, a 69-year-old male experienced drain breakage due to impingement between the patella and the femoral component. Both cases were successfully managed using 3D CT for precise localization, enabling minimally invasive retrieval through targeted suture removal rather than extensive wound exploration.
Conclusion: Three-dimensional CT can play a valuable role in managing these complications. It can help accurately mark the site and measure dimensions from the proximal suture line, ultimately enabling a minimally invasive re-exploration.
Keywords: Computed tomography, knee arthroplasty, orthopedic surgery, surgical closed drain.
Total knee arthroplasty is one of the most commonly performed orthopedic surgeries worldwide, with excellent long-term outcomes and cost-effectiveness [1]. These surgeries have increased substantially over the last two decades. One surgical aspect of arthroplasty is the use of surgical drains to prevent hematoma formation and reduce unwanted sequelae. However, every intervention has potential adverse effects, one of which is an entrapped or retained surgical drain.
Entrapment may occur due to several causes, including unintentional suture fixation during wound closure or entrapment between the implant and bony surfaces. Regardless of the cause, it is an unnecessary burden for both the patient and surgeon.
Here, we report two cases of entrapment and retained segments of surgical closed drains in knee arthroplasty and their management using 3D computed tomography (CT).
Case No: 1
A 56-year-old female with Grade IV osteoarthritis of the left knee underwent primary total knee arthroplasty under regional anesthesia (combined spinal epidural anesthesia). The intraoperative period was uneventful, and the patient was hemodynamically stable. At the end of surgery, a closed suction drain (Romovac suction drain, No. 14, Romsons International, Noida, India, Ltd.) was placed intra-articularly toward the lateral gutter under direct visualization. Before wound closure, free movement of the drain was confirmed by gentle traction.
As per institutional protocol, drain removal was attempted after 24 h of surgery. Despite a moderate traction force, the drain could not be withdrawn. Repositioning the knee into flexion was attempted, but this resulted in the drain breakage with retention of the proximal segment. An investigation was undertaken to determine the cause. Post-operative radiographs of the knee failed to clearly demonstrate the retained drain (Fig. 1).
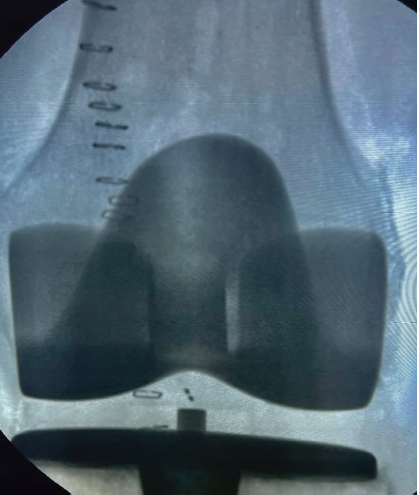
Figure 1: Anteroposterior radiograph of the knee in the post-operative period.
A 3D CT scan was subsequently performed, which precisely localized the retained drain segment lying between the articular surface of the patella and the femoral implant (Fig. 2).
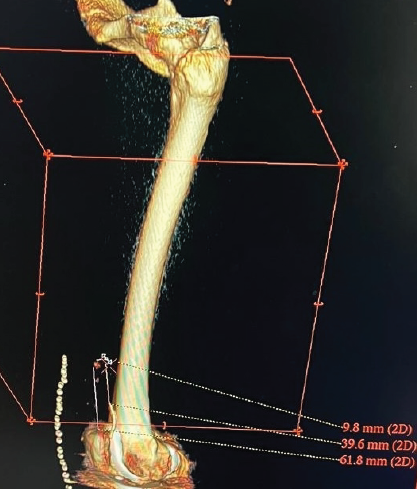
Figure 2: 3D computed tomography scan showing the retained drain segment.
The decision to remove the drain under sedation was made. With the help of the 3D CT scan, the corresponding four stapler sutures were removed. Below that, only one fascial suture was removed, and the retained drain piece was extracted without difficulty. Wound wash was given, and closure was done in layers. The rest of the post-operative period was uneventful, and the patient was discharged in stable condition on the 5th day. On 1- and 3-month follow-up in the outpatient department, the patient had no complaints and demonstrated satisfactory functional outcomes.
Case No: 2
A 69-year-old male with Grade IV osteoarthritis of the right knee underwent primary total knee arthroplasty using an identical surgical technique and drain placement as described above. At 24 h postoperatively, drain removal was attempted with the knee in extension, with gentle traction. The drain broke during removal, leaving the proximal segment retained within the joint. 3D CT scan showed that the retained segment was impinged between the articular surface of the patella and the femoral implant (Fig. 3).
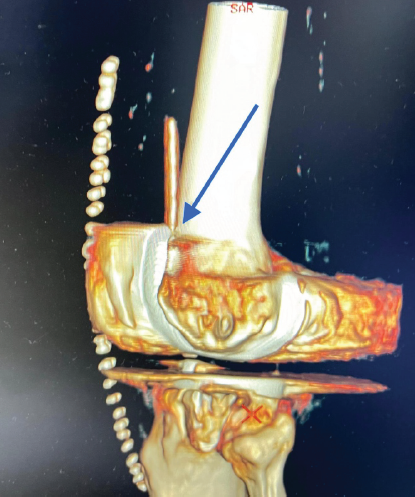
Figure 3: 3D computed tomography scan showing the point of impingement (indicated by blue arrow).
As in the previous case, under sterile precautions, the corresponding sutures and fascial sutures were removed under sedation. The drain was removed through this minimal access approach and closed after wound wash. The rest of the post-operative period was uneventful, and the patient was discharged in stable condition on the 6th day. The patient recovered without complications and reported no issues at subsequent follow-up visits.
Fig. 4 demonstrates the tethered junction points of the retrieved drain segments.

Figure 4: The drain with its broken junction of the retained segment.
Role of 3D CT scan
In both cases, a 3D CT scan was performed to help localize the retained segments. The scan enabled assessment of the distance from the proximal suture line. With these dimensions, the exact location of the retained drain segment was identified. This was immensely helpful in guiding us to the corresponding sutures. Instead of opening all sutures from the proximal or distal end, as documented in the literature, we opened only the four sutures above the drain location. This allowed the removal of the retained segment through a minimally invasive approach. Despite these advantages, 3D CT scan has limitations, including radiation exposure, added cost, and availability at the medical center. These factors need to be weighed against potential benefits.
Total knee arthroplasty is one of the most common orthopedic surgeries performed worldwide. At the end of surgery, the use of a closed surgical drain is commonly practiced among orthopedic surgeons to prevent hematoma formation and reduce post-operative swelling [2]. Unintentional entrapment or retention of part of the surgical drain can lead to numerous complications, including infection, the need for re-exploration, pain, and psychological trauma to the patient [3].
Common causes of drain breakage include entrapment in a closed space between the implant and bony surface, unintentional suturing during wound closure, and soft-tissue incarceration [4]. Suture entrapment can be prevented and identified during primary surgery itself. Most commonly, the drain is kept in the lateral gutter away from the suture line. At the end of closure, the drain is tugged, and smooth movement confirms the absence of entrapment [5].
Ragunanthan et al. documented approaches for dealing with entrapped drains while avoiding surgical intervention [4]. Although free movement of the drain was meticulously checked before wound closure in both of our patients, the drain subsequently migrated and became stuck, leading to breakage. Constant force can push the drain beyond its tensile strength to a breaking point. Various causes of drain breakage have been described, including stretching, weakening by body fluids, manufacturing defects, unintentional suturing creating a weakened junction, and high negative pressure causing strong tissue adherence [6]. Surgical removal is usually the preferred approach to rectify this complication. Sometimes retained drain segments have been left in situ, but this carries risks including pain, mechanical blockage, or foreign body granulation formation [7,8].
Traditional plain radiographs often fail to adequately visualize retained drain segments due to the radiolucent nature of drain materials and the superimposition of anatomic structures. In both our cases, post-operative radiographs could not clearly demonstrate the retained drain segments.
Three-dimensional CT scanning offers several advantages over traditional 2D imaging modalities. Its multiplanar reconstruction capabilities allow visualization of structures from any angle, providing a comprehensive understanding of complex anatomy. This technology eliminates superimposition artifacts common in plain radiographs and offers superior spatial resolution compared to magnetic resonance imaging for bone structures. Mancino et al. emphasized the value of 3D CT scanning for intraoperative navigation in primary total hip arthroplasty [9]. Troiano et al. concluded that 3D CT-based pre-operative planning and intraoperative navigation are a safe procedure without increased incidence of complications [10].
In our cases, 3D CT precisely localized the retained segments and their relationship to surrounding structures. This information was crucial in planning a minimally invasive retrieval approach. Instead of extensive wound exploration with removal of all sutures, we were able to target only the specific area containing the retained drain. This reduced surgical trauma, operative time, and potentially lowered infection risk.
