
While all-suture fixation for very distal, unstable lateral clavicle fractures with poor bone stock is an appealing option, it could, however, lead to an increased risk of refracture.
Dr. Joël Locher, Department of Orthopaedic and Trauma Surgery, Zuger Kantonsspital, Switzerland. E-mail: joel.locher@zgks.ch
Abstract
Introduction: Distal clavicle fractures account for 10–30% of all clavicle fractures, with a considerable proportion being displaced. Although both conservative and various surgical approaches can lead to favorable outcomes and functional results, the optimal treatment strategy remains a subject of debate. All-suture techniques are becoming increasingly popular due to advantages such as enhanced torsional and axial stability and reduced implant-associated morbidity. Nonetheless, potential consequences, such as the effects of bone remodeling issues and refracture predisposition, remain inadequately investigated.
Case Report: We report the case of a 25-year-old athletic male who sustained a displaced, very distal clavicle fracture with poor bone stock. This case highlights a previously unreported complication of all-suture osteosynthesis: the development of a bone groove, likely caused by the recurrent “sawing” motion of the sutures. Although the initial fracture healed appropriately, a subsequent injury – a fall while skiing – resulted in a new fracture at the site of the bone groove. Nonetheless, as the initial fracture had consolidated well and bone stock in the lateral fragment was adequate, plate osteosynthesis was successfully performed for the second fracture, with no complications observed.
Conclusion: All-suture stabilization is a viable option for dislocated distal clavicle fractures with poor bone stock, offering good stability and fewer implant-related issues. However, this case highlights a potential complication, bone groove formation at the augmentation site, possibly predisposing to refracture. Suture material choice may influence this risk, warranting further investigation.
Keywords: All suture, osteosynthesis, lateral clavicle fracture, bone groove, refracture.
Distal clavicle fractures account for 10–30% of all clavicle fractures, with half being dislocated [1]. Standard radiographs are commonly used for identification and classification, with the modified Neer classification [2] and the Jaeger and Breitner classification [3] being the most widely applied. Other diagnostic methods, such as computed tomography (CT) scans and magnetic resonance imaging, have also been proposed for classification [4]; however, their use is not standardized and may delay treatment. There is no consensus on the optimal treatment, as both conservative and surgical approaches have demonstrated good functional outcomes, even in displaced unstable fractures [1,4,5]. However, a non-union rate of up to 31% has been reported for conservative treatment, although only half of these were symptomatic (6). In addition, surgical treatment has been associated with a significant rate of hardware-related complications [6,7]. Several surgical techniques have been described, generally categorized into two main groups: rigid internal fixation (including T-plates, locking plates, hook plates, coracoclavicular or acromioclavicular stabilization with screws or Kirschner-wire (K-wire), and intramedullary fixation) and flexible osteosynthesis with or without arthroscopic assistance (such as tension band wiring, sutures, bone anchors, tapes, cortical buttons, and synthetic grafts or allografts), as well as various hybrid approaches [8]. Hook plates have recently been associated with lower functional scores compared to locking plates [6]. In very lateral and comminuted fractures, achieving adequate bone purchase in the lateral fragment can be challenging, potentially leading to screw pull-out. Apposition of fragments alone has been proposed as sufficient for fracture healing, but achieving proper repositioning in both the superoinferior and anteroposterior planes can be difficult [9]. Acromioclavicular transfixation with K-wires has also been suggested; however, it is associated with up to 29% of hardware complications, such as K-wire breakage or migration [10]. We report a case of reosteosynthesis in a 25-year-old athletic male who sustained a refracture at the site of a previously healed distal clavicle fracture. The initial fracture, caused by a mountain biking accident, was treated with an arthroscopic all-suture technique, leading to satisfactory healing but the development of a bone groove. Following a high-energy skiing accident 24 weeks later, he sustained a refracture at the groove site, which was successfully treated with locking plate osteosynthesis. The patient was informed that data from this case would be submitted for publication, and consent was obtained. No funding was received for this work.
