
This case report aims to outline the successful management of an extremely rare case of dislocation of the second to fifth metacarpal without dislocation.
Dr. Omprakash Suthar, Department of Orthopaedics, B.J Medical College and Sassoon General Hospital, Pune, Maharashtra, India. E-mail: omprakashsuthar510@gmail.com
Abstract
Introduction: Carpometacarpal (CMC) joint dislocations represent <1% of all injuries to the hand and wrist regions. Up to 70% of CMC dislocations are missed or misdiagnosed due to severe swelling and overlapping of bones on the radiograph of the wrist.
Case Report: We report the case of a 36-year-old male patient, following a road traffic accident, who complained of pain and swelling in his left hand. On plain radiographs, 2nd–5th CMC joints dislocation without any fracture was found, confirmed on computed tomography scan. Closed reduction with manual traction and slab application was attempted, but it was unsuccessful as it was precarious. The patient was then taken up for surgery. Third CMC joint reduction to its articulation with the capitate with a retrograde K-wire remains the cornerstone for achieving the reduction of the remaining CMC joints. Once that was achieved, the 2nd, 4th, and 5th CMC joint reduction was done and fixed with K-wires. An additional intermetacarpal wire from 5th to 4th was used for extra stability for the highly mobile 4th and 5th CMC joints. Dynamic fluoroscopy showed stable fixation and reduction. K-wires were removed after 6 weeks, and physiotherapy was started.
Conclusion: At the 1-year follow-up, the patient showed stable joints with good hand grip and range of motion (ROM). Hence, careful hand examination and radiographic assessment are necessary to avoid missing the diagnosis. Anatomic reduction and fixation with K-wires done at the earliest is the treatment of choice.
Keywords: Carpometacarpal dislocation, multiple, 2nd–5th.
Carpometacarpal (CMC) joint dislocations without fractures represent <1% of all injuries to the hand and wrist [1]. These dislocations occur in all four ulnar digits without a fracture, making it an even rarer entity. Up to 70% of these CMC dislocations are missed initially due to severe swelling over the dorsum of the hand masking the obvious hump deformity and due to overlapping of the bones on the radiograph [2]. Dislocations of the finger CMC joints are usually high-energy injuries commonly seen in boxers and motorcyclists [3]. Diagnosis requires a high index of suspicion, thorough clinical examination, and appropriate radiography [4]. Most of the cases reported include a single CMC joint dislocation. Delay in the treatment of CMC dislocations results in poor functional outcomes and chronic residual pain.
A 36-year-old manual laborer presented to a tertiary care hospital with gross swelling over the dorsum of the left hand following a fall from a scooter (Fig. 1).
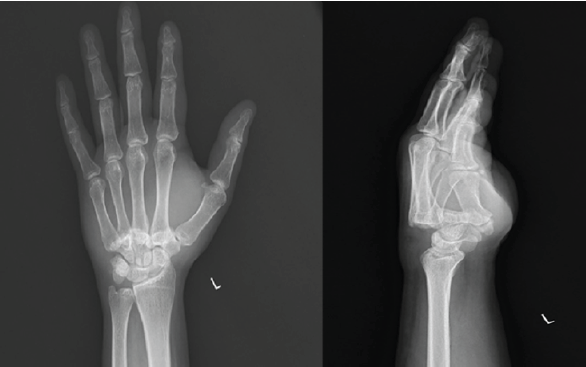
Figure 1: Pre-operative radiographs showing dorsal dislocation of the 2nd–5th metacarpals. Overlapping of the metacarpals over the carpal bones with loss of parallelism and “M” lines seen over the posteroanterior radiograph.
He was managed with analgesics, a crepe bandage, and limb elevation initially for 2 days before reporting to the hospital. Plain radiographs of the left-hand anteroposterior and lateral views revealed dorsal CMC dislocations of all four fingers of the ulnar side of the left hand (Fig. 2). An oblique view of the left hand was taken to confirm the diagnosis. A 3D computed tomography (CT) scan was done to rule out fracture-dislocations (Fig. 3).

Figure 2: Clinical photo showing swelling over the dorsum of the hand, which is masking the hump deformity present at the base of the metacarpals.

Figure 3: Representative 3D computed tomography scan showing dislocation without any fractures.
Closed reduction with manual traction and slab application was attempted, but it was unsuccessful as it was highly unstable. The patient was then taken up for surgery. Third CMC joint reduction to its articulation with the capitate was done and fixed with a retrograde K-wire. Once that was achieved, the 2nd, 4th, and 5th CMC joint reduction was done and fixed with K-wires. An additional intermetacarpal wire from 5th to 4th was inserted for extra stability for the highly mobile 4th and 5th CMC joints (Fig. 4).
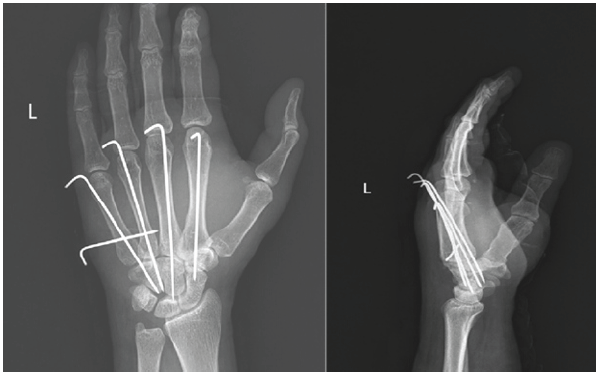
Figure 4: Immediate post-operative radiographs after anatomical reduction of the carpometacarpal joints and K-wire fixation.
Dynamic fluoroscopy showed stable fixation and reduction. Postoperatively, a cock-up splint was applied, and immobilization was continued for 6 weeks. K-wires were removed after 6 weeks. Satisfactory reduction was maintained on re-examination after 6 weeks following cast removal (Fig. 5).

Figure 5: A series of photographs showing radiographs and clinical pictures at 6 weeks when the K-wires were removed. The patient had no to very little movement at the carpometacarpal joints at this stage.
Physiotherapy was started 6 weeks postoperatively after K-wire removal with active and passive mobilization of the wrist joint, metacarpophalangeal joints, and proximal and distal interphalangeal joints of fingers, to achieve good functional recovery. Full range of motion of the hand was achieved, showing a good result at 1-year follow-up (Fig. 6).
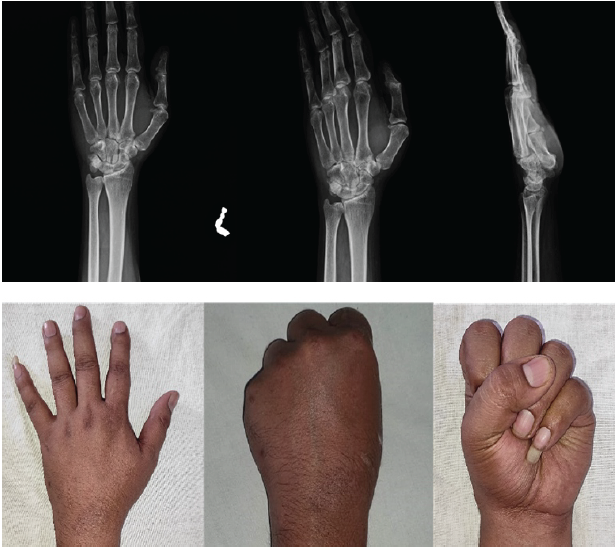
Figure 6: A series of photographs showing the radiographs and excellent clinical outcome of the patient at 1-year follow-up.
CMC joints are saddle joints that are stabilized by volar and dorsal ligaments, transverse metacarpal ligaments, long flexor and extensor tendons, and intrinsic muscles of the hand [1]. Dorsal ligaments are stronger than volar ligaments. Furthermore, ulnar-sided CMC joints are more mobile than radial CMC joints. It is, however, generally accepted that the range of motion in the 2nd through 5th CMC joints increases from the radial to the ulnar side of the hand: The 2nd joint is essentially immobile, whereas the 5th joint simultaneously flexes and adducts. The flexion-extension motion ranges from 1° to 3° for the 2nd and 3rd CMC joints, 10–15° for the 4th CMC joint, and 15–30° for the 5th CMC joint [5].
CMC joint dislocations can be classified based on the direction in which the metacarpal dislocates in relation to the carpal bones into three types: Dorsal, volar [6], and divergent. “Divergent variant” of multiple CMC dislocations in which divergence is defined as volar dislocation of ≥1 joint with concomitant dorsal dislocation of ≥1 joint. Since dorsal ligaments are stronger than volar ligaments, volar ligaments get damaged more easily, allowing the metacarpal to dislocate toward the intact dorsal ligament [7].
The diagnosis is easily missed, as localized swelling may obscure the clinical deformity, and routine radiographs may not show the displacement clearly. Even though patients with numerous CMCJ injuries frequently experience substantial edema, we do not advise postponing surgical intervention since the severely misaligned bones cause persistent swelling. After surgery, hand elevation and active finger mobilization typically help this swelling go down [8]. Hence, a systematic and thorough examination of the radiographs is necessary. A postero-anterior, dead lateral, and oblique views are to be done to start with. Several features should be assessed on all radiographs. Gilula’s three carpal arcs, as well as the “parallel M” lines along the 2nd–5th CMC joint, should be maintained [9]. All articular surfaces should be parallel, with the maintenance of uniform joint space, and there should be no overlap of surfaces [10]. The metacarpal cascade lines can be checked to assess metacarpal disassociation in a normal hand; lines drawn along the axis of the 2nd–5th metacarpals should intersect at a point approximately 2 cm proximal to the articular surface of the distal radius [7]. Chmell described the “oblique metacarpal line”, whereby a tangential line drawn across the metacarpal heads of the 3rd–5th rays allows identification of shortening, which may result from CMC joint injury or shaft fracture. In a lateral radiograph of the uninjured wrist, the radius, lunate, capitate, and third metacarpal should form a continuous axis. A CT scan is an option to rule out any fracture dislocations.
CMC dislocation of all the fingers of the ulnar side of the hand is a rare form of hand injury. It is important to diagnose and treat this injury to avoid the considerable morbidity associated with this condition. Even though these injuries can be treated by different methods, better results are seen in open reduction and internal fixation with K-wires. It will help in the accurate reduction of dislocations and early functional recovery.
Carpometacarpal dislocations of the 2nd–5th digits without fracture are rare and frequently missed due to swelling and overlapping metacarpals on radiographs. Diagnosis requires a strong index of suspicion, systematic radiographic evaluation (parallel M lines, cascade lines, Gilula arcs), and early CT where necessary. Stable alignment and superior functional results are achieved through anatomical reduction, which starts with the third CMC joint stabilization as the cornerstone and is followed by K-wire fixation. Poor hand function, chronic instability, and lingering pain are avoided with early surgery.
References
- 1. Pundkare GT, Patil AM. Carpometacarpal joint fracture dislocation of second to fifth finger. Clin Orthop Surg 2015;7:430-5. [Google Scholar] [PubMed]
- 2. Henderson JJ. Arafa MA. Carpometacarpal dislocation. An easily missed diagnosis. J Bone Joint Surg Br 1987;69:212-4. [Google Scholar] [PubMed]
- 3. Sharma AK, John JT. Unusual case of carpometacarpal dislocation of all the four fingers of ulnar side of hand. Med J Armed Forces India 2005;61:188-9. [Google Scholar] [PubMed]
- 4. De Beer JV, Maloon S, Anderson P, Jones G, Singer M. Multiple carpo-metacarpal dislocations. J Hand Surg Br 1989;14:105-8. [Google Scholar] [PubMed]
- 5. El-Shennawy M, Nakamura K, Patterson RM, Viegas SF. Three-dimensional kinematic analysis of the second through fifth carpometacarpal joints. J Hand Surg Am 2001;26:1030-5. [Google Scholar] [PubMed]
- 6. Kumar S, Arora A, Jain AK, Agarwal A. Volar dislocation of multiple carpometacarpal joints: Report of four cases. J Orthop Trauma 1998;12:523-6. [Google Scholar] [PubMed]
- 7. Chheda AP, Anand BV, Palanisami RS, Rishab C, Aleyas A. Multiple carpometacarpal dislocations. A case series. J Chem Health Risks 2025;15:2576-80. [Google Scholar] [PubMed]
- 8. Bhardwaj P, Sivakumar BS, Vallurupalli A, Pai M, Sabapathy SR. Fracture dislocations of the carpometacarpal joints of the fingers. J Clin Orthop Trauma 2020;11:562-9. [Google Scholar] [PubMed]
- 9. I Broken. Figure 2 Arc I Broken at Lunotriquetral. Available from: https://www ajronline.org Last accessed on 23 Dec 2025]. [Google Scholar] [PubMed]
- 10. Fisher MR, Rogers LF, Hendrix RW. Systematic approach to identifying fourth and fifth carpometacarpal joint dislocations. AJR Am J Roentgenol 1983;140:319-24. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2023 Two Discrete Intra-articular Synovial Hemangiomas of a Knee Joint Presenting as Chronic Knee Pain
November 10, 2023 Two Discrete Intra-articular Synovial Hemangiomas of a Knee Joint Presenting as Chronic Knee Pain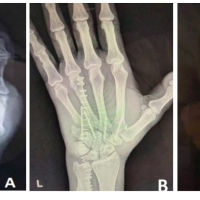 December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature
December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature February 10, 2021 A Rare Case of Contiguous Three-level Lumbar Burst Fractures-treated with Combined Posterior Stabilization and Anterior Fusion
February 10, 2021 A Rare Case of Contiguous Three-level Lumbar Burst Fractures-treated with Combined Posterior Stabilization and Anterior Fusion April 1, 2026 Campylobacter Fetus Periprosthetic Joint Infection: A Case Report and Review of Literature from the Past Three Decades
April 1, 2026 Campylobacter Fetus Periprosthetic Joint Infection: A Case Report and Review of Literature from the Past Three Decades