In Case 1, the drain was likely unintentionally sutured, leading to breakage at the weakened junction. Although free gliding movement was ensured before closure, the drain may have been kinked at some level, creating a false sensation of smooth movement. During removal, repositioning the knee to flexion was attempted with moderate, constant force. Extreme force or jerky movements should be avoided. If a patient complains of pain during drain traction, it should be handled carefully, as the drain may be entrapped between anatomical structures.
In Case 2, the drain broke while being removed with the knee in extension. This may have been due to weakening from impingement between the articular surface of the patella and the femoral component, which was confirmed on the 3D CT scan.
The field continues to evolve with advances in imaging technology, including ultra-high resolution CT scanners, dual-energy CT, and artificial intelligence-assisted image reconstruction. These developments promise to further enhance image quality while potentially reducing radiation exposure and acquisition times.
Entrapped or retained segments of surgical closed drains are uncommon complications after knee arthroplasty. Although protocol-based precautions are undertaken to avoid these, patients can still face these complications. Three-dimensional CT may be a valuable adjunct in managing retained drain complications. It can help accurately localize the retained segment and measure distances from the suture line, potentially enabling a more focused, minimally invasive approach. Based on our experience with these two cases, we recommend considering 3D CT when traditional imaging fails to adequately localize retained drain segments, weighing the benefits of precise localization against considerations of radiation exposure, cost, and availability.
Three-dimensional CT can be incorporated into practice to accurately predict the site of drain impingement and compression. It may help avoid extensive wound exploration, reducing the need for more invasive secondary surgery in the post-operative period.
References
- 1. Varacallo MA, Luo TD, Mabrouk A, Johanson NA. Total knee arthroplasty techniques. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/nbk499896 [Google Scholar] [PubMed]
- 2. Maniar RN, Pradhan P, Bhatnagar N, Maniar A, Bidwai R, Bindal P. Role of suction drain after knee arthroplasty in the tranexamic acid era: A randomized controlled study. Clin Orthop Surg 2019;11:73-81. [Google Scholar] [PubMed]
- 3. Laratta JL, Lombardi JM, Shillingford JN, Grosso MJ, Lehman RA, Lenke LG, et al. Optimal management of tethered surgical drains: A cadaver study. J Am Acad Orthop Surg 2019;27:129-35. [Google Scholar] [PubMed]
- 4. Ragunanthan N, Ibad Sha I. Tethered drain after total knee replacement – Two different case scenarios and review of literature. J Orthop Rep 2022;1:100048. [Google Scholar] [PubMed]
- 5. Jaafar S, Vigdorchik J, Markel DC. Drain technique in elective total joint arthroplasty. Orthopedics 2014;37:37-9. [Google Scholar] [PubMed]
- 6. Gheorghiu D, Chris C, Teanby D. Retained surgical drain after total knee arthroplasty: An eight-year follow-up: A case report. JBJS Case Connect 2015;5:e63. [Google Scholar] [PubMed]
- 7. Widman J, Jacobsson H, Larsson SA, Isacson J. No effect of drains on the postoperative hematoma volume in hip replacement surgery: A randomized study using scintigraphy. Acta Orthop Scand 2002;73:625-9. [Google Scholar] [PubMed]
- 8. Cox JS, Friess D. Retained surgical drains in orthopedics: Two case reports and a review of the literature. Case Rep Orthop 2017;2017:8194571. [Google Scholar] [PubMed]
- 9. Mancino F, Fontalis A, Magan A, Plastow R, Haddad FS. The value of computed tomography scan in three-dimensional planning and intraoperative navigation in primary total hip arthroplasty. Hip Pelvis 2024;36:26-36. [Google Scholar] [PubMed]
- 10. Troiano E, Masini A, Colasanti GB, Drago C, Giannotti S, Mondanelli N. 3D CT-based preoperative planning and intraoperative navigation in reverse shoulder arthroplasty: Early clinical outcomes. Medicina (Kaunas) 2025;61:749. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review
February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review February 1, 2026 Robotic-Assisted Dynamic Intraoperative Assessment of Coronal Plane Stability Across the Range of Motion During Total Knee Arthroplasty
February 1, 2026 Robotic-Assisted Dynamic Intraoperative Assessment of Coronal Plane Stability Across the Range of Motion During Total Knee Arthroplasty January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review
January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis
December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis