
Early recognition and staged surgical stabilization of cervical facetal dislocation with central cord syndrome can significantly improve neurological outcomes, particularly in elderly patients with degenerative spine disease.
Dr Soumyamay Mukherjee, Department of Orthopaedics, Government Roypettah Hospital, Kilpauk Medical College, Chennai, Tamil Nadu, India. E-mail: soumyamoy345@gmail.com
Abstract
Introduction: Subaxial cervical spine injuries are common following high-energy trauma; however, bilateral facet dislocation at C5–C6 associated with central cord syndrome (CCS) is rare. Such injuries demand early diagnosis and timely surgical intervention to optimize neurological recovery.
Case Report: A 63-year-old male presented with neck pain and quadriparesis following a fall from a height of 6 feet under the influence of alcohol. Neurological examination revealed upper limb weakness more severe than lower limbs, consistent with CCS. Imaging showed C5–C6 fracture dislocation with bilateral locked facets and spinal cord compression. Closed reduction using Gardner–Wells skull traction was followed by staged posterior lateral mass fixation and anterior cervical discectomy with fusion. The patient showed significant neurological improvement postoperatively.
Conclusion: Early reduction and staged surgical stabilization in C5–C6 bilateral facet dislocation with CCS leads to favorable neurological outcomes, especially in elderly patients with pre-existing cervical degeneration.
Keywords: Cervical spine trauma, facet dislocation, central cord syndrome, subaxial spine injury, quadriparesis.
Subaxial cervical spine injuries account for nearly 65% of all cervical spine traumas [1]. Facetal dislocations usually result from flexion-distraction forces and are frequently associated with neurological deficits [2]. Central cord syndrome (CCS) is most commonly seen in elderly patients with cervical spondylosis following trauma [3]. The coexistence of bilateral facet dislocation at C5–C6 with CCS is uncommon and presents unique challenges in management. We report a rare case successfully treated with staged surgical stabilization.
A 63-year-old male presented to the emergency department with severe neck pain and weakness of all four limbs following a fall from approximately 6 feet while intoxicated. There was no history of loss of consciousness (Fig. 1).

Figure 1: Initial clinical picture of the patient after being received in the emergency department.
Pre-operative neurological assessment demonstrated an incomplete cervical spinal cord injury with a central cord pattern. Motor examination revealed marked weakness of the upper limbs, with key muscle power graded 2/5 bilaterally from C5 to T1. Left T1 assessment was limited due to a pre-existing claw hand deformity. Lower-limb motor strength was relatively preserved at 3/5 bilaterally from L2 to S1.
Sensory examination showed reduced sensation over the upper-limb dermatomes (C5–T1), whereas all sensations were preserved in the lower-limb dermatomes (L2–S1). Sacral sensory sparing was present, and the bulbocavernosus reflex was intact, confirming an incomplete injury. Deep tendon reflexes and muscle tone were normal. The patient was classified as ASIA impairment scale grade D, consistent with CCS. The patient presented with quadriparesis, with upper limb weakness more pronounced than lower limbs and reduced motor power and sensation in the upper limbs (Left > Right). The findings are suggestive of CCS. A plain radiograph of the cervical spine showed C5–C6 fracture dislocation (Fig. 2).
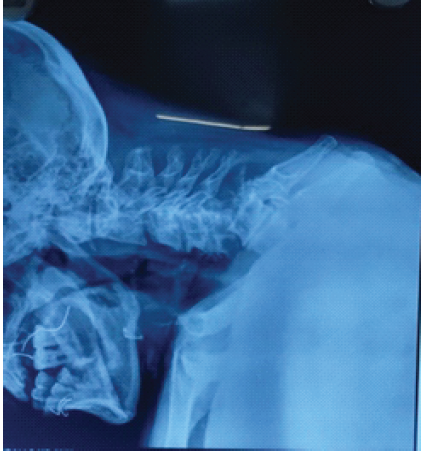
Figure 2: Cervical spine X-ray showing C5–C6 fracture dislocation
A computed tomography scan depicted an anterior dislocation of C5 over C6 with bilateral locked facets (Fig. 3).
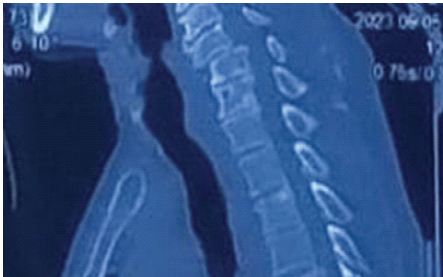
Figure 3: Computed tomography scan showing anterior dislocation of C5 over C6 with bilateral locked facets.
MRI sequences showed anterior dislocation of the C5 vertebral body over C6 vertebra, with bilateral locked facets, spinal cord compression, and signal intensity changes indicating cord edema (Fig. 4).
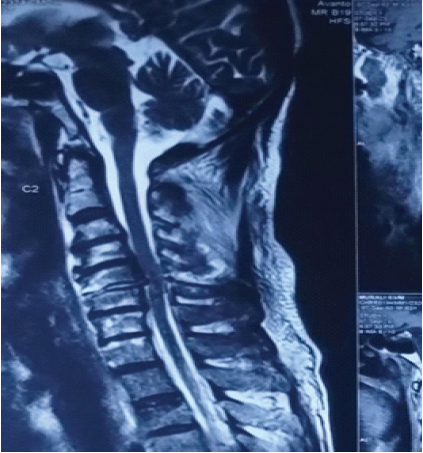
Figure 4: Magnetic resonance imaging sequences showing anterior dislocation of the C5 vertebral body over C6 vertebrae with bilateral locked facets, spinal cord compression, and signal intensity changes indicating cord edema.
C5–C6 fracture-dislocation with bilateral locked facets and CCS was diagnosed. It was a distractive flexion injury – Allen and Ferguson Stage III [1] which correlates with modern classification systems such as the Subaxial Cervical Spine Injury Classification (SLIC) system [4].”
Management
Initial reduction was achieved using Gardner–Wells skull tongs traction [5] (Fig. 5).

Figure 5: Cervical spine lateral X-ray after application of Gardner–Well tongs and successful reduction of dislocation.
After successful reduction, definitive surgical stabilization was performed in two stages:
- Posterior lateral mass fixation for immediate stabilization (Fig. 6)
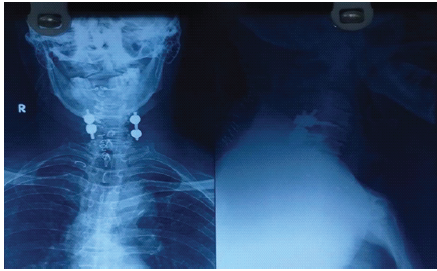
Figure 6: Post-operative cervical spine X-ray, anterior-posterior and lateral view showing the posterior cervical stabilization.
- Anterior cervical discectomy and fusion at the C5–C6 level to restore disc height and anterior column support (Fig. 7).
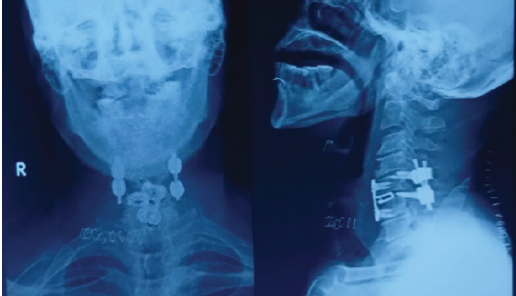
Figure 7: Post-operative cervical spine radiograph showing anterior-posterior and lateral views after the second procedure, showing anterior cervical discectomy and fusion at the C5–C6 level.
Post-operative neurological examination
Post-operative neurological evaluation demonstrated significant improvement, particularly in motor function. Upper-limb motor strength improved to 4/5 on the right side from C5 to T1, and on the left side, it improved to 3/5 till C7, with residual weakness at C8 on the left side. Lower-limb motor power improved to 5/5 bilaterally from L2 to S1. Sensory examination showed improvement in upper-limb sensation. Lower-limb and sacral sensations remained intact. Reflexes and muscle tone remained normal. The patient continued to demonstrate neurological recovery with upper-limb motor strength improving to 5/5 on the right side from C5 to T1, and on the left side, it improved to 4/5 till C7, with residual weakness at C8, more pronounced on the left side at the end of 3 months. At 2-year follow-up, lower-limb motor power was maintained at 5/5 bilaterally from L2 to S1, enabling functional ambulation, with a marked reduction in the upper-limb motor deficit, consistent with expected recovery patterns in CCS. At 2-year follow-up, the radiograph showed intact implants with mild screw loosening (Fig. 8), and left side upper-limb power had improved, with no residual defects (Fig. 9).
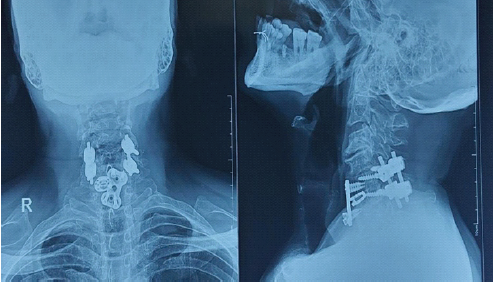
Figure 8: Post-operative cervical spine radiograph showing anterior-posterior and lateral views at 2-year follow-up.

Figure 9: Clinical outcome of the patient showing near normal recovery and back to normal life at 2-year follow-up.
CCS represents the most frequently encountered incomplete spinal cord injury and is classically associated with a disproportionate motor deficit affecting the upper extremities more than the lower extremities. This characteristic neurological pattern is attributable to the somatotopic organization of the corticospinal tracts, wherein fibers innervating the cervical segments and upper limbs are located more centrally within the spinal cord, while thoracic, lumbar, and sacral fibers are positioned progressively more peripherally [3]. Consequently, central cord compression preferentially disrupts upper-extremity motor function, often resulting in pronounced distal weakness of the hands and forearms, which can significantly impair activities of daily living. Sensory deficits are variable, but sacral sparing is frequently observed due to the peripheral location of sacral sensory fibers, a finding that supports the diagnosis of CCS and helps differentiate it from other incomplete cord syndromes. The syndrome most commonly arises following a hyperextension injury in elderly patients with pre-existing cervical spondylosis, osteophyte formation, or degenerative spinal canal stenosis. In this population, hyperextension can result in anterior compression of the spinal cord by vertebral bodies or osteophytes, combined with posterior compression from buckling of the ligamentum flavum and lamina, producing a “pincer” effect on the central cord [6]. Notably, spinal instability is often absent, distinguishing CCS from other traumatic cervical spinal cord injuries that require urgent stabilization. Although less common, CCS has also been described in younger individuals following high-energy trauma or flexion mechanisms, underscoring the heterogeneity of injury patterns associated with this syndrome. Prognosis in CCS is generally favorable compared with other incomplete spinal cord injuries, with many patients demonstrating early and progressive neurological recovery. Recovery typically follows a predictable pattern, with improvement in lower extremity strength preceding proximal upper extremity function and, finally, distal hand function. Despite this overall positive outlook, residual hand weakness and fine motor deficits may persist, particularly in older patients or those with severe initial neurological impairment. Bladder dysfunction may occur in the acute phase but often improves with time. These prognostic considerations are important for patient counseling and rehabilitation planning. Management of CCS remains a topic of ongoing debate, particularly regarding the role and timing of surgical intervention. While historically treated conservatively due to the absence of overt instability, recent literature suggests that selected patients, especially those with significant pre-existing cervical stenosis or neurological deficits, may benefit from early decompressive surgery [7]. Surgical management aims to alleviate ongoing cord compression, potentially facilitating neurological recovery and preventing secondary injury [8,9,10]. Nevertheless, treatment decisions should be individualized, considering patient age, comorbidities, radiographic findings, and neurological progression. In the context of our case, the clinical presentation and imaging findings are consistent with the established pathophysiological mechanisms of CCS described in the literature. We recognized in this case early intervention of reduction by Gardner–Well tongs followed by global stabilization on the next day improved the outcome of the patient. He was back to normal within 2 months. Recognition of this syndrome is critical, as timely diagnosis and appropriate early management can significantly influence functional outcomes.
C5–C6 bilateral facet dislocation with CCS is a rare injury pattern. Prompt reduction and staged surgical stabilization result in good neurological recovery. Early intervention remains the key determinant of outcome.
Early recognition and staged surgical stabilization of cervical facet dislocation with central cord syndrome can significantly improve neurological outcomes, particularly in elderly patients with degenerative spine disease.
References
- 1. Allen BL, Ferguson RL. Mechanisms of injury of the cervical spine. Spine 1982;7:184-97. [Google Scholar] [PubMed]
- 2. Anderson PA, Muchow RD, Munoz A, Resnick DK, Vaccaro AR, Fehlings MG, et al. Facet dislocations of the cervical spine. J Am Acad Orthop Surg 2010;18:718-28. [Google Scholar] [PubMed]
- 3. Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg 1954;11:546-77. [Google Scholar] [PubMed]
- 4. Vaccaro AR, Hulbert RJ, Patel AA, Fisher C, Lehman RA Jr., Dvorak M, et al. The subaxial cervical spine injury classification system: A novel approach to recognize the importance of morphology, neurology, and integrity of the disco-ligamentous complex. Spine (Phila Pa 1976) 2007;32:2365-74. [Google Scholar] [PubMed]
- 5. Fehlings MG, Sekhon LH, Tator C, Arnold P, Benzel E, Brodke DS, et al. Management of cervical spine injuries. Spine 2010;35:S165-77. [Google Scholar] [PubMed]
- 6. Rhee JM, Kraiwattanapong C, Hutton WC, et al. Timing of surgery in cervical spine trauma. Spine J 2015;15:187-95. [Google Scholar] [PubMed]
- 7. Bose B. Anterior cervical fusion for flexion injuries. J Neurosurg 1992;76:716-20. [Google Scholar] [PubMed]
- 8. Joaquim AF, Patel AA, Vaccaro AR, Schroeder GD, Kepler CK, Hilibrand AS, et al. Surgical treatment of cervical facet dislocation. Global Spine J 2014;4:195-202. [Google Scholar] [PubMed]
- 9. Aarabi B, Alexander M, Mirvis SE, Shanmuganathan K, Chesler D, Maulucci C, et al. Central cord syndrome revisited. Neurosurgery 2011;68:195-204. [Google Scholar] [PubMed]
- 10. Fehlings MG, Vaccaro A, Wilson JR, Singh A, Cadotte DW, Harrop JS, et al. Early versus delayed decompression for traumatic cervical spinal cord injury: Results of the surgical timing in acute spinal cord injury study (STASCIS). PLoS One 2012;7:e32037. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture
July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture May 1, 2025 Phrenic Nerve Palsy in Anterior Cervical Discectomy and Fusion: Rare as Hen’s Teeth
May 1, 2025 Phrenic Nerve Palsy in Anterior Cervical Discectomy and Fusion: Rare as Hen’s Teeth September 10, 2022 Synovial Hemangioma Presenting as Anterior Knee Pain – A Case Series
September 10, 2022 Synovial Hemangioma Presenting as Anterior Knee Pain – A Case Series October 1, 2024 Comparison of functional and radiological outcome of unstable intertrochanteric femur fractures treated using PFN and PFNA in patients with osteoporosis
October 1, 2024 Comparison of functional and radiological outcome of unstable intertrochanteric femur fractures treated using PFN and PFNA in patients with osteoporosis