A 25-year-old, otherwise healthy and physically active male was riding a mountain bike at high speed when he abruptly applied the brakes, resulting in a forward ejection over the handlebars and direct impact on his right shoulder. He presented to the emergency department with pain and deformity of the right clavicle.
Clinical findings
Hematoma and deformity were observed at the right distal clavicle. The skin was intact and not under tension. Movements below the horizontal plane were possible but painful. Sensation and perfusion of the arm were intact. No pain was elicited upon palpation of the thorax. He was unable to hold weight with the arm, and lifting of the arm over the horizontal in the frontal and lateral direction was particularly painful. The Body-Cross-Adduction Test was painful. No other pain to pressure at the shoulder was noted. All other joints at the arm showed a free range of motion. There were no signs or complaints of instability.
Diagnostic assessment
Conventional radiographs and a CT scan revealed a very distal, multifragmentary, and dislocated clavicle fracture (Fig. 1). Due to the highly comminuted distal configuration, the lateral bone stock was severely compromised. The fracture was classified as Jäger-Breitner Type IIa and Neer Type V. No further associated injuries were identified.
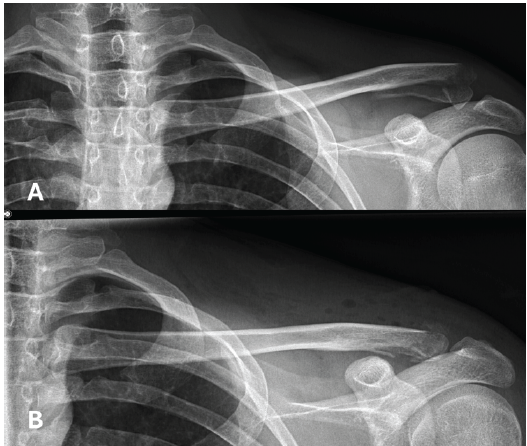
Figure 1: A: X-ray showing a dislocated, multifragmentary lateral clavicle fracture after the first accident. B: X-ray imaging performed one day postoperatively.
Therapeutic intervention
Since the patient desired an early return to sports activities and given the dislocation of the fracture, surgical treatment was chosen. Due to the multifragmentary nature of the fracture and poor bone stock, osteosynthesis with a locking plate was avoided due to the risk of screw pull-out. An arthroscopic all-suture technique was chosen, incorporating a double-loop coracoclavicular stabilization and a figure-of-0 cerclage between the medial fragment and the acromion. Surgery was performed with the patient in the beach-chair position, using a Trimano® arm holder under general anesthesia. A diagnostic glenohumeral and subacromial arthroscopy was conducted to exclude associated injuries. Under arthroscopic visualization, the undersurface of the coracoid was prepared for optimal exposure. A small oblique incision of 4 cm was made from the posterolateral distal clavicle toward the coracoid process. The deltoid insertion was partially detached from the clavicle, and the fracture site was exposed. The fracture was reduced and temporarily stabilized using a K-wire from the lateral acromion to the medial clavicle fragment. Two DYNATAPE® (Johnson and Johnson) sutures tapes were arthroscopically shuttled from the dorsal clavicle, beneath the coracoid, and to the ventral clavicle, then secured on top of the medial clavicle fragment, in the manner of a loop augmentation.
A 3 mm hole was drilled dorsolaterally to anteromedially through the acromion. The end of a secured DYNATAPE® suture tape was shuttled in a figure-of-0 configuration through these holes and knotted on top of the clavicle, creating a cerclage between the medial fragment and the acromion to achieve a horizontal stability. Reduction was confirmed visually and fluoroscopically.
The superior trapezo-deltopectoral fascia was reconstructed using No. 2 Vicryl sutures (Ethicon, Somerville, NJ, USA). The wound was closed and dressed according to standard post-operative care. Postoperatively, the patient was immobilized in a sling for 6 weeks. Active wrist and elbow motion was permitted, along with progressive passive shoulder range of motion in the scapular plane. After 6 weeks, active range of motion was allowed, followed by progressive strengthening, with full return to sports activities at 3 months.
Follow-up and complication
No perioperative complications were reported, and the wound healed appropriately. At the first follow-up X-ray (Fig. 2), taken 6 weeks postoperatively, a bone groove was observed in the clavicle at the level of the coracoclavicular loop augmentation. This groove became more pronounced and widened on the 3-month follow-up X-ray. However, fracture healing remained satisfactory, and the patient achieved full restoration of shoulder function without any reported pain or disabilities. Clinically, he demonstrated a highly satisfactory outcome with no limitations in daily activities.

Figure 2: X-rays at 3 months post-operative, showing good bone healing and the formation of a bone groove at the level of the coracoclavicular loop augmentation.
Physiotherapy was carried out to progressively strengthen the shoulder muscles and improve scapular stabilization. Palpation of the clavicle and acromioclavicular joint elicited no pain, and the cross-body test was negative. The patient had regained full strength compared to the uninjured side and had fully returned to sports. No clinical signs of instability were observed.
At 24 weeks postoperatively, the patient sustained a clavicle refracture at the site of the previous bone groove following a high-energy skiing accident (Figs. 3 and 4).
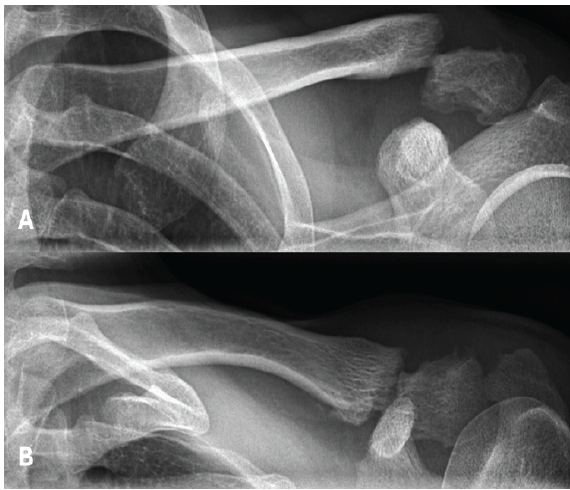
Figure 3: X-rays showing a refracture after a skiing accident, occurring 3.5 months after the initial all-suture osteosynthesis.
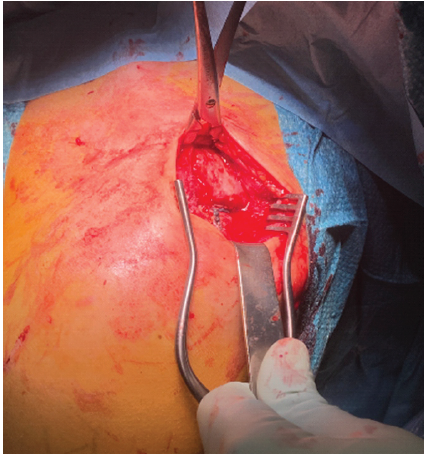
Figure 4: Intraoperative images of the DynaTape® system and the fracture at the site of the bone groove during plate osteosynthesis.
Given the improved bone stock of the lateral fragment, locking plate osteosynthesis was chosen as treatment. Coracoclavicular reconstruction was deemed unnecessary, as the lateral fragment remained stable. Both the surgery and post-operative course were uneventful through the 3-month follow-up, and the fracture at the site of the bone groove had nearly completely healed (Fig. 5).
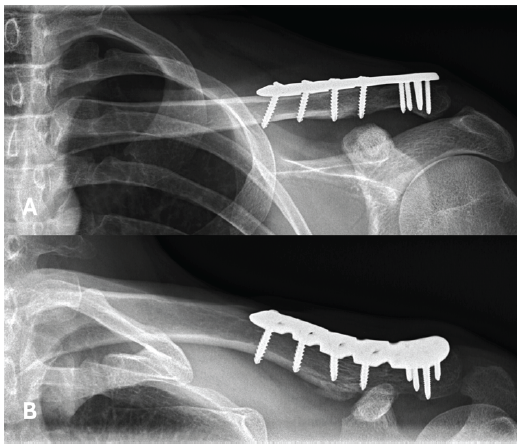
Figure 5: X-rays at the final follow-up, 3 months after plate osteosynthesis, showing good healing of the fracture.
The management of dislocated distal clavicle fractures remains a topic of debate, with multiple surgical approaches available [10]. In cases of highly distal fractures with inadequate bone stock, locking plates may provide insufficient fixation due to limited bone engagement, increasing the risk of screw pull-out [6]. In such scenarios, all-suture stabilization offers theoretical advantages, including adequate rotational and axial stability – even when lateral bone stock is compromised. Furthermore, it may reduce the need for implant removal, as these implants are much less prominent. In the present case, we observed the formation of a bone groove at the coracoclavicular augmentation site following all-suture stabilization, likely caused by repetitive motion producing a “sawing” effect. Although clinically asymptomatic, this groove may have acted as a predisposed site for refracture of the clavicle. This phenomenon is an up-to-date not described complication of an all-suture osteosynthesis in distal clavicle fracture. A parallel can be drawn to the well-documented phenomenon of tunnel widening in coracoclavicular stabilization techniques, such as button fixation, where the clavicle is drilled, and sutures or tapes are passed through it. In such cases, the phenomenon is associated with loss of reduction [11] and in severe case with fracture of the clavicle [12]. Furthermore, the selection of suture material might be important. Biomechanical research has shown that flat-braided sutures, such SutureTape®, enhance rigidity at the fracture site with reduced creep, whereas alternative sutures, such as Ethibond®, exhibit superior elasticity, more closely resembling ligament characteristics [13]. In this case, we utilized DYNATAPE™, a dynamic, high-strength non-resorbable tape with a salt-infused silicone core designed to attract moisture in fluid-rich environments, thereby enhancing tissue approximation. According to the manufacturer, DYNATAPE™’s self-tensioning mechanism provides sustained compression for at least 12 weeks, making it well suited for coracoclavicular stabilization by supporting prolonged healing. Compared to other suture tapes such as FiberTape®, DYNATAPE has demonstrated 55% less tissue abrasiveness, potentially reducing local tissue irritation and damage. We hypothesize that this may also result in less bone irritation; however, a bone groove was still observed [14]. Non-resorbable suture tapes remain the standard for all-suture stabilization of lateral clavicle fractures due to their superior mechanical strength and durability. While the development of high-strength resorbable tapes is appealing and could potentially mitigate the “sawing” effect observed in this case, achieving sufficient long-term mechanical stability in high-load applications while maintaining resorbable properties remains a significant challenge.
All-suture stabilization represents a viable option for managing dislocated distal clavicle fractures with compromised bone stock, offering advantages such as enhanced rotational and axial stability, elimination of the need for hardware removal, and reduced implant-related complications. However, this case highlights a notable risk associated with the technique: the development of a bone groove at the coracoclavicular augmentation site, which may predispose to subsequent fractures. The choice of suture material appears to influence these outcomes. Future studies are warranted to identify the optimal suture materials, assess the clinical significance of post-operative bone grooves, and evaluate the risk of refracture to refine indications and optimize techniques for all-suture fixation.
All-suture stabilization offers a viable option for dislocated distal clavicle fractures with poor bone stock, but may risk bone groove formation and refracture. Suture material choice could influence this complication and warrants further study.
References
- 1. Kihlström C, Hailer NP, Wolf O. Surgical and non-surgical treatment for fully displaced lateral clavicle fractures have similar outcomes: An observational register study of 113 patients. Injury 2024;55:111422. [Google Scholar] [PubMed]
- 2. Stenson J, Baker W. Classifications in brief: The modified neer classification for distal-third clavicle fractures. Clin Orthop Relat Res 2021;479:205-9. [Google Scholar] [PubMed]
- 3. Jäger M, Breitner S. Therapy related classification of lateral clavicular fracture. Unfallheilkunde 1984;87:467-73. [Google Scholar] [PubMed]
- 4. Sharma V, Modi A, Armstrong A, Pandey R, Sharma D, Singh H. The management of distal clavicle fractures – a survey of UK shoulder and elbow surgeons. Cureus 2021;13:e17305. [Google Scholar] [PubMed]
- 5. Raval P, See A, Singh HP, Distal Third Clavicle Collaborative. Distal third clavicle fractures: A nationwide trainee-led collaborative review of current practice. Bone Jt Open 2022;3:953-9. [Google Scholar] [PubMed]
- 6. Uittenbogaard SJ, Van Es LJ, Den Haan C, Van Deurzen DF, Van Den Bekerom MP. Outcomes, union rate, and complications after operative and nonoperative treatments of neer type II distal clavicle fractures: A systematic review and meta-analysis of 2284 patients. Am J Sports Med 2023;51:534-44. [Google Scholar] [PubMed]
- 7. Gutman MJ, Joyce CD, Patel MS, Lazarus MD, Horneff JG. Outcomes following different fixation strategies of Neer type IIB distal clavicle fractures. Arch Bone Jt Surg 2022;10:160-5. [Google Scholar] [PubMed]
- 8. Kuner E, Beeres FJ, Babst R, Schoeniger R. Which lateral clavicle fractures can be treated by an arthroscopic-assisted endobutton procedure? An analysis of risk factors. Arch Orthop Trauma Surg 2019;139:331-7. [Google Scholar] [PubMed]
- 9. Navarro RA. In my experience… the perplexing problem of distal clavicle fractures. J Orthop Exp Innov. 2025;6:2. [Google Scholar] [PubMed]
- 10. Panagopoulos A, Solou K, Nicolaides M, Triantafyllopoulos IK, Kouzelis A, Kokkalis ZT. Coracoclavicular fixation techniques for Neer IIb and “extralateral” fractures of the distal clavicle: A systematic review. JSES Rev Rep Tech 2024;4:676-83. [Google Scholar] [PubMed]
- 11. Velasquez Garcia A, Franco Abache A, Ingala Martini L. Clavicular tunnel widening after coracoclavicular stabilization surgery: A systematic review and meta-analysis. J Shoulder Elbow Surg 2024;33:738-55. [Google Scholar] [PubMed]
- 12. Waterman BR. Editorial commentary: Tunnel widening and loss of reduction may be inevitable after acromioclavicular stabilization with cortical suspensory devices whether inset (top hats) or onlay (buttons). Arthroscopy 2023;39:2281-2. [Google Scholar] [PubMed]
- 13. Cunningham G, Almeida LA, Gauthier M. All-suture technique for fixation of unstable displaced distal clavicle fracture. JSES Rev Rep Tech 2022;2:168-73. [Google Scholar] [PubMed]
- 14. Synthes D. DYNA Suture Technology Value Analysis Brief. Mitek Sports Medicine (DePuy Synthes); 2023. Available from: Johnson & Johnson MedTech website: https://www.jnjmedtech.com/system/files/pdf/162479-230211%20DSUS%20DYNA%20Suture%20Technology%20Value%20Brief_V2%20030123%203.pdf [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?
December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary? October 1, 2025 Osteosynthesis in Iatrogenic Femoral Neck Fracture following Irreducible Posterior Hip Fracture Dislocation in an Elderly Patient: A Case Report and Literature Review
October 1, 2025 Osteosynthesis in Iatrogenic Femoral Neck Fracture following Irreducible Posterior Hip Fracture Dislocation in an Elderly Patient: A Case Report and Literature Review October 1, 2024 Bicondylar Tibial Plateau Fracture in Below-Knee Amputation: A Rare Injury Case Report
October 1, 2024 Bicondylar Tibial Plateau Fracture in Below-Knee Amputation: A Rare Injury Case Report