
Both stand-alone PEEK cages and anterior cervical plating provide comparable short-term clinical outcomes in ACDF. However, the choice of implant should be guided by patient-specific factors, as PEEK cages offer reduced operative morbidity but may be associated with a higher risk of subsidence and loss of lordosis.
Dr. Vikramaditya Rai, Department of Orthopaedics, Dr. Rajendra Prasad Government Medical College, Kangra, Himachal Pradesh, India. E-mail: raizobiotec@gmail.com
Abstract
Introduction: Anterior cervical discectomy and fusion (ACDF) is a widely used procedure for treating cervical spondylotic myelopathy and radiculopathy. While anterior cervical plating (ACP) is the traditional method to ensure stability and fusion, it may be associated with increased dysphagia, adjacent segment degeneration, and hardware complications. Stand-alone polyetheretherketone (PEEK) cages offer a potential alternative with reduced operative morbidity. However, comparative evidence regarding their short-term clinical and radiological outcomes remains limited. The objective of this study was to compare the short-term clinical and radiological outcomes of ACDF performed using stand-alone PEEK cages versus conventional ACP.
Materials and Methods: Current prospective comparative study encompassed 29 patients with cervical radiculopathy or radiculomyelopathy at C3–C7 levels. Group A (n = 14) underwent ACDF with standalone PEEK cage, while Group B (n = 15) underwent conventional ACDF with ACP. Clinical outcomes were determined by employing Visual Analog Scale (VAS) scores, neck pain disability index (NPDI), blood loss, operation time, Odom’s criteria, and post-operative dysphagia. Radiological outcomes included fusion rates, cervical Cobb’s lordosis, and cage subsidence, assessed at 1, 3, and 6 months post-surgery.
Results: Both groups exhibited significant post-surgical improvements in NPDI and VAS scores (P < 0.05), with no notable intergroup differences (P > 0.05). Group A exhibited shorter operation times and less blood loss (P < 0.05). Dysphagia, fusion rates, and surgical outcomes were similar between the groups (P > 0.05). However, Group A exhibited relatively greater cage subsidence, cervical lordosis, loss of disc height, as well as fused segment angle (P < 0.05).
Conclusion: ACDF with stand-alone PEEK cages demonstrated clinical outcomes comparable to ACDF with ACP fixation but showed higher rates of post-operative complications, including loss of cervical lordosis and cage subsidence.
Keywords: Anterior cervical discectomy and fusion, polyetheretherketone cage, anterior cervical discectomy and fusion, anterior cervical plating, cervical radiculopathy, cervical myelopathy, standalone cage, fusion rate, dysphagia, cervical lordosis.
Anterior cervical discectomy and fusion (ACDF) aims to achieve bony union, restore cervical lordosis, and decompress the spinal cord as well as nerve roots. Conventionally, surgeons have utilized anterior cervical plating (ACP) to provide immediate rigid fixation and improve arthrodesis rates [1,2]. However, plating has potential drawbacks, including hardware complications, increased risk of adjacent segment degeneration, and higher incidence of dysphagia and dysphonia, particularly in multilevel procedures [3,4,5,6,7]. To address these concerns, self-locking cage systems have been developed as an alternative to conventional plating. These standalone devices aim to provide similar biomechanical stability while reducing soft-tissue manipulation and anterior bulk [8,9]. Various materials, including titanium, carbon, and polyetheretherketone (PEEK), are used in these cage designs. The predominant drawback associated with standalone cage implementation is the increased frequency of non-union, implant subsidence, diminished cervical lordosis, and pseudarthrosis development [10,11,12]. A recent meta-analysis of 10 randomized controlled trials encompassing 779 patients reported that ACDF with stand-alone spacers outperformed conventional instrumentation in terms of estimated blood loss, total post-operative complications, dysphagia rates, and adjacent segment disease (ASD) [13]. Moreover, conclusive evidence was absent regarding the superior intermediate-term efficacy of standalone cages versus ACP constructs in ACDF procedures [14]. Despite numerous studies comparing standalone cages to plated ACDF constructs, a consensus on the superiority of one technique over the other has not been reached. Current investigation aimed to enhance current body of evidence by evaluating and comparing clinical and radiological outcomes of ACDF performed with standalone PEEK cages versus the traditional technique involving ACP.
Patient selection
This prospective comparative study was conducted at a tertiary care hospital between June 2023 and June 2024. Ethical approval for the study was obtained from the Institutional Ethics Committee of Dr. Rajendra Prasad Government Medical College, Kangra, Himachal Pradesh, India, on May 15, 2023 (IEC approval number: IEC/022/2023). The sample size was based on consecutive enrollment of all eligible patients undergoing single- or two-level ACDF during the study period. Given the exploratory and comparative nature of the study, no formal pre-study sample size calculation was performed, and all patients meeting the inclusion criteria were included to minimize selection bias. A total of 29 patients between the ages of 37 and 60 years who underwent single- or two-level ACDF were included. Inclusion criteria encompassed: (1) Clinical signs and symptoms of cervical spondylotic myelopathy or cervical radiculopathy unresponsive to conservative treatment, (2) Age between 18 and 65 years, (3) Disc herniation confirmed by magnetic resonance imaging (MRI) or computed tomography (CT) demonstrating nerve root or spinal cord compression, and (4) Involvement of one or two contiguous disc levels from C3–C4 to C6–C7. Exclusion criteria included cervical spine fractures, prior cervical surgery, and involvement of three or more levels, predominant posterior pathology, infection, neoplasm, and refusal to provide consent. After obtaining ethical approval and informed consent from all the individual participants, enrolled patients underwent clinical examination, radiography, and MRI. They were randomized into two groups: Group A, comprising 14 patients (12 males; 2 females) with age 50.07 ± 9.92 years (range 38–63) underwent ACDF with stand-alone PEEK cage and Group B, consisting of 15 patients (8 males; 7 females) with age 48.87 ± 11.36 years (range 36–61) underwent conventional ACDF with ACP. Mean follow-up time in Group A was 6.5 ± 7.2 months, and in Group B was 7.2 ± 8.7 months. Complete follow-up was achieved for all participants, with no significant demographic disparities identified between study groups (Table 1).
Surgical technique/devices
Surgeries were conducted using Smith-Robinson cervical fusion technique [2], with the patient, under general anesthesia, positioned supine on the operating table, and a small roll placed under the interscapular region. The ACDF with ACP involves a meticulous approach to the cervical spine through an anterior incision. After careful dissection and exposure of the appropriate level, confirmed radiographically, a complete discectomy was performed. The endplates were meticulously prepared, preserving the subchondral bone while removing all cartilaginous material. A tricortical iliac crest autograft was harvested and precisely fitted to the intervertebral space, ensuring proper depth and alignment. For aminotomy, osteophyte removal was performed as necessary. The graft was then placed, recessed slightly from the anterior vertebral cortex. An ACP was applied to enhance stability. Intraoperative radiographs confirmed proper positioning of the graft and hardware before closure. Postoperatively, patients were immobilized in Philadelphia hard cervical collars for 3 months. The ACDF with a standalone PEEK cage followed a similar initial approach and exposure. After confirming the correct operative level radiographically, a thorough discectomy was conducted encompassing removal of posterior longitudinal ligament, any compressive disc material, and osteophytes. The endplates underwent preparation through curettage and rasping techniques. The appropriate cage size was determined using trial spacers. The chosen PEEK cage was packed with autologous cancellous bone graft and meticulously positioned within the intervertebral space (Fig. 1).
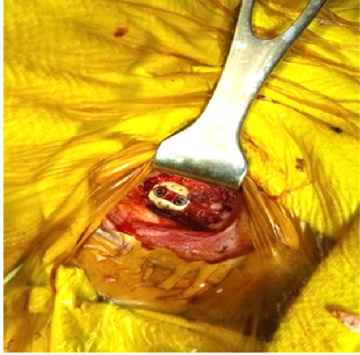
Figure 1: Anterior cervical discectomy and fusion: Intraoperative for cage placement.
Fluoroscopic imaging was employed to confirm appropriate device placement. With plating technique, patients were prescribed Philadelphia hard cervical collar for 3months postoperatively, followed by neck range of motion (ROM) physiotherapy. Follow-up evaluations are conducted at 1, 3, and 6 months post-surgery to assess healing and functional outcomes. Patients were discharged between the 3rd and 5th post-operative days.
Outcome measures
Clinical and radiological follow-ups were carried out at 1, 3, and 6 months post-surgery. Spinal alignment, as well as fusion status, was determined by employing anteroposterior as well as lateral radiographs. Fusion was described as the presence of bridging trabecular bone between endplates, lack of implant failure signs, and <50% radiolucency surrounding cage. Cervical lordotic curvature was assessed through Cobb angle determination from the C2 to C7 inferior endplate landmarks (Fig. 2).
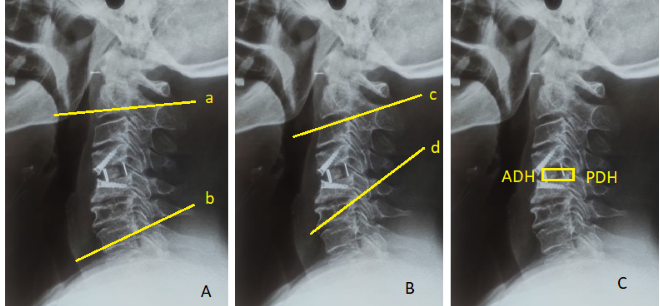
Figure 2: (a) Cervical Cobb’s lordosis measurement: Determined by the angle formed between the upper endplate of C2 and the lower endplate of C7 in the neutral position (lines a and b). (b) Fused segment angle measurement: Calculated as the angle formed between the upper endplate of the superior vertebral body and the lower endplate of the inferior vertebral body in the neutral position (lines c and d). (c) Disc height measurement: The average of the anterior disc height and posterior disc heights.
Primary outcome measures included VAS scores for neck and shoulder pain, handgrip strength, muscle power, neck pain disability index (NPDI), neck ROM, Swallowing Quality of Life Questionnaire (SWAL-QoL) score, Cervical Spine Functional Score (CSFS), arthrodesis, Odom’s criteria, as well as cervical lordosis correction. Secondary outcomes encompass dysphagia, implant subsidence or displacement, fusion rates, and complications. Intraoperative and post-operative data were also collected.
Statistical Analysis
Categorical variables were indicated as numbers and percentages, while quantitative data were expressed as mean ± standard deviations and medians with interquartile ranges (25th–75th percentiles). Data normality was evaluated by employing Shapiro–Wilk test. Non-parametric tests were utilized for non-normally distributed data. For quantitative variables, we applied Mann–Whitney test for non-normally distributed data along with the independent t-test for normally distributed data. Qualitative variables were analyzed by employing the Chi-square test, while Fisher’s exact test was utilized when expected cell values were found to be <5. Data entry was done by employing Microsoft Excel, and final analyses were done by employing IBM Statistical Package for the Social Sciences Statistics version-25.0 (Chicago, USA). For all analyses, P < 0.05 was considered statistically significant.
Clinical outcome assessment
In Group A, eight patients underwent C3–C5 fusion and six underwent C6–C7 fusion by employing standalone PEEK cages. In Group B, seven patients had C3–C5 fusion and eight had C6–C7 fusion with use of an ACP, with insignificant differences observed between groups. Neither group experienced perioperative complications such as cerebrospinal fluid leakage, cage migration, hematoma, wound infection, or plate-related issues. Group A had a shorter operative time (103.5 ± 27.2 min) and less blood loss (132.7 ± 31.6 mL) compared to Group B (128.4 ± 32.3 min; 157.2 ± 39.3 mL), with both differences being statistically significant (P < 0.05) (Table 1).
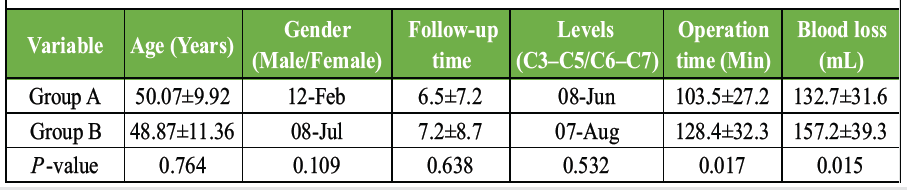
Table 1: Baseline characteristics of the study population
Mild dysphagia was reported by four patients in Group A and 6 in Group B within 24 h post-surgery. Among these, three patients in Group A and 4 in Group B recovered within 2 weeks, while remaining one patient in Group A and 2 in Group B resolved spontaneously by 1 month postoperatively. At final follow-up, none of the patients in either group experienced dysphagia, and there was insignificant difference in dysphagia rates between the groups at any time point. Surgical outcomes, as assessed by Odom’s criteria, demonstrated insignificant differences among groups (Table 2).
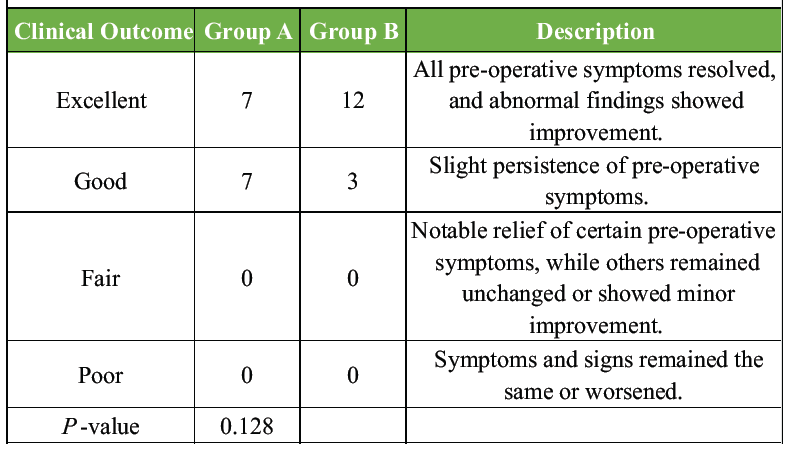
Table 2: Results of surgery according to Odom’s criteria
Functional outcomes
We assessed various parameters at 1, 3, and 6 months postoperatively (Fig. 2).
Figure 2: (a) Cervical Cobb’s lordosis measurement: Determined by the angle formed between the upper endplate of C2 and the lower endplate of C7 in the neutral position (lines a and b). (b) Fused segment angle measurement: Calculated as the angle formed between the upper endplate of the superior vertebral body and the lower endplate of the inferior vertebral body in the neutral position (lines c and d). (c) Disc height measurement: The average of the anterior disc height and posterior disc heights.
VAS for neck pain demonstrated insignificant differences among two groups at any time point (P > 0.05). At 1 month, the median VAS score for the plating group was 2 (range 0–6) compared to 2 (range 1–7) for the PEEK cage group. By 6 months, both groups had a median score of 0, indicating substantial pain reduction in both groups. Similarly, VAS scores for shoulder pain demonstrated insignificant differences among groups at any follow-up (P > 0.05). Median scores at 1 month were 2 for both groups, reducing to 0 for both groups at 3 and 6 months. Muscle power improved in both groups over time, with insignificant differences observed among 2 groups at any follow-up (P > 0.05). Mean muscle power at 1 month was 3.67 ± 1.05 for the plating group and 3.71 ± 0.91 for the PEEK cage group. By 6 months, these values had increased to 4.53 ± 0.92 and 4.64 ± 0.84, respectively. The NPDI scores showed progressive improvement in both groups, with insignificant differences between them at any time point (P > 0.05) (Fig. 3).
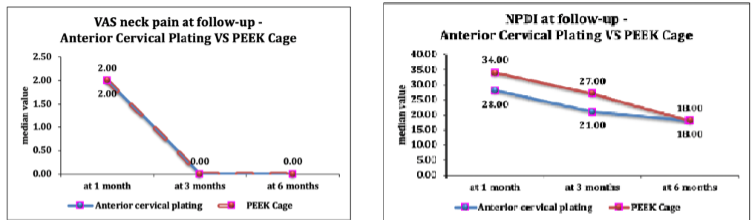
Figure 3: The clinical outcomes: Visual Analog Scale neck pain, and neck pain disability index scores at post-operative 1, 3, and 6 months follow-up.
At 1 month, the median NPDI score for the plating group was 28 (range 20–90) compared to 34 (range 20–92) for the PEEK cage group. By 6 months, these had reduced to 18 (range 9–63) and 18 (range 13–71), respectively.
The SWAL-QoL scores improved over time in both groups, with insignificant differences between them (P > 0.05). Mean scores at 1 month were 29.47 ± 8.78 for the plating group and 28.43 ± 8.82 for the PEEK cage group. At the 6-month mark, these values declined to 13.27 ± 6.35 and 13.29 ± 4.97, respectively, suggesting enhanced swallowing function in both groups.
Neck flexion, extension, and rotation were assessed at each follow-up. For neck flexion, the percentage of patients having a normal range rose from 73.33% at 1 month to 80% at 6 months in the plating group, and from 57.14% to 85.71% in the PEEK cage group. Similar improvements were observed for neck extension. Interestingly, all patients in both groups demonstrated normal left and right cervical rotation at all follow-ups. Insignificant differences were observed between groups for any of these parameters (P > 0.05). Handgrip strength showed gradual improvement in both groups. For the left hand, the percentage of patients with normal grip strength increased from 86.67% at 1 month to 86.67% at 6 months in the plating group, and from 78.57% to 85.71% in the PEEK cage group. For the right hand, these percentages were 80–80% for the plating group and 64.29–71.43% for the PEEK cage group. Group outcomes were comparable, with statistically insignificant variation (P > 0.05). CSFS percentage decreased over time in both groups, indicating functional improvement. At 1 month, the median CSFS was 30.7% for the plating group and 11.05% for the PEEK cage group. At 6-month follow-up, these rates had decreased to 14.2% and 3%, respectively. Nevertheless, the observed differences did not achieve statistical significance (P > 0.05). Odom’s criteria showed progressive improvement in both groups. At 1 month, 53.33% of patients in the plating group and 42.86% in the PEEK cage group had good or excellent outcomes. At 6 months, fusion rates reached 100% in both the plating group and the PEEK cage group. Insignificant differences were found between groups at any follow-up (P > 0.05).
Radiographic outcomes
We assessed implant positioning, Cobb’s angle, and fusion status at several time points post-operatively. Throughout the 6-month follow-up period, no instances of implant malpositioning or subsidence were observed in either group. This suggests that both techniques provided stable implant positioning over the study period. Cervical lordosis was evaluated using Cobb angle measurements (Fig. 4).
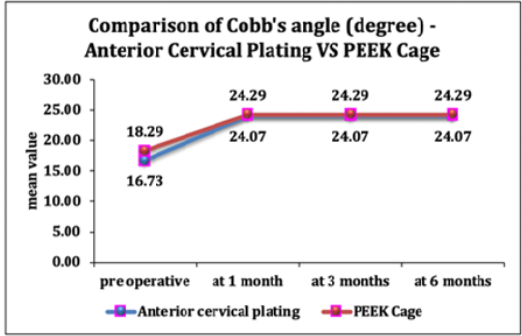
Figure 4: Comparison of trend of Cobb’s angle (degree) at different times of follow-up.
Preoperatively, the mean Cobb’s angle was 18.29 ± 6.32° for Group A and 16.73 ± 6.43° for Group B. At 1 month postoperatively, both groups demonstrated a significant rise in Cobb’s angle compared to pre-operative values (P < 0.05 for both groups). Mean Cobb’s angle rose to 24.07 ± 2.05° in the plating group and 24.29 ± 1.9° in the PEEK cage group. This improvement in cervical lordosis was maintained at 3 and 6 months postoperatively, with insignificant changes found after 1-month mark. Importantly, there were insignificant differences in Cobb’s angle among two groups at any post-operative time point (P = 0.768 at 1, 3, and 6 months). This suggests that both techniques were equally effective in improving and maintaining cervical lordosis.
Fusion status was assessed at 6 months postoperatively (Fig. 5).
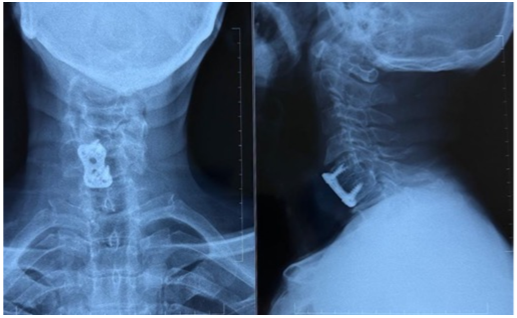
Figure 5: Radiograph on post-operative 6 months showing fusion in conventional plate anterior cervical discectomy and fusion and standalone polyetheretherketone cage.
In the ACP group, 13 out of 15 patients (86.67%) achieved arthrodesis, while in the PEEK cage group, 12 out of 14 patients (85.71%) achieved fusion. Statistically insignificant differences in fusion rates among the two groups (P = 1.00) were observed. Number of patients who did not achieve fusion by 6 months was small and comparable between groups: 2 patients (13.33%) in the plating group and 2 patients (14.29%) in the PEEK cage group.
Complications
At 1 month post-surgery, 11 out of 15 patients in the ACP group and 9 out of 14 in the PEEK Cage group reported no complications. Bone graft site pain affected two patients in each group, while eczema due to cervical collar use was observed in 2 ACP patients and 3 PEEK Cage patients. These differences were statistically insignificant (P = 0.857, Fisher’s exact test). By 3 months, complications had notably decreased. Only one patient in each group reported persistent bone graft site pain, and eczema cases resolved completely. The differences remained statistically insignificant (P = 1, Fisher’s exact test). At the 6-month follow-up, all 29 patients across both groups reported no complications, indicating similar and favorable long-term outcomes for both groups.
Various surgical techniques are available for ACDF, with iliac bone autografts commonly used. One common concern with these grafts is morbidity at the donor site. As a result, interbody fusion using cage fixation has become a popular alternative. Many studies have compared outcomes between cage-only fixation and conventional plate fixation (Table 3), with most reporting no significant differences in clinical outcomes.
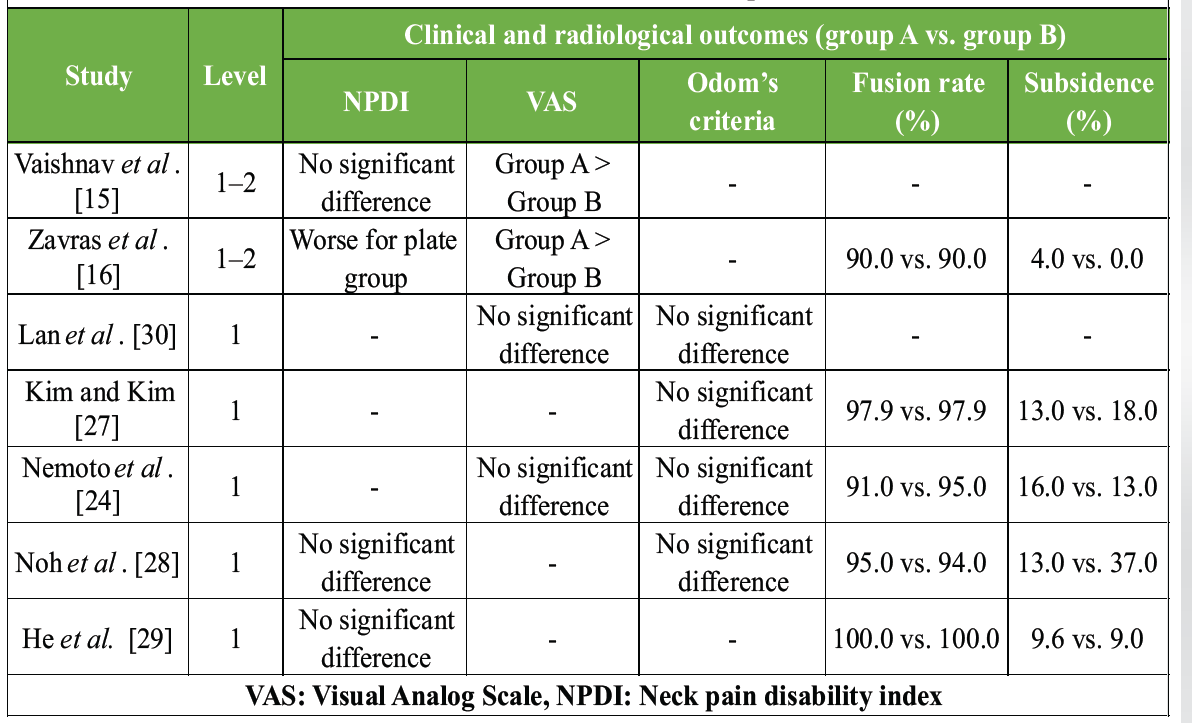
Table 3: Review of previous studies comparing stand-alone cage and conventional plate fixation (at the end of 6 months follow-up)
Nevertheless, research by Vaishnav et al. [15] and Zavras et al. [16] showed significantly better VAS scores in the plate fixation group for single-level ACDF. These differences may be linked to factors such as changes in cervical lordosis due to cage subsidence [17,18,19] or increased posterior cervical tension from pseudoarthrosis.
Although certain studies have not demonstrated a clear link between subsidence and clinical outcomes, Lee et al. observed that increased subsidence was linked to less favorable results [20]. Earlier research comparing fusion rates, subsidence, and kyphosis suggested that cage-only fixation was linked to lower fusion rates but higher rates of subsidence and kyphosis. Notably, the success of fusion decreased with an increasing number of surgical levels [10,19,21]. These findings suggest that cage-only constructs may offer less stable vertebral fixation than conventional plate fixation [22,23]. In this study, we compared clinical and radiological outcomes between single- and two-level ACDF using PEEK cages versus conventional anterior plate fixation. Our results revealed significant differences in blood loss and operation time, with the cage group showing lower values, consistent with outcomes by Zavras et al. [16] and Nemoto et al. [24]. In contrast, Son et al. [25] reported higher blood loss with conventional plate fixation. Although stand-alone cages have demonstrated comparable clinical outcomes to plate fixation in multi-level procedures, differences in blood loss and operation time remain debated [3,8,26]. The reduced blood loss in the cage fixation group may be attributed to less extensive preparation required for the anterior vertebral surface.
Both surgical approaches in our study showed similar improvements in symptoms and structural integrity. Significant improvements in NDI and VAS scores were observed in both groups, with substantial restoration of cervical lordosis and favorable surgical efficacy. No significant differences were found in fusion rates, subsidence rates, physical function, or post-operative complications, supporting the findings of Zavras et al. [16], Kim et al. [27], Noh et al. [28], and He et al. [29]. Regarding swallowing outcomes, SWAL-QoL scores enhanced in both groups over time, with insignificant differences at the final follow-up. These outcomes align with those of Nemoto et al., who similarly reported insignificant differences in dysphagia rates among groups [24]. In contrast, Zavras et al. [16] reported poorer swallowing outcomes in the plate group at both 6 weeks and 6 months, whereas Lan et al. [30] found a lower rate of post-operative dysphagia in cage group. He et al. [29] also found differences in dysphagia rates at 1 and 3 months, though these differences diminished by 12 months. In their studies on ACDF with plate versus PEEK cage in degenerative cervical myelopathy, Zavras et al. [16] and Nemoto et al. [24] concluded that both approaches were effective for managing single- and two-level cervical spondylotic myelopathy. Plate patients reported worse swallow function, but cage-plate construct had better post-operative cervical spine alignment and stability [16,24]. Zhu et al. similarly reported that stand-alone cages demonstrated safety and efficacy in multilevel spinal procedures, but the conventional plate fixation was good for patients requiring more post-operative stability and improved cervical alignment [31]. There are limitations to the current investigation, such as a small sample size, which limits our ability for confirming statistical equivalence among groups, particularly for long-term outcomes such as ASD and arthrodesis rates. This limitation may also explain the minimal changes in physical component scores observed beyond 6 months postoperatively, despite no significant intergroup differences. In addition, some loss to follow-up, especially with radiographic data, and the study’s relatively short duration of 6 months may not capture potential long-term differences between the two techniques.
Current investigation found that both ACDF with stand-alone PEEK cages and conventional ACDF with ACP are equally effective and safe surgical options for treating degenerative cervical spine conditions. The choice between these two methods should depend on patient-specific factors and surgeon preference, as both offer similar outcomes concerning fusion rates, functional recovery, pain relief, and complication rates. Future investigation with larger sample sizes and longer follow-up periods is required for confirming these outcomes and evaluate potential long-term differences among two approaches.
ACDF using either stand-alone PEEK cages or ACP yields comparable short-term clinical outcomes. Stand-alone cages reduce operative time and blood loss but may predispose to greater cage subsidence and loss of lordosis. The choice of technique should therefore be individualized based on patient profile and surgeon preference.
References
- 1. Connolly PJ, Esses SI, Kostuik JP. Anterior cervical fusion: Outcome analysis of patients fused with and without anterior cervical plates. J Spinal Disord 1996;9:202-6. [Google Scholar] [PubMed]
- 2. Wang JC, McDonough PW, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976) 2000;25:41-5. [Google Scholar] [PubMed]
- 3. Yang L, Gu Y, Liang L, Gao R, Shi S, Yuan W, et al. Stand-alone anchored spacer versus anterior plate for multilevel anterior cervical diskectomy and fusion. Orthopedics 2012;35:e1503-10. [Google Scholar] [PubMed]
- 4. Chung JY, Kim SK, Jung ST, Lee KB. Clinical adjacent-segment pathology after anterior cervical discectomy and fusion: Results after a minimum of 10-year follow-up. Spins J 2014;14:2290-8. [Google Scholar] [PubMed]
- 5. Brodke DS, Klimo P Jr., Bachus KN, Braun JT, Dailey AT. Anterior cervical fixation: Analysis of load-sharing and stability with use of static and dynamic plates. J Bone Joint Surg Am 2006;88:1566-73. [Google Scholar] [PubMed]
- 6. Epstein NE. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg Neurol Int 2019;10:100. [Google Scholar] [PubMed]
- 7. Garg R, Rath GP, Bithal PK, Prabhakar H, Marda MK. Effects of retractor application on cuff pressure and vocal cord function in patients undergoing anterior cervical discectomy and fusion. Indian J Anaesth 2010;54:292-5. [Google Scholar] [PubMed]
- 8. Wang Z, Zhu R, Yang H, Shen M, Wang G, Chen K, et al. Zero-profile implant (Zero-p) versus plate cage benezech implant (PCB) in the treatment of single-level cervical spondylotic myelopathy. BMC Musculoskelet Disord 2015;16:290. [Google Scholar] [PubMed]
- 9. Hofstetter CP, Kesavabhotla K, Boockvar JA. Zero-profile anchored spacer reduces rate of dysphagia compared with ACDF with anterior plating. J Spinal Disord Tech 2015;28:E284-90. [Google Scholar] [PubMed]
- 10. Song KJ, Taghavi CE, Lee KB, Song JH, Eun JP. The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Spine (Phila Pa 1976) 2009;34:2886-92. [Google Scholar] [PubMed]
- 11. Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: A prospective study. Spine (Phila Pa 1976) 2002;27:2453-8. [Google Scholar] [PubMed]
- 12. Nambiar M, Phan K, Cunningham JE, Yang Y, Turner PL, Mobbs R. Locking stand-alone cages versus anterior plate constructs in single-level fusion for degenerative cervical disease: A systematic review and meta-analysis. Eur Spine J 2017;26:2258-66. [Google Scholar] [PubMed]
- 13. McDonnell JM, Youssef S, Ross TD, Marland H, Turley L, Cunniffe G, et al. The efficacy of anchored stand-alone spacers in comparison to conventional cage and plate in anterior cervical discectomy and fusion surgery: A meta-analysis of randomised controlled trials for clinical and radiological outcomes. Brain Spine 2024;4:102748. [Google Scholar] [PubMed]
- 14. Li Z, Zhao Y, Tang J, Ren D, Guo J, Wang H, et al. A comparison of a new zero-profile, stand-alone Fidji cervical cage and anterior cervical plate for single and multilevel ACDF: A minimum 2-year follow-up study. Eur Spine J 2017;26:1129-39. [Google Scholar] [PubMed]
- 15. Vaishnav AS, Saville P, McAnany S, Patel D, Haws B, Khechen B, et al. Predictive factors of postoperative dysphagia in single-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976) 2019;44:E400-7. [Google Scholar] [PubMed]
- 16. Zavras AG, Nolte MT, Sayari AJ, Singh K, Colman MW. Stand-alone cage versus anterior plating for 1-level and 2-level anterior cervical discectomy and fusion: A randomized controlled trial. Clin Spine Surg 2022;35:155-65. [Google Scholar] [PubMed]
- 17. Oh K, Lee CK, You NK, Kim SH, Cho KH. Radiologic changes of anterior cervical discectomy and fusion using allograft and plate augmentation: Comparison of using fixed and variable type screw. Korean J Spine 2013;10:160-4. [Google Scholar] [PubMed]
- 18. Park SB, Chung CK, Lee SH, Yang HJ, Son YJ, Chung YS. The impact of menopause on bone fusion after the single-level anterior cervical discectomy and fusion. J Korean Neurosurg Soc 2013;54:496-500. [Google Scholar] [PubMed]
- 19. Pereira EA, Chari A, Hempenstall J, Leach JC, Chandran H, Cadoux-Hudson TA. Anterior cervical discectomy plus intervertebral polyetheretherketone cage fusion over three and four levels without plating is safe and effective long-term. J Clin Neurosci 2013;20:1250-5. [Google Scholar] [PubMed]
- 20. Lee YS, Kim YB, Park SW. Risk factors for postoperative subsidence of single-level anterior cervical discectomy and fusion: The significance of the preoperative cervical alignment. Spine (Phila Pa 1976) 2014;39:1280-7. [Google Scholar] [PubMed]
- 21. El-Tantawy A. Is it possible to eliminate the plate-related problems and still achieve satisfactory outcome after multilevel anterior cervical discectomy? Eur J Orthop Surg Traumatol 2015;25 Suppl 1:S135-45. [Google Scholar] [PubMed]
- 22. Kast E, Derakhshani S, Bothmann M, Oberle J. Subsidence after anterior cervical inter-body fusion. A randomized prospective clinical trial. Neurosurg Rev 2009;32:207-14. [Google Scholar] [PubMed]
- 23. Resnick DK, Trost GR. Use of ventral plates for cervical arthrodesis. Neurosurgery 2007;60 1 Suppl 1:S112-7. [Google Scholar] [PubMed]
- 24. Nemoto O, Kitada A, Naitou S, Tachibana A, Ito Y, Fujikawa A. Stand-alone anchored cage versus cage with plating for single-level anterior cervical discectomy and fusion: A prospective, randomized, controlled study with a 2-year follow-up. Eur J Orthop Surg Traumatol 2015;25 Suppl 1:S127-34. [Google Scholar] [PubMed]
- 25. Son DK, Son DW, Kim HS, Sung SK, