
3D-printed patient-specific implants enable precise reconstruction and functional restoration in complex distal tibia defects following wide tumor resection.
Dr. Mohit Basra, Department of Orthopaedics, Maulana Azad Medical College, Old Resident Doctor Hostel, New Delhi, India. E-mail: drmohitbasra@gmail.com
Abstract
Introduction: The advent of 3D-printed, patient-specific implants has revolutionized limb salvage surgeries, offering precise, personalized solutions for complex skeletal reconstructions.
Case Report: We describe a case of 32-year-old lady with a recurrent distal tibia giant cell tumor. Wide resection followed by reconstruction with 3D-printed customized implant was performed. At 2-year follow-up, the patient achieved full weight-bearing and American Orthopaedic Foot and Ankle Society Ankle-Hindfoot score improved from 30 preoperatively to 84 postoperatively.
Conclusion: This case highlights the potential of 3D-printed customized implants in complex joint reconstructions of large defects after wide tumor resections with personalized design and maintaining joint function.
Keywords: Giant cell tumor, recurrent, distal tibia, 3D printed, patient-specific implant.
Giant cell tumors (GCTs) of distal tibia pose distinct surgical challenges due to the anatomy of the joint and the complex mechanical requirements of this weight-bearing area. Wide resection and reconstruction of the distal tibia have traditionally relied on techniques like structural allografts, autografts with ankle arthrodesis or endoprosthetic reconstruction. All these techniques have specific limitations such as altered anatomy, limited or insufficient remaining host bone, periprosthetic fractures, inadequate soft tissue coverage, infection, and gait abnormalities. The emergence of 3D-printed implants has revolutionized orthopedic oncology by developing patient-specific prostheses that address these limitations effectively. Pre-operative computed tomography (CT) scans are used to develop patient-specific 3D-printed titanium or chromium-cobalt implants. Such implants help to preserve joint anatomy, function and minimize limb-length discrepancies. This case report outlines the application of a 3D-printed, patient-specific distal tibia prosthesis for recurrent GCT. We aim to demonstrate how this novel approach overcomes the drawbacks of conventional techniques along with oncological safety and functional restoration, thus offering a tailored treatment for anatomically complex tumors. We seek to add to the expanding body of evidence supporting the use of personalized orthopedic solutions in complex tumor reconstructions.
We present a case of a 32-year-old woman who presented with a 3-month history of progressive pain and swelling over the right ankle with difficulty in ambulation. 7 years earlier, she had undergone extended curettage and bone cementing for GCT of the right distal tibia. On examination, the range of motion at the ankle joint was painful and restricted: 20° plantarflexion and 0° of dorsiflexion. The American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hind foot score (as per Orthotoolkit) was calculated to be 30. Radiological investigations were done which revealed a heterogeneous lesion on X-ray, CT, and magnetic resonance imaging in the distal tibia measuring 4.2 ´ 3.4 ´ 4.5 cm (craniocaudal ´ transverse ´ anteroposterior) (Fig. 1).
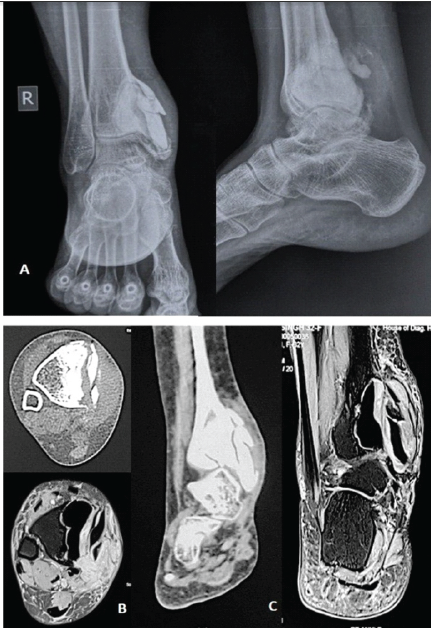
Figure 1: Pre-operative imaging showing recurrence of giant cell tumors with bone cement in situ. (a) X-ray anteroposterior and lateral, (b) axial section of computed tomography (CT) and magnetic resonance imaging (MRI), (c) coronal section of CT and MRI.
There was cortical destruction along with soft tissue extension and was staged as Campanacci grade 3. Histopathological examination confirmed recurrence of GCT. Four doses of denosumab 120 mg/weekly were given pre-operatively, resulting in consolidation, sclerosis of tumor margins, and decreased soft tissue component. Thereafter, we decided to salvage the ankle joint by wide resection and reconstruction with customized 3D-printed implant.
Pre-operative planning
As illustrated in Fig. 2 and Fig.3.
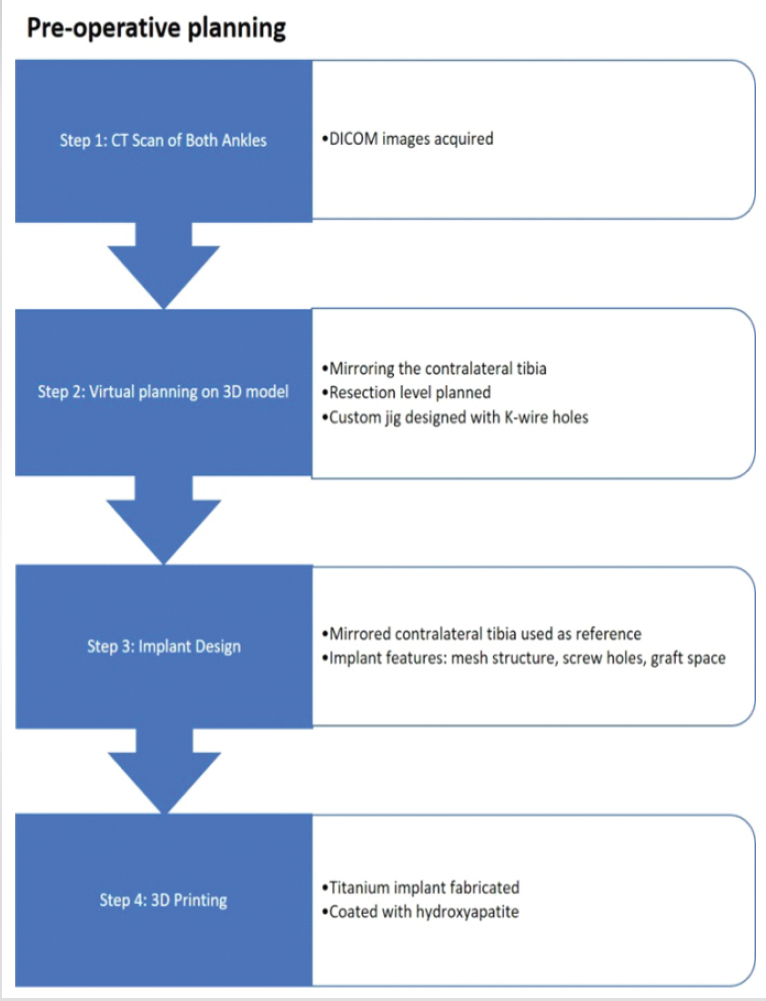
Figure 2: Flowchart depicting the preoperative planning stages, from computed tomography scan acquisition and 3D model development to the design of a custom 3D-printed titanium implant.
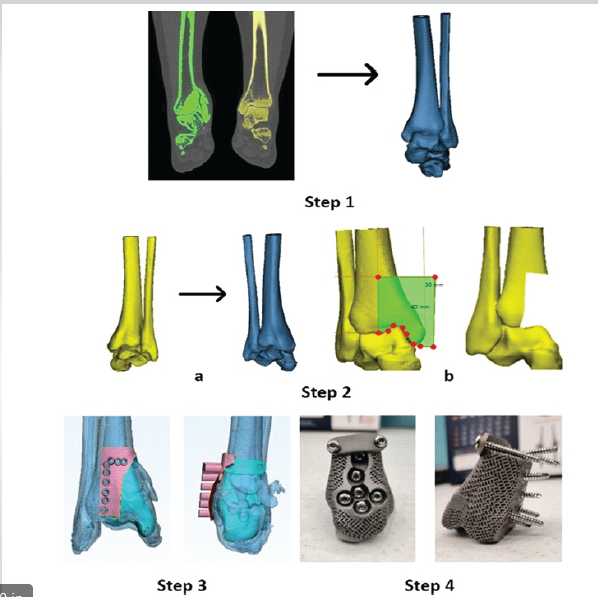
Figure 3: The steps of virtual planning and final implant. Step 1: Generating 3D model from digital imaging and communications in medicine images. Step 2: Mirroring the normal tibia to use as a reference and planning the resection. Step 3: Overlapping normal with diseased tibia showing base for the 3D implant and making a jig with holes for K-wire for resection. Step 4: Final 3D-printed titanium implant with mesh structure.
Surgical technique
The tumor was approached medially through the previous incision and exposed after careful soft tissue dissection. A resection jig was placed, and K-wires marked the resection margins, confirmed fluoroscopically. The tumor was excised with an oscillating saw, matching the pre-operative plan. A 10 cm fibular strut and iliac crest graft from the contralateral side were integrated into the customized 3D-printed implant. After reaming the canal and preparing the tibia, the construct was implanted and securely fixed, with the strut extending intramedullary. Implant stability was achieved through its customized contour, which articulated distally with the talus, conformed to the lateral surface of the tibia, and matched the proximal tibial resection surface. Additional fixation was provided by three proximal and three distal screws passed through the implant into the free fibula and anchoring at the tibial far cortex. The ankle joint capsule was sutured to the implant, thereby allowing reconstruction of the ankle joint and enhancing rotational stability.
