
Surgery for a floating lamina carries a high risk; therefore, it is important to prevent pseudoarthrosis and spinal restenosis during the initial laminoplasty.
Dr. Arihiko Tsukamoto, Department of Orthopaedic Surgery, Sapporo Medical University Hospital, Sapporo, Hokkaido, Japan. E-mail: aritsukatennis1104@yahoo.co.jp
Abstract
Introduction: Although cervical laminoplasty is a commonly performed procedure, several potential pitfalls must be recognized.
Case Report: The patient was a 68-year-old man who presented with myelopathy caused by a floating lamina resulting from pseudoarthrosis at the lateral gutter and reclosure of the lamina following cervical laminoplasty. Intraoperatively, the C2 and C3 laminae were found to be mobile. To avoid spinal cord injury, the laminae were stabilized using forceps while carefully drilling them with a high-speed burr under spinal cord monitoring. Scar tissue was removed, and the dural sac was decompressed. The patient’s symptoms improved early after surgery.
Conclusion: In the present case, medial deviation of the lateral gutter and damage to the inner cortex of the lamina during the initial surgery likely led to pseudoarthrosis at the lateral gutter. Subsequent osteophyte formation associated with the pseudoarthrosis, along with reclosure of the lamina, resulted in recurrence of myelopathic symptoms. Careful attention to the positioning of the lateral gutter is therefore essential when performing cervical laminoplasty.
Keywords: Laminoplasty, floating lamina, re-close of lamina, pseudarthrosis of the lateral gutter.
Various techniques for cervical laminoplasty have been reported, including the double-door method, open-door method, and skip laminectomy [1,2,3]. Here, we report a case of myelopathy caused by pseudarthrosis at the lateral gutter and reclosure of the lamina due to malposition of the lateral gutter.
The patient was a 68-year-old male who presented with gait instability, fine motor dysfunction of the fingers, and numbness in both upper limbs. Eight years earlier, he had undergone C2–C5 laminoplasty at a previous hospital for numbness in both upper limbs, which resulted in symptomatic relief. However, 6 months ago, the numbness recurred, prompting him to consult the previous hospital again. Due to comorbidities, he was referred to our institution. Subsequently, the numbness in his upper limbs gradually worsened, and he developed fine motor impairment in his fingers and gait instability. Although surgery was planned, it had to be postponed due to the onset of pulmonary thromboembolism. Once anticoagulation therapy could be temporarily discontinued, the surgery was performed. His medical history included thoracic plasmacytoma, for which he was undergoing chemotherapy. On examination, the patient exhibited numbness and impaired temperature and pain sensation throughout both upper limbs. He had experienced multiple episodes of urinary incontinence, indicating bladder and bowel dysfunction. Due to spasticity and unsteadiness, independent walking was difficult. Fine motor dysfunction of the fingers made buttoning clothes and writing difficult. Muscle strength was mildly reduced to MMT Grade 4 in both upper limbs below the deltoid muscles. The biceps, brachioradialis, and triceps tendon reflexes were hyperactive. In the lower limbs, tendon reflexes were also hyperactive, and bilateral ankle clonus was present. Both Hoffmann’s and Trömner’s reflexes were positive bilaterally. The finger escape sign was Grade 2 on the right and Grade 1 on the left. In the 10-s test, the patient was able to perform 13 movements on both sides. The Romberg sign was positive. In the previous pre-operative plain radiographs, no abnormalities in cervical alignment were observed. Magnetic resonance imaging (MRI) showed spinal cord compression at the C2/3, C4/5, and C5/6 levels (Fig. 1).
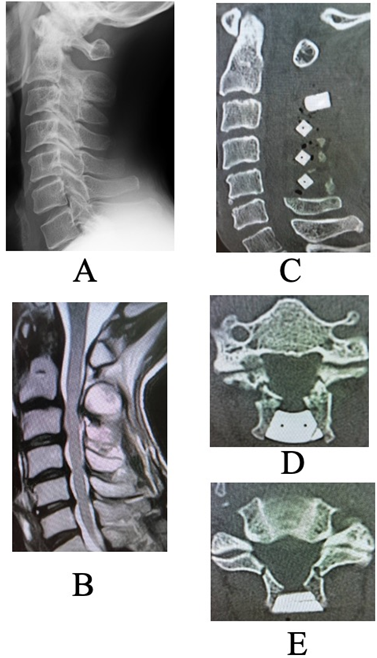
Figure 1: (a and b) Pre-operative images before the initial surgery. (a) Plain lateral radiographs Neutral position. No abnormal alignment or dynamic instability was observed. (b) Sagittal magnetic resonance imaging image. Spinal cord compression is evident at the C2/3, C4/5, and C5/6 levels. (c, d, e): Post-operative computed tomography after the initial surgery. (c) Sagittal view (d) Axial view at the C2 lamina level (e) Axial view at the C3 lamina level. Lamina inner plate damage at the lateral gutters is observed at both C2 and C3, but the spacers are well positioned, and sufficient laminar opening was achieved. At the C3 level, the lateral gutters were created medial to the medial pedicular line.
A C2–C5 double-door laminoplasty was performed. Post-operative computed tomography (CT) revealed a narrow lateral gutter at C3 and damage to the inner lamina, but adequate opening of the lamina was achieved, and the spacer was positioned appropriately (Fig. 1). In the current pre-operative plain radiographs, there was no deterioration in alignment, and no evidence of vertebral slippage or intervertebral instability (Fig. 2).
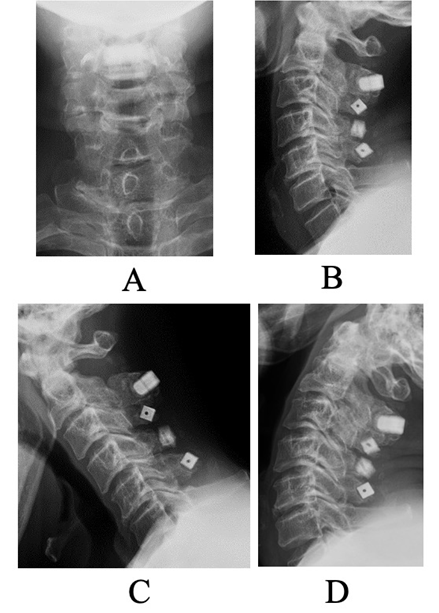
Figure 2: Pre-operative plain lateral radiographs for the current surgery. (a) Anteroposterior view. (b) Neutral lateral view. (c) Flexion view. (d) Extension view. No alignment abnormalities or dynamic instability were observed.
MRI showed spinal cord compression and signal changes at the C3 and C3/4 levels. CT myelography revealed non-union of the lateral gutters at C2 and C3 with osteophyte formation, and the lamina had reclosed. Marked spinal cord compression was observed at the C2–3 laminar level (Fig. 3).
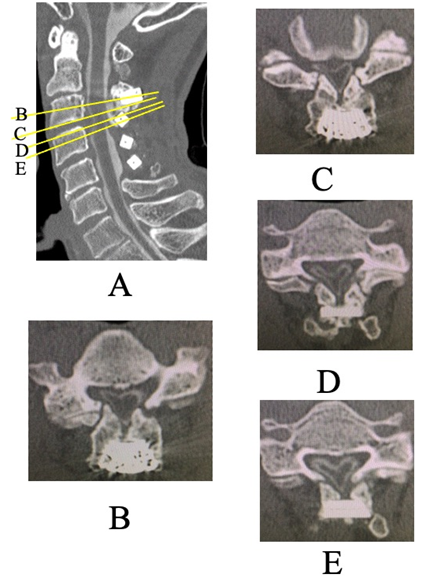
Figure 3: Pre-operative computed tomography Myelography for the current surgery. (a) Sagittal view. (b, c, d, e) Axial view (b) C3 level (c) Inferior edge of C3 (d) Superior edge of C4 (e) C4 level. Pseudarthrosis and osteophyte formation at the lateral gutters of the C2 and C3 laminae, as well as laminar reclosure, were observed. Severe spinal cord compression was noted at the C2/3 laminar level.
