
Not all cystic-appearing hand swellings are ganglion cysts – vascular lesions, such as cavernous hemangiomas must be considered, as accurate diagnosis and surgical planning depend on appropriate imaging and recognition of their intraoperative characteristics.
Dr. Mihir Maniar, Department of Orthopaedics, Wockhardt Hospitals Ltd, Institute of Medical Science and Research, Evershine Road, Naya Nagar, Mira Road East, Thane - 401107, Maharashtra, India. E-mail: mihirmaniar.15@gmail.com
Abstract
Introduction: Vascular lesions, such as cavernous hemangiomas of the finger’s flexor tendon sheath are uncommon and can easily be mistaken for more common masses, such as ganglion cysts. Early recognition is important to plan appropriate imaging and excision with correct surgical technique.
Case Report: We report a 60-year-old female who presented with a painless, slowly enlarging subcutaneous swelling over the palmar aspect of her right hand. The initial clinical impression was a ganglion cyst of the flexor sheath. Ultrasound suggested a hypoechoic lesion without any internal vascular flow on Doppler. However, intraoperative findings revealed a vascular mass firmly adherent to the flexor tendon sheath. Complete excision was performed. Final histopathological examination confirmed the diagnosis of cavernous hemangioma. The patient had an uneventful recovery with full finger motion and no recurrence at annual follow-up.
Conclusion: Cavernous hemangioma of the flexor tendon sheath can present like a ganglion cyst. Pre-operative suspicion (especially when imaging shows internal vascularity), careful operative planning, and complete excision are keys to a good outcome.
Keywords: Cavernous hemangioma, tendon sheath, ganglion cyst, hand lump, case report.
Patients with a lump or swelling on their hand or wrist frequently seek evaluation in orthopedic clinics. While ganglion cysts are by far the most common type of these palpable soft-tissue masses, clinicians must also consider a broader differential diagnosis. Among the less frequent but important possibilities are vascular lesions, such as hemangiomas, especially when they originate from tendon sheaths or synovial tissue. Their pre-operative misdiagnosis is not uncommon [1,2,3]. The diagnostic challenge arises because tenosynovial hemangiomas often present with clinical features similar to ganglion cysts. They tend to feel soft and fluctuant and appear in comparable locations, creating a diagnostic and management dilemma. Maintaining awareness of this mimicry is clinically crucial, as the approach to a suspected vascular lesion differs significantly: It typically demands more specific pre-operative imaging and a carefully planned surgical strategy to control bleeding [2,3,4]. As highlighted in published literature and case series, hemangiomas represent a well-documented, though relatively rare, cause of hand masses that are often mistaken for the more ubiquitous ganglion cyst [2,3,4,5,6,7].
A 60-year-old, right-handed woman sought evaluation for a slow-growing lump on the palm of her right hand, which she had noticed over the past 6 months. She reported no preceding trauma, pain was minimal, and there were no neurological symptoms. There was no relevant medical history.
Clinical findings
On examination, there was a 2 × 1.5 cm, soft, non-tender, slightly compressible swelling over the volar aspect, over the distal palmar crease along the 2nd metacarpal region. The swelling was mobile in the transverse plane but was adherent to deep structures on longitudinal palpation. The overlying skin was normal, and there was no pulsation, audible bruit, or warmth. She maintained full motion in the metacarpophalangeal and interphalangeal joints of her fingers. Neurological and vascular assessments were normal.
Investigations
Radiographs of the hand were unremarkable. An ultrasound study identified a well-defined, fluid-filled (anechoic to hypoechoic) mass lying next to the flexor tendon sheath. The lesion glided along with the tendon during active finger motion, and no calcifications were seen. A magnetic resonance imaging (MRI) was not performed at this stage based on the clinical assessment and available resources.
Differential diagnosis
Ganglion cyst, giant cell tumor of tendon sheath, tenosynovitis with cystic change, hemangioma/vascular malformation.
Treatment
Surgery was performed under regional anesthesia with a tourniquet applied. A Bruner-type incision was made over the mass. Upon dissection, a dark bluish-red, compressible vascular tumor was identified, densely adherent to the flexor tendon sheath of the index finger (Fig. 1). The lesion consisted of numerous thin-walled vessels and bled actively when incised (Fig. 1).