Post-operative period
The post-operative period was uneventful. The patient progressed from non-weight bearing to partial weight bearing with an ankle-foot orthosis, followed by full weight bearing by 6 weeks. At 1-year follow-up, she was asymptomatic, performing routine activities with 40° plantarflexion and 0° dorsiflexion. At 2 years, ankle range of motion was 30° plantarflexion and 0° dorsiflexion and the AOFAS Ankle – Hindfoot score improved from 30 preoperatively to 84 postoperatively (Fig. 4).
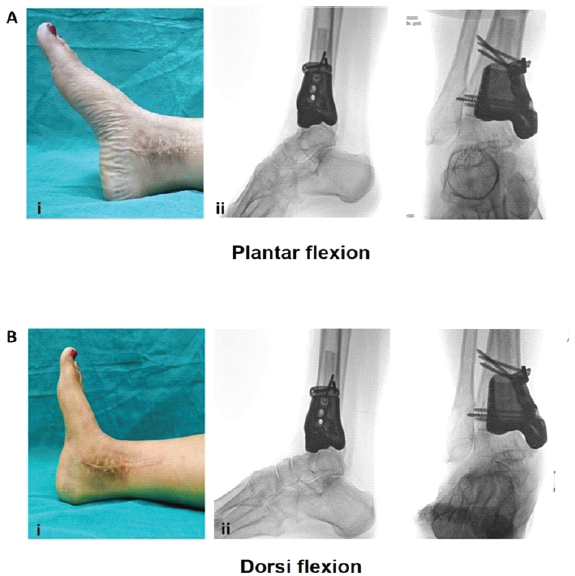
Figure 4: Illustration of functional ankle range of motion achieved. (a) Post-operative clinical (i) and fluoroscopic (ii) images demonstrating ankle plantarflexion in anteroposterior (AP) and lateral views. (b) Clinical (i) and fluoroscopic (ii) images showing ankle dorsiflexion in AP and lateral views at final follow-up.
Recurrent GCTs pose significant therapeutic challenges due to their propensity for local destruction. Our patient’s initial management with curettage and bone cementing 7 years prior aligns with standard practice for primary GCTs. Treatment modalities for recurrent GCTs of the distal tibia range from repeated curettage with adjuvants to wide resection and arthrodesis or reconstruction. Intralesional curettage, often augmented with phenol, cryotherapy, or polymethylmethacrylate cement, aims to preserve joint function but carries a high recurrence risk [1]. A systematic review in 2023 done for the treatment of recurrent GCT of bones comprising 458 patients in 12 studies found that a second recurrence occurred in 25.7% cases treated with intralesional curettage [2]. Wide resection results in significant bone and articular loss, complicating reconstruction. Traditional reconstruction options include ankle arthrodesis, structural allografts, or modular endoprostheses. Arthrodesis provides stability but sacrifices joint mobility, leading to gait abnormalities and reduced quality of life. Allografts, while preserving bone stock, are plagued by complications such as infection, non-union, and resorption [3]. Modular endoprostheses, though widely used, often fail to match the patient’s unique anatomy, resulting in periprosthetic fractures (17%), implant loosening (19%), and infection rates of up to 34% [4]. These disadvantages underscore the need for innovative solutions like patient-specific 3D-printed implants.
The use of a 3D-printed, patient-specific distal tibia prosthesis offers several advantages over conventional methods. A 2018 study showed that 11 patients with distal radius GCT managed with patient-specific 3D-printed customized implant showed significant reduction in pain (Visual Analog Scale [VAS] score, P < 0.001) and functional outcome as assessed from disabilities of the arm, shoulder, and hand questionnaire and Mayo wrist outcome scores with no recurrence and complications after a mean follow-up of 14.45 months [5]. Lu et al. report a successful reconstruction of a proximal tibia defect in a 15-year-old with osteosarcoma using a custom 3D-printed prosthesis, preserving the knee joint and achieving good function at 26 months with no complications [6]. The precision of 3D-printed jigs ensures accurate tumor resection, minimizing damage to surrounding tissues and reducing operative time – a critical factor in reducing infection risk [7]. Yon et al. report a case series of 2 cases using 3D-printed, patient-specific prostheses for foot and ankle tumor resections, showing improved AOFAS and VAS scores, stable placement, and early bone integration over 2 years [8]. He et al. report on six patients with talus malignant tumors treated with 3D-printed custom-made modular prostheses from 2016 to 2021, achieving a mean musculoskeletal tumor society score (MSTS-93) of 26.8 and AOFAS scores of 88.5 over a 54.8-month follow-up. The approach showed good osseointegration, minimal complications (one delayed wound healing) and preserved joint function, suggesting a viable reconstruction option [9]. Huang et al. demonstrated that 3D-printed, patient-specific hemipelvic prostheses achieved accurate acetabular reconstruction with a mean MSTS-93 score of 18.2 at 36.2-month follow-up. The study reported reduced aseptic loosening rates when ≥4 sacral screws were used, highlighting improved mechanical stability and acceptable early functional outcomes [10]. This case reinforces that management of recurrent GCT at rare anatomical sites is predominantly guided by available literature due to the paucity of cases. Although this limits the ability to independently assess treatment-related concerns, the case illustrates the feasibility of patient-specific 3D-printed reconstruction, achieving limb salvage and early functional recovery.