The surgical strategy was to first perform posterior resection of the C2 and C3 laminae. If post-operative decompression was deemed insufficient or if symptoms did not improve, anterior decompression and fusion would be considered as an additional procedure. Intraoperatively, the C2 and C3 laminae were found to be floating. While the assistant stabilized the laminae with forceps, they were carefully resected using a high-speed drill along with the artificial bone. Although there was a partial decrease in motor evoked potentials during surgery, lamina removal was continued with care. The dura mater was found to be adherent and scarred; the epidural scar tissue was carefully removed, and decompression was confirmed before concluding the procedure. Postoperatively, numbness in both upper limbs temporarily worsened but subsequently improved. MRI confirmed adequate decompression of the spinal cord, and thus anterior surgery was not performed (Fig. 4).
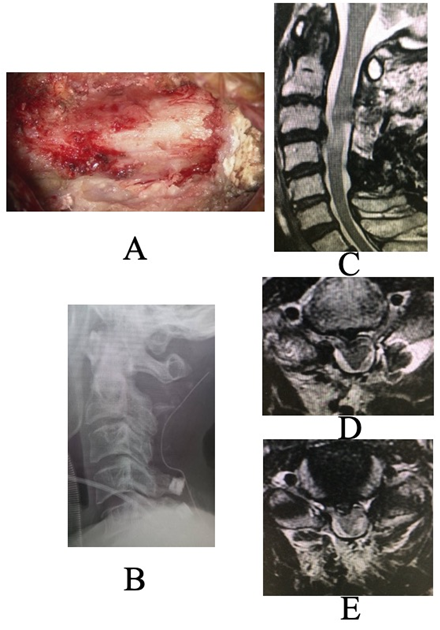
Figure 4: (a) Intraoperative photo after decompression. (b, c, d, e) Post-operative images. (b) Lateral plain radiograph (c) Sagittal magnetic resonance imaging (d) Axial view at the inferior edge of C3 (e) Axial view at the superior edge of C. Adequate spinal cord decompression was achieved.
Fine motor function of the fingers and gait instability improved, and urinary incontinence resolved. The patient was discharged home 2 weeks after surgery. The pre-operative Japanese Orthopaedic Association score was 7.5, which improved to 14.5 1 year postoperatively, with a recovery rate of 73.7%.
Hashimoto et al. reported that among 4,208 cases of cervical laminoplasty, 40 required reoperation, including 10 for radiculopathy, 8 for adjacent segment stenosis, 6 for spacer sinking, 4 for instability, 3 for ossification of the posterior longitudinal ligament (OPLL), 3 for disc herniation, 2 for trauma, 2 for post-operative scar formation, 1 for ossification of the anterior longitudinal ligament (ALL), and 2 for unknown causes [4]. Similarly, Jimbayashi et al. reported that 5 of 169 patients who underwent cervical laminoplasty required reoperation due to refusion of the lamina, and all patients with laminar refusion demonstrated progression of post-operative kyphosis [5]. They also noted that patients who required reoperation had a higher prevalence of neuromuscular or psychiatric disorders and that many had a pre-operative C2–7 lordotic angle of <–10°. The causes of restenosis after cervical laminoplasty have been attributed to insufficient decompression width or inadequate cranio-caudal decompression range at the initial surgery, progression of post-operative kyphotic deformity, and enlargement of OPLL or osteophytes [6,7]. In the present case, there was no significant post-operative kyphotic deformity, OPLL, or marked osteophyte formation between vertebral bodies. It was considered that the narrow width of the lateral gutter at the initial surgery led to gradual refusion of the lamina, and pseudoarthrosis at the lateral gutter resulted in osteophyte formation and recurrence of myelopathy. Because no compression from OPLL or intervertebral osteophytes was observed and no kyphotic deformity was present, additional fixation was deemed unnecessary in this case. Sufficient spinal cord decompression was expected to be achieved by posterior decompression alone. Regarding revision surgery after cervical laminoplasty, Hashimoto reported that 40 out of 4,208 cases required reoperation. The causes included 10 cases of radiculopathy, 8 cases of adjacent segment stenosis, 6 cases of spacer subsidence, 4 cases of instability, 3 cases of OPLL, 3 cases of disc herniation, 2 cases of trauma, 2 cases of post-operative scarring, 1 case of ossification of the ALL, and 2 cases of unknown cause [4]. Sakai et al. reported that laminar refusion occurred in 6 of 110 patients 1 year after cervical laminoplasty, and that clinical outcomes were poorer in the refusion group [8]. They also noted that laminar refusion was more likely to occur in cases using anchors rather than spacers, and identified advanced age, a large cervical sagittal vertical axis, and progression of kyphosis as risk factors. In the present case, the patient was not elderly at the time of the initial surgery (60 years old), a spacer was used, and no kyphotic deformity was observed. Regarding the creation of the lateral gutter, Ueda et al. reported that the greatest expansion of the spinal canal is achieved when the gutter is made along the medial pedicular line, whereas excessive lateral placement may cause difficulty in elevating the lamina and can lead to axial pain due to facet joint destruction [9]. Conversely, if the lateral gutter is positioned too medially, insufficient spinal cord decompression, increased damage to the inner cortical plate of the lamina, and the development of pseudoarthrosis leading to laminar refusion may occur. In the present case, post-operative CT revealed that the lateral gutters were located medially to the medial pedicular line on both sides, with evident damage to the inner laminar cortex. These findings suggest that pseudoarthrosis at the lateral gutter and subsequent laminar refusion were the causes of recurrent myelopathy. A case presenting with laminar refusion and pseudoarthrosis at the lateral gutters resulting in recurrent myelopathy as late as 8 years after surgery is considered extremely rare. Furthermore, preservation of the semispinalis cervicis muscle attached to the C2 spinous process has been reported to be important in posterior cervical decompression, as the spinal canal at the upper cervical levels is inherently wide, allowing preservation in most cases [10]. In the present case, laminoplasty at C2 may not have been necessary at the initial surgery. Damage to the musculature attached to C2 could have resulted in increased mechanical stress on the C2 lamina, potentially contributing to the development of pseudoarthrosis at this level. Reports have described surgical treatment of myelopathy caused by a “floating lamina” arising from congenital anomalies of the axis (C2); in those cases satisfactory decompression was achieved by excising the floating lamina without drilling it [11,12,13]. Drilling a floating lamina with a powered drill is extremely hazardous because of the risk of direct spinal cord injury. In the present case, however, extensive post-operative epidural adhesions made simple excision likely to produce a dural defect; epidural scarring and firm adhesions were indeed observed. Therefore, we performed frequent intraoperative spinal cord monitoring and, with an assistant firmly stabilizing the lamina with forceps, carefully drilled the lamina over an extended period. No post-operative neurological deterioration was observed. Because prior surgery had removed soft-tissue attachments to the lamina (for example, the semispinalis cervicis), mechanical fixation or traction using surrounding tissues was not feasible; manual stabilization of the lamina was therefore preferred. To avoid applying pressure to the lamina during resection, a steel bar was used when removing the high-strength artificial bone spacer, while a diamond burr was employed for the laminar bone. We conclude that when a floating lamina is present without epidural adhesions, excision is appropriate; in cases where adhesions are anticipated, it is important to proceed slowly and meticulously with drilling under continuous spinal cord monitoring.
This case illustrates a rare but significant complication of myelopathy caused by a floating lamina due to reclosure of the lamina following cervical laminoplasty. Although no apparent post-operative kyphotic deformity or instability was observed, the narrow lateral gutter and damage to the inner lamina during the initial surgery are considered contributing factors to pseudoarthrosis and subsequent reclosure. In cases where the lamina is mobile and adhesions are anticipated, careful drilling with secure fixation of the lamina under neuromonitoring is essential. To prevent reclosure, it is crucial to create an appropriately positioned lateral gutter during the initial surgery and to remain vigilant about the risk of recurrence over long-term follow-up.
In cervical laminoplasty, it is important to create the lateral gutter along the medial pedicular line and to avoid injury to the inner cortical plate to prevent reclosure of the lamina and pseudoarthrosis of the lateral gutter. Although drilling the floating lamina after surgery is technically demanding, the lamina should be stabilized as much as possible, and meticulous drilling should be performed under spinal cord monitoring.
References
- 1. Miyazaki K, Tada K, Matsuda Y, Okuno M, Yasuda T, Murakami H. Posterior extensive simultaneous multisegment decompression with posterolateral fusion for cervical myelopathy with cervical instability and kyphotic and/or s-shaped deformities. Spine (Phila Pa 1976) 1989;14:1160-70. [Google Scholar] [PubMed]
- 2. Satomi K, Nishu Y, Kohno T, Hirabayashi K. Long-term follow-up studies of open-door expansive laminoplasty for cervical stenotic myelopathy. Spine 2016;41:299-305. [Google Scholar] [PubMed]
- 3. Kimura I, Shingu H, Nasu Y. Long-term follow-up of cervical spondylotic myelopathy treated by canal-expansive laminoplasty. J Bone Joint Surg Br 1995;77:956-61. [Google Scholar] [PubMed]
- 4. Hashimoto K, Aizawa T, Ozawa H, Tanaka Y, Kusakabe T, Morizumi N, et al. Reoperation rates after laminoplasty for cervical disorders: A 26-year period survival function method analysis. Spine Surg Relat Res 2019;3:304-11. [Google Scholar] [PubMed]
- 5. Jimbayashi H, Iida K, Kazu K, Saiwai H, Kawaguchi K, Matsumoto Y, et al. Cases requiring reoperation for recurrence of myelopathy by lamina closure after a double-door laminoplasty using a modified Kirita-Miyazaki suture method. J Orthop 2023;44:12-6. [Google Scholar] [PubMed]
- 6. Yamazaki A, Homma T, Uchiyama S, Katsumi Y, Okumura H. Morphologic limitations of posterior decompression by midsagittal splitting method for myelopathy caused by ossification of the posterior longitudinal ligament in the cervical spine. Spine (Phila Pa 1976) 1999;24:32-4. [Google Scholar] [PubMed]
- 7. Kimura S, Homma T, Uchiyama S, Katsumi Y, Okumura H. Posterior migration of cervical spinal cord between split laminae as a complication of laminoplasty. Spine (Phila Pa 1976) 1995;20:1284-8. [Google Scholar] [PubMed]
- 8. Sakai K, Hirai T, Arai Y, Maehara H, Torigoe I, Inose H, et al. Laminar closure in double-door laminoplasty for cervical spondylotic myelopathy with nonkyphotic alignment. Spine (Phila Pa 1976) 2021;46:999-1006. [Google Scholar] [PubMed]
- 9. Ueda S, Ioroi Y, Fukuda M, Kumamoto S, Sasaki H, Kawanabe Y, et al. Anatomical evaluation of the lateral hinge in cervical laminoplasty. Spinal Surg 2011;25:147-52. [Google Scholar] [PubMed]
- 10. Kim D, Jang HJ, Moon BJ, Kim KH, Park JY, Kuh SU, et al. Ossification of posterior longitudinal ligament growth in the C1/2 segment and its clinical significance -is C2 total decompression necessary? Spine 2024;49:1692-700. [Google Scholar] [PubMed]
- 11. Nakashima T, Otsuki B, Shimizu T, Fujibayashi S, Murata K, Matsuda S. Cervical myelopathy caused by invagination of floating anomalous C2 and C3 laminae in the spinal canal. Spine Surg Relat Res 2020;20:274-6. [Google Scholar] [PubMed]
- 12. Sakaura H, Yasui Y, Miwa T, Yamashita T, Ohzono K, Ohwada T. Cervical myelopathy caused by invagination of anomalous lamina of the axis. J Neurosurg Spine 2013;19:694-4. [Google Scholar] [PubMed]
- 13. Xu JX, Wang CG, Zhou CW, Tang Q, Li JW, Xu HZ, et al. Cervical myelopathy caused by invaginated laminae of the axis associated with occipitalizaion of the atlas: Case report and literature review. Medicine (Baltimore) 2017;96:e9156. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2022 Novel Approach for Posterior C1 Double-door Laminoplasty with Atlantoaxial Fusion in Progressive Cervical Myelopathy: A Case Report
July 10, 2022 Novel Approach for Posterior C1 Double-door Laminoplasty with Atlantoaxial Fusion in Progressive Cervical Myelopathy: A Case Report January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial January 19, 2013 Fat Embolism Syndrome in Fracture Tibia Treated By Unreamed Interlocking Nail
January 19, 2013 Fat Embolism Syndrome in Fracture Tibia Treated By Unreamed Interlocking Nail October 29, 2014 Fracture of Uncemented Revision Femoral Stems in three Arthroplasty Patients: A Case Series with three different brands.
October 29, 2014 Fracture of Uncemented Revision Femoral Stems in three Arthroplasty Patients: A Case Series with three different brands.