Figure 1: Intraoperative photograph. The image shows the surgical exposure through a volar Bruner (zig-zag) incision, revealing the characteristic appearance of the lesion: a well-defined, dark red, lobulated, and compressible mass adherent to the flexor tendon sheath.
Using bipolar cautery for meticulous hemostasis, the mass was completely removed along with a margin of the involved synovial sheath, while carefully preserving the underlying flexor tendon. The tourniquet was released to ensure complete hemostasis before wound closure.
Histopathology
Microscopic analysis of the excised tissue confirmed the diagnosis. It revealed multiple, dilated, blood-filled vascular spaces lined by a single layer of endothelial cells, consistent with a cavernous hemangioma (Fig. 2a-c).
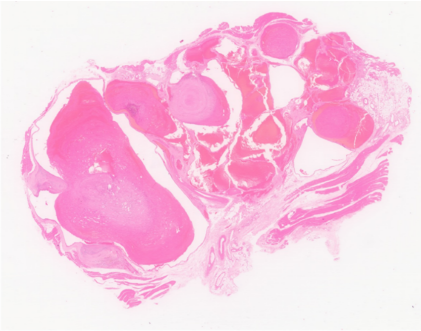
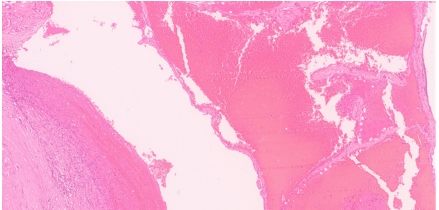
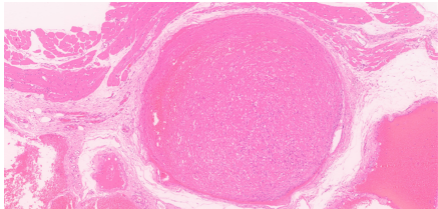
Figure 2: (a) Histopathological analysis. Low-power photomicrograph (Hematoxylin and Eosin [H&E] stain) of the excised specimen reveals a well-circumscribed lesion composed of numerous, dilated, thin-walled vascular spaces. (b and c) High-power photomicrograph (H&E stain) details the lesion’s architecture, showing large, blood-filled cavernous channels lined by a single layer of benign, flattened endothelial cells – findings diagnostic of a cavernous hemangioma.
Post-operative recovery was uneventful. The patient started early range-of-motion exercises under hand therapy. At the 1-year follow-up visit, she had regained full, painless finger motion. There were no clinical signs of recurrence, and reported satisfaction with the final result (Fig. 3).

Figure 3: Post-operative clinical photograph. A well-healed surgical scar on the volar hand is shown, demonstrating a favorable cosmetic outcome without evidence of scar contracture.
Hemangiomas of the hand and tendon sheath are uncommon and can present at any age. These vascular lesions are categorized into types, such as capillary, cavernous, and venous; cavernous hemangiomas are typically composed of large, dilated vascular channels and are often situated in deeper tissues [1,3,6]. In clinical practice, a soft, mobile hand mass is frequently assumed to be a ganglion cyst, given its high prevalence, especially if an initial ultrasound describes it as “cystic.” This underscores a key diagnostic challenge: The potential for mimicry. Without specific vascular assessment, a tenosynovial hemangioma can easily be mistaken for a benign ganglion or other common soft-tissue tumor. Such misdiagnosis can lead to unprepared surgeons encountering unexpected vascularity during surgery, which may result in incomplete removal and eventual recurrence [6,8]. Doppler can demonstrate internal vascular flow, and MRI provides superior anatomical detail and characteristic signal patterns that can confirm a vascular diagnosis, thereby allowing for appropriate surgical planning. For any clinically ambiguous hand mass where a vascular origin is considered, MRI should be regarded as the imaging modality of choice, as it accurately defines the lesion’s extent and its relationship to critical neurovascular structures [4,5]. Surgical excision with a margin of involved synovium/tendon sheath is the treatment of choice for localized lesions and is usually curative [2,3,7]. Inadequate resection is the primary cause of recurrence [6,8]. Achieving adequate access is vital; a Bruner-type incision on the volar aspect provides excellent exposure of the flexor tendon sheath and neurovascular bundles, facilitating safe dissection and complete removal of the lesion while minimizing trauma to surrounding structures [9,10]. Some diffuse vascular malformations may require staged excision, sclerotherapy, or multidisciplinary management with interventional radiology and vascular surgery. Pre-operative planning for any suspected vascular lesion must prioritize hemostasis. This includes ensuring a tourniquet and bipolar cautery are readily available and, for extensive lesions, considering pre-operative angiography or embolization [8]. In our reported case, we proceeded without a pre-operative MRI. However, intraoperative findings revealed the classic appearance of a cavernous hemangioma (Fig. 1). A longitudinal Bruner incision was utilized, which afforded optimal visualization. With meticulous dissection and en bloc excision of the lesion with a cuff of involved sheath, we were able to preserve the underlying flexor tendon completely. Similar successful excisions have been described in isolated reports of flexor tendon sheath hemangiomas [3,7]. The patient experienced a straightforward recovery and remained recurrence-free with full function at the 1-year follow-up. While this single case has its limitations – notably the absence of a pre-operative MRI and the need for longer-term follow-up – it reinforces several important clinical lessons:
- It is vital to maintain a broad differential diagnosis for any hand mass
- A vascular lesion must be considered when ultrasound findings are atypical or show internal flow, prompting more definitive imaging
- Surgical planning should always account for the possibility of a vascular tumor to ensure complete excision and safe hemostatic control
- The Bruner approach allows for adequate exposure, ensures flap vascularity, and reduces the risk of a flexor contracture.
While ganglion cysts are the most common soft-tissue masses in the hand, clinicians should be aware that rarer entities, such as cavernous hemangiomas can present with an identical clinical picture. A high index of suspicion, supported by targeted imaging, such as Doppler ultrasound or MRI, is essential for accurate pre-operative diagnosis and safe surgical planning. When properly managed with careful dissection and complete excision, these vascular lesions can be successfully removed with excellent functional recovery and a low likelihood of recurrence.
Do not assume every soft, cystic-appearing hand mass is a ganglion. If imaging suggests internal vascularity or if the lesion’s clinical behavior is atypical, consider hemangioma in the differential and obtain MRI or Doppler ultrasound – planned excision with careful hemostasis yields good functional outcomes.
References
- 1. Devaney K, Vinh TN, Sweet DE. Synovial hemangioma: A report of 20 cases with differential diagnostic considerations. Hum Pathol 1993;24:737-45. [Google Scholar] [PubMed]
- 2. Talwalkar SC, Hayton MJ, Stilwell JH, Temperley D, Freemont AJ. Tenosynovial haemangioma of the finger. Acta Orthop Belg 2005;71:618-21. [Google Scholar] [PubMed]
- 3. Dalei TR, Loya VK. Tendon sheath hemangioma. J Hand Microsurg 2019;11 Suppl 1:S22-5. [Google Scholar] [PubMed]
- 4. Weinzweig J, Watson HK, Wiener BD, Genter BE. Hemangioma of the extensor pollicis brevis in the first dorsal compartment: An unusual cause of bilateral de Quervain’s disease. J Hand Surg Am 1996;21:256-8. [Google Scholar] [PubMed]
- 5. Waddell GF. A haemangioma involving tendons. J Bone Joint Surg Br 1967;49:138-41. [Google Scholar] [PubMed]
- 6. Spinner M, Moon S, Young L. Recurrent cavernous haemangioma of the extensor tendons of the hand. Hand 1983;15:223-7. [Google Scholar] [PubMed]
- 7. Kim DH, Jeong M, Shim SB, Lee JH, Kim CK. Hemangioma of the flexor digitorum superficialis tendon sheath in the hand. J Korean Soc Surg Hand 2014;19:154-8. [Google Scholar] [PubMed]
- 8. Lee TC, Chien SH, Liu PC, Cheng YM. A rapidly recurrent synovial hemangioma involving tendon sheath: A rare case in the finger. Formosan J Musculoskelet Disord 2011;2:135-8. [Google Scholar] [PubMed]
- 9. Bruner JM. The zig-zag volar-digital incision for flexor-tendon surgery. Plast Reconstr Surg 1967;40:571-4. [Google Scholar] [PubMed]
- 10. Wolfe SW, Pederson WC, Kozin SH, Cohen MS, editors. Green’s Operative Hand Surgery. 8th ed. Philadelphia, PA: Elsevier; 2022. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report
July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report