
Single-stage autologous minced cartilage combined with PRP scaffold offers a promising biologic and cost-effective treatment for adolescent patellar osteochondral defects, enabling functional recovery and a less morbid alternative to traditional two-stage procedures.
Dr. Anand Raj Rajendrababu, Department of Orthopaedics, Kasaragod Institute of Medical Sciences, Kasaragod, Kerala, India. E-mail: mail.anandrajr@gmail.com
Abstract
Introduction: Osteochondral defects of the patella in pediatric patients are rare but clinically significant due to pain, mechanical symptoms, and potential long-term sequelae. Traditional two-stage approaches, such as autologous chondrocyte implantation, are often avoided in younger patients due to surgical burden and cost. This case report presents a single-stage biologic cartilage repair using autologous minced cartilage and a biologic scaffold (AutoCart, Arthrex) in a 14-year-old male with a symptomatic osteochondral defect in the patella.
Case Report: The technique involves arthroscopic harvest of autologous minced cartilage, intra-operative preparation of platelet-rich plasma (PRP), and application of a cartilage-PRP-BioCartilage matrix. Cancellous bone graft was also added in this case due to the large size of the defect.
Conclusion: At 6 months post-operative, the patient was asymptomatic, had returned to full activity, and magnetic resonance imaging confirmed excellent defect filling with no complications.
Keywords: Osteochondral defect, patella, autologous minced cartilage, adolescent.
Osteochondral defects (OCD) of the patella in skeletally immature patients are diagnostic and therapeutic challenges. These defects, often traumatic or idiopathic, can lead to progressive pain and early degeneration if untreated [1]. Traditional management includes microfracture, osteochondral autografts, and autologous chondrocyte implantation (ACI). While ACI has shown promising outcomes in patella-femoral lesions [2,3,4], its use in young patients is limited due to the two-staged nature, higher cost, and delayed recovery. Emerging single-stage, biologically augmented techniques utilizing minced autologous cartilage, platelet-rich plasma (PRP), and cartilage scaffolds offer an attractive alternative [5,6,7]. This case illustrates the application of such a technique (AutoCart, Arthrex) in an adolescent with an osteochondral patellar lesion.
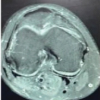
A 14-year-old healthy, right-hand dominant male football player presented with a 9-month history of anterior knee pain on the right side. Pain was insidious in onset, worsened by stairs, squatting, and prolonged activity. No prior trauma or instability was reported. Mild effusion, positive patellar grind test, and crepitus were observed on physical examination, along with tenderness on the lateral facet of the patella. X-ray and computed tomography scan of the knee showed a smooth osteochondral defect in the lateral facet of the patella (Figs. 1 and 2). Magnetic resonance imaging (MRI) revealed a focal 14 × 12 mm osteochondral defect along the superior pole of the right patella on the lateral facet with >15 mm depth (Fig. 3). There were no signs of instability or ligamentous injury. Initial treatment consisted of physical therapy, activity modification, and NSAIDs for 3 months. Persistent symptoms prompted surgical management.
Surgical technique
Preparation
After a round of diagnostic arthroscopy (Fig. 4a) confirming the diagnosis and loose body removal, autologous minced cartilage, approximately 200 mg, was harvested arthroscopically from a non-weight-bearing area of the lateral femoral condyle and trochlea using an arthroscopic shaver. Simultaneously, nearly 60 mL of the patient’s blood was drawn and processed intraoperatively to isolate PRP.
Graft preparation
The cartilage was minced using a sterile shaver (GraftNet system) and mixed with micronized cartilage scaffold (BioCartilage) and autologous PRP to form a cohesive paste.
Application
The undersurface of the patella cannot be treated arthroscopically by this technique. Hence, an open procedure was carried out. A lateral parapatellar incision was made approximately 10 cm long and dissected by the lateral parapatellar approach. The patella was everted medially, and the large osteochondral defect was visualized (Fig. 4b).
- Cancellous bone graft obtained from the non-weight-bearing area of the lateral femoral condyle
- Defect site was debrided to stable cartilage margins, and bone was prepared using a curette to create a stable bed (Fig. 4c)
- Cancellous bone graft applied (Fig. 4d), followed by the biologic paste (Fig. 4e) to fill the defect and contour flush with the surrounding cartilage surface (Fig. 4f)
- Fibrin glue was applied to secure the construct (Fig. 5)
- The knee was held in extension post-application to ensure adhesion during the initial polymerization
- The knee was taken through a full range of movement to make the graft contoured with the surface of the patella.
The immediate post-operative period involved a hinged knee brace allowing flexion up to 30° flexion in the first 2 weeks, followed by progressive increase in range of motion (ROM) up to 90° in the 1st month; progressive weight bearing was allowed as tolerated. Return to sports training at 4 months, full return to sports at 6 months.
The patient achieved pain-free walking at 2 months; almost full ROM and returned to football at 6 months (Fig. 6). IKDC pediatric increased from 52 (pre-operative) to 91 (12 months post-operative); KOOS-Child Sports subscore improved from 60 to 95. MRI findings (Fig. 7) at 6 months postoperatively showed a near-complete defect filling with well-defined cartilage of uniform signal intensity, nearly 3 mm thick, and likely to be hyaline. Minimal subchondral edema and cortical irregularity were noted, but without any unstable osteochondral fragments. No hypertrophy or delamination. No complications such as infection, arthrofibrosis, or donor site morbidity.
This case supports the viability of biologic, single-stage cartilage repair techniques in adolescents, particularly for patellar OCD. Compared to traditional matrix-induced autologous chondrocyte implantation or osteochondral autograft transfer system procedures [2,3], this approach avoids the need for multiple surgeries, preserves tissue, and leverages the high healing potential in young individuals [6]. A similar technique was described by Farr and Yao using BioCartilage and PRP for femoral condyle lesions [5], but data in adolescents and for patellar defects remain limited. Recent reports on AutoCart demonstrate promising mid-term results with simplified logistics and similar efficacy to staged ACI [7,8,9].
Limitations
Single-patient case study, lack of second-look arthroscopy or histology, and no long-term data beyond 18 months (Table 1 and 2).
Considerations
The regenerative environment in adolescents may enhance outcomes with biologic scaffolds. While long-term outcomes remain under investigation, early results support the feasibility of autologous minced cartilage repair for medium-sized patellar OCDs.
Single-stage autologous cartilage repair using minced cartilage, PRP, and scaffold represents a promising strategy for managing OCD in the adolescent patella. It provides functional improvement, radiographic healing, and high patient satisfaction with low morbidity.
Single-stage autologous minced cartilage repair combined with platelet-rich plasma scaffold is a promising and effective treatment for adolescent patellar osteochondral defects, offering functional improvement, radiographic healing, and high satisfaction with low morbidity, whereas avoiding the complexity and cost of traditional two-stage procedures.
References
- 1. Mithoefer K, Williams RJ 3rd, Warren RF, Potter HG, Spock CR, Jones EC, et al. Chondral resurfacing of articular cartilage defects in the knee with the microfracture technique. Surgical technique. J Bone Joint Surg Am 2006;88 Suppl 1:294-304. [Google Scholar] [PubMed]
- 2. Minas T, Chiu R. Autologous chondrocyte implantation. Am J Knee Surg 2000;13:41-50. [Google Scholar] [PubMed]
- 3. Gudas R, Gudaite A, Pocius A, Gudiene A, Cekanauskas E, Monastyreckiene E, et al. Ten-year follow-up of a prospective, randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint of athletes. Am J Sports Med 2012;40:2499-508. [Google Scholar] [PubMed]
- 4. Ebert JR, Fallon M, Ackland TR, Wood DJ. Outcomes of autologous chondrocyte implantation in adolescent vs. Adult patients. Am J Sports Med 2018;46:62-9. [Google Scholar] [PubMed]
- 5. Farr J, Yao JQ. Chondral defect repair using minced cartilage autograft: A prospective case series. Knee 2011;18:361-5. [Google Scholar] [PubMed]
- 6. Bonasia DE, Marmotti A, Mattia S, et al. Adolescent osteochondral injuries: New perspectives in cartilage repair. J Exp Orthop 2016;3:5. [Google Scholar] [PubMed]
- 7. Gracitelli GC, Meric G, Pulido PA, et al. Autologous minced cartilage repair technique for chondral lesions: A systematic review. Cartilage 2021;13 1 Suppl:383S-93. [Google Scholar] [PubMed]
- 8. Schneider S, Ossendorff R, Walter SG, Berger M, Endler C, Kaiser R, et al. Arthroscopic autologous minced cartilage implantation of cartilage defects in the knee: A 2-year follow-up of 62 patients. Orthop J Sports Med 2024;12:23259671241297970. [Google Scholar] [PubMed]
- 9. Schneider S, Linnhoff D, Ilg A, Salzmann GM, Ossendorff R, Holz J. Comparison of three different techniques for the treatment of cartilage lesions-matrix-induced autologous chondrocyte implantation (MACI) versus autologous matrix-induced chondrogenesis (AMIC) and arthroscopic minced cartilage-a 2-year follow-up on patient-reported pain and functional outcomes. J Clin Med 2025;14:2194. [Google Scholar] [PubMed]
- 10. Levinson C, Cavalli E, Sindi DM, Kessel B, Zenobi-Wong M, Preiss S, et al. Chondrocytes from device-minced articular cartilage show potent outgrowth into fibrin and collagen hydrogels. Orthop J Sports Med 2019;7:2325967119867618. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 A Case of In Situ Fixation of Large Lateral Condyle Femur Osteochondral Defect Secondary to Trauma in a Young Male – A Case Report
July 1, 2026 A Case of In Situ Fixation of Large Lateral Condyle Femur Osteochondral Defect Secondary to Trauma in a Young Male – A Case Report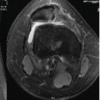 June 1, 2026 Arthroscopic-assisted Suture-based Fixation of Patellar Osteochondral Fractures using the DG-lock Suturing: A Novel Technique
June 1, 2026 Arthroscopic-assisted Suture-based Fixation of Patellar Osteochondral Fractures using the DG-lock Suturing: A Novel Technique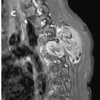 June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report
June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report
May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report