Limitations
Our case report is a single-patient study design, which restricts the generalizability of the findings. The use of patient-specific 3D-printed implants has practical concerns related to cost and availability, particularly in resource-limited environments. These issues have yet to be fully explored through formal economic analyses. The relatively short follow-up period of 2 years prevents a comprehensive assessment of implant durability. Long-term observation will therefore be essential to determine the longevity of the metal articular surface at the ankle joint and to identify potential late complications such as wear, loosening, or implant failure.
Patient-specific 3D-printed implants represent a promising advancement in managing recurrent GCTs of the distal tibia, offering oncological safety, functional restoration, and personalized design. While challenges like cost and technical complexity remain, this case and supporting literature encourage their exploration as a viable alternative to traditional reconstructions.
This case demonstrates that 3D-printed, patient-specific implants can offer a reliable limb-salvage option after distal tibia tumor resection, also preserving joint function and enabling early weight-bearing. Their application could redefine reconstruction methods in challenging orthopedic and oncologic cases.
References
- 1. Klenke FM, Wenger DE, Inwards CY, Rose PS, Sim FH. Giant cell tumor of bone: Risk factors for recurrence. Clin Orthop Relat Res 2010;469:591-9. [Google Scholar] [PubMed]
- 2. Pitsilos C, Givissis P, Papadopoulos P, Chalidis B. Treatment of recurrent giant cell tumor of bones: A systematic review. Cancers 2023;15:3287. [Google Scholar] [PubMed]
- 3. Ippolito JA, Martinez M, Thomson JE, Willis AR, Beebe KS, Patterson FR, et al. Complications following allograft reconstruction for primary bone tumors: Considerations for management. J Orthop 2018;16:49-54. [Google Scholar] [PubMed]
- 4. Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, Cheong D, et al. Failure mode classification for tumor endoprostheses: Retrospective review of five institutions and a literature review. J Bone Joint Surg Am 2011;93:418-29. [Google Scholar] [PubMed]
- 5. Lu M, Min L, Xiao C, Li Y, Luo Y, Zhou Y, et al. Uncemented three-dimensional-printed prosthetic replacement for giant cell tumor of distal radius: A new design of prosthesis and surgical techniques. Cancer Manag Res 2018;10:265-77. [Google Scholar] [PubMed]
- 6. Lu M, Li Y, Luo Y, Zhang W, Zhou Y, Tu C. Uncemented three-dimensional-printed prosthetic reconstruction for massive bone defects of the proximal tibia. World J Surg Oncol 2018;16:47. [Google Scholar] [PubMed]
- 7. Wong KC, Kumta SM, Sze KY, Wong CM. Use of a patient-specific CAD/CAM surgical jig in extremity bone tumor resection and custom prosthetic reconstruction. Comput Aided Surg 2012;17:284-93. [Google Scholar] [PubMed]
- 8. Yon CJ, Choi BC, Lee JM, Lee SW. Personalized 3D-printed prostheses for bone defect reconstruction after tumor resection in the foot and ankle. J Funct Biomater 2025;16:62. [Google Scholar] [PubMed]
- 9. He X, Lu M, Zou C, Li Z, Gong T, Kenmegne GR, et al. Three-dimensional printed custom-made modular talus prosthesis in patients with talus malignant tumor resection. J Orthop Surg Res 2024;19:273. [Google Scholar] [PubMed]
- 10. Huang X, Huang D, Lin N, Yan X, Qu H, Ye Z. 3D-printed prosthesis with an articular interface for anatomical acetabular reconstruction after type I + II (+ III) internal hemipelvectomy: Clinical outcomes and finite element analysis. J Bone Joint Surg Am 2025;107:184-95. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 A Rare Case Report of Giant Cell Tumor in the Distal Tibia: Management with Tumor Excision and Limb Reconstruction with Ilizarov Fixator
July 1, 2025 A Rare Case Report of Giant Cell Tumor in the Distal Tibia: Management with Tumor Excision and Limb Reconstruction with Ilizarov Fixator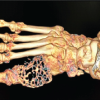 June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction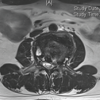 May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report
May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability
April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability