
Delayed jersey finger cases can be treated effectively with single-stage tendon retrieval and anchor fixation without the need for staged reconstruction.
Dr. Musa Ergin, Orthopaedic Surgeon, Cihanbeyli State Hospital, Department of Orthopedics and Traumatology, Konya, Turkey. E-mail: drmusaergin@gmail.com
Abstract
Introduction: Jersey finger, or avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx, is typically a condition requiring prompt surgical intervention. Delayed presentations are rare and present surgical difficulties due to tendon retraction and adhesion formation.
Case Report: We report the case of a 59-year-old patient who presented to the hospital 1 month later with a closed avulsion injury to the flexor tendon of the fifth finger of the left hand following blunt trauma. Intraoperatively, the ruptured FDP tendon was located just proximal to the A1 pulley. Tendon retrieval and distal relocation were performed using a silicone rod. Without sacrificing the pulley system, the tendon was reattached to the distal phalanx using a mini-anchor suture. There was no problem in the post-operative recovery period, and the patient regained satisfactory flexion function.
Conclusion: This case demonstrates that delayed FDP avulsion injuries can be managed effectively with direct repair and anchor fixation, even several weeks post-injury, without pulley sacrifice or complex tendon grafting. However, it should be kept in mind that tendon retraction may not allow direct repair in every case.
Keywords: Jersey finger, flexor tendon avulsion, delayed repair, anchor fixation, flexor digitorum profundus rupture, case report.
Jersey finger refers to the avulsion of the flexor digitorum profundus (FDP) tendon from its insertion at the base of the distal phalanx [1]. The term originates from athletic injuries, where a player grasps an opponent’s jersey, and the finger is suddenly pulled back. Although most cases occur on the ring finger, it can also occur on other fingers [2]. Early diagnosis and prompt surgical repair of jersey finger injuries are critical to prevent long-term functional impairment [3]. Tendon retraction and adhesion formation can occur rapidly, making delayed repairs difficult. In acute cases, direct reattachment of the FDP to the distal phalanx is usually done through a bone anchor or pull-out technique [4]. Delayed cases, particularly those lasting more than 3 weeks after injury, are rare in the literature and are generally associated with worse outcomes. In such chronic cases, treatment options include staged reconstruction, tendon grafting, tendon lengthening, or even arthrodesis if necessary [5]. In this case report, we present a 59-year-old patient who sustained an FDP avulsion injury to her left fifth finger and was admitted to the hospital 1 month after the injury.
A 59-year-old right-handed patient presented with complaints of limited movement, pain, and swelling in her left fifth finger following blunt trauma to her hand. The injury occurred during a fall at home a month ago, and she reported persistent loss of distal flexion and mild swelling. Clinical examination revealed a complete loss of active flexion of the distal interphalangeal (DIP) joint of the left fifth finger, consistent with FDP avulsion. No advanced imaging, such as ultrasound or magnetic resonance imaging (MRI), was performed, as the diagnosis was clinically evident and surgical exploration was already indicated due to the delayed presentation. A small bone fragment was detected to be avulsed on the radiograph.
Surgical technique
Under local anesthesia and without using a tourniquet, a Brunner incision was made distal to the volar aspect of the fifth finger (Fig. 1).

Figure 1: Determination of distal incision line.
Considering that the ruptured tendon due to bone avulsion did not escape to the proximal A4 pulley, only a distal incision was made at first. However, after exploration, it was determined that the A4 pulley was ruptured and the tendon was advancing proximally. Then, a mini-incision was made over the A1 pulley. The ruptured tendon was found at the proximal border of the A1 pulley (Fig. 2). The tendon was identified, mobilized, and delivered distally through the pulley system using a silicone rod to avoid damaging the intact pulleys and to facilitate gliding (Fig. 3). After preparing the FDP insertion site in the distal phalanx, the tendon was fixed using a 2.5 mm mini anchor suture (Fig. 4). Since the tendon tension was appropriate, no lengthening procedure was considered for the tendon (Fig. 5). The A4 pulley was repaired with 4/0 surgical suture. The flexor tendon sheath and skin were meticulously closed.

Figure 2: The flexor tendon could be found at the A1 pulley level.

Figure 3: (a) Advancement of the silicone rod proximally under the pulleys without connecting the incision lines (b) Distal relocation of the ruptured tendon.
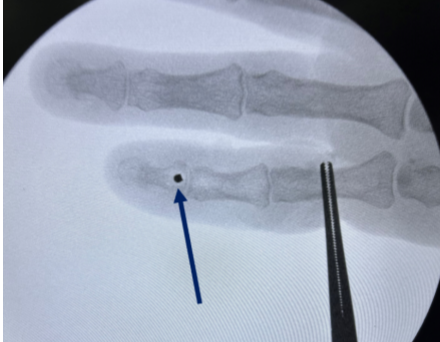
Figure 4: Confirmation of anchor placement with fluoroscopy.

Figure 5: Demonstration of pre-operative and post-operative tendon tension.
Post-operative course
After surgery, the finger was immobilized in a dorsal blocking splint. Passive joint motion exercises were started after the 1st week in the post-operative period. In the 4th week, a protected active motion protocol was started under supervision. At week 12, the patient regained 60° DIP flexion without extension lag, and grip strength was satisfactory for daily activities. Although validated scoring systems such as disabilities of the Arm, Shoulder, and Hand (DASH) were not applied, the patient reported satisfactory functional recovery in daily activities.
FDP avulsion injuries, commonly known as jersey fingers, are usually managed surgically within the first few days after injury to prevent tendon retraction and adhesion formation. Delayed presentations, defined as those occurring more than 4 weeks after injury, are extremely rare and present unique surgical challenges. Most surgeons advocate repair as soon as possible after injury because chronic cases are believed to have limited surgical options and a poorer prognosis [5]. However, recent reports suggest that delayed cases can achieve favorable outcomes with careful surgical planning [6]. In the present case, a one-stage repair was successfully performed despite a 1-month delay. The tendon was found proximal to the A1 pulley, but it was advantageous in that it remained mobile and flexible enough for advancement. The use of a silicone rod enabled atraumatic guidance of the tendon through the sheath and pulley system, facilitating distal advancement without requiring pulley release or staged reconstruction. This approach may not always be possible to manage every chronic case. However, it should be emphasized that this favorable outcome was likely influenced by intraoperative findings, particularly the limited proximal retraction and preserved tendon mobility, which may not be present in all chronic cases. Chronic cases of FDP avulsion are frequently treated with two-stage reconstruction, tendon grafts, and even DIP arthrodesis in low-demand patients [7]. However, these approaches have inherent disadvantages such as prolonged recovery time, risk of graft failure, and joint stiffness. Our case demonstrates that in selected cases where the tendon is not retracted beyond the palm, direct anchor fixation remains a feasible option, even after a significant delay. There is a limited but growing body of literature addressing delayed repairs, although high-level evidence remains scarce. Our case contributes to this gap and suggests that with appropriate patient selection, delayed intervention may provide functional recovery similar to acute repairs. The choice of surgical technique is also an important parameter affecting the results. In acute cases, both the pull-out technique and bone anchors are used. However, especially in cases with small avulsion fractures, mini anchors provide a more stable fixation and reduce the risk of subcutaneous knot complications [8,9]. Halát et al. and Brustein et al. showed in their biomechanical studies that anchor fixation provides higher tensile strength than the pull-out technique [10,11]. Therefore, a mini anchor was preferred in our case, and successful fixation was achieved. The use of silicone rods is recommended in chronic cases to allow the tendon to slide distally more easily and to reduce the risk of adhesion. Savage reported in his in vitro studies that silicone rods provide a smoother glide mechanism in the tendon sheath, thus improving the functional results of the tendon repair performed in the final stage [12]. In our case, tendon mobilization was performed with the help of a silicone rod, the existing pulley structures were preserved, and the functional axis of the tendon was provided. Post-operative rehabilitation is also critical to the success of outcomes. JB Tang reported that early passive and controlled active movement protocols provide a better range of motion by reducing the risk of adhesions in flexor tendon repairs [13]. Parallel to these recommendations, in our case, passive movements were started in the 1st week, protected active movements were started in the 4th week, and results close to a full functional recovery were obtained in the 12th week. However, rehabilitation protocols may vary across institutions, which could influence functional outcomes. This study has several limitations inherent to its case report design. First, it represents a single patient, which limits generalizability. Second, no comparative analysis with alternative treatment strategies such as staged reconstruction, tendon grafting, or DIP arthrodesis was performed. Third, the follow-up duration of 12 weeks is relatively short and does not allow assessment of long-term tendon integrity, late adhesions, or degenerative changes. In addition, functional outcomes were evaluated mainly based on the range of motion and clinical assessment without validated scoring systems such as DASH or Quick DASH, and grip strength was not quantified using a dynamometer. Pre-operative imaging was limited to plain radiographs, and advanced imaging modalities such as ultrasound or MRI were not used. Furthermore, tendon tension was assessed subjectively intraoperatively, and no biomechanical evaluation was performed. Finally, variability in rehabilitation protocols and anatomical differences between patients may influence outcomes. Despite these limitations, this report highlights the feasibility of single-stage repair in selected delayed cases.
The chances of success in delayed jersey finger repairs depend on the availability of the tendon, adequate mobilization, use of appropriate fixation techniques, and careful rehabilitation protocol. Each case should be evaluated individually, and primary repair should be preferred whenever possible.
Even in cases of delayed presentation, direct repair of the jersey finger with a mini-anchor and silicone rod-assisted mobilization can yield satisfactory functional outcomes if careful surgical planning and appropriate rehabilitation are implemented.
References
- 1. Bachoura A, Ferikes AJ, Lubahn JD. A review of mallet finger and jersey finger injuries in the athlete. Curr Rev Musculoskelet Med 2017;10:1-9. [Google Scholar] [PubMed]
- 2. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg 1977;2:66-9. [Google Scholar] [PubMed]
- 3. Gillig JD, Smith MD, Hutton WC, Jarrett CD. The effect of flexor digitorum profundus tendon shortening on jersey finger surgical repair: A cadaveric biomechanical study. J Hand Surg Eur Vol 2015;40:729-34. [Google Scholar] [PubMed]
- 4. Kang N, Marsh D, Dewar D. The morbidity of the button-over-nail technique for zone 1 flexor tendon repairs. Should we still be using this technique? J Hand Surg Eur Vol 2008;33:566-70. [Google Scholar] [PubMed]
- 5. Flint J, Aldridge JM 3rd. Jersey Finger. Singapore: World Scientific Publishing Company; 2016. [Google Scholar] [PubMed]
- 6. Sawaya ET, Choughri H, Pelissier P. One-stage treatment of delayed ‘jersey finger’ by Z-step lengthening of the flexor digitorum profundus tendon at the wrist. J Plast Reconstr Aesthet Surg 2012;65:264-6. [Google Scholar] [PubMed]
- 7. Ruchelsman DE, Christoforou D, Wasserman B, Lee SK, Rettig ME. Avulsion injuries of the flexor digitorum profundus tendon. J Am Acad Orthop Surg 2011;19:152-62. [Google Scholar] [PubMed]
- 8. Halát G, Negrin L, Erhart J, Ristl R, Hajdu S, Platzer P. Treatment options and outcome after bony avulsion of the flexor digitorum profundus tendon: A review of 29 cases. Arch Orthop Trauma Surg 2017;137:285-92. [Google Scholar] [PubMed]
- 9. Schneider LH, Wehbe MA. Delayed repair of flexor profundus tendon in the palm (zone 3) with superficialis transfer. J Hand Surg Am 1988;13:227-30. [Google Scholar] [PubMed]
- 10. Halát G, Negrin LL, Unger E, Koch T, Streicher J, Erhart J, et al. Introduction of a new repair technique in bony avulsion of the FDP tendon: A biomechanical study. Sci Rep 2018;8:9906. [Google Scholar] [PubMed]
- 11. Brustein M, Pellegrini J, Choueka J, Heminger H, Mass D. Bone suture anchors versus the pullout button for repair of distal profundus tendon injuries: A comparison of strength in human cadaveric hands. J Hand Surg 2001;26:489-96. [Google Scholar] [PubMed]
- 12. Savage R. In vitro studies of a new method of flexor tendon repair. J Hand Surg Br 1985;10:135-41. [Google Scholar] [PubMed]
- 13. Tang JB. Rehabilitation after flexor tendon repair and others: A safe and efficient protocol. J Hand Surg Eur Vol 2021;46:813-7. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report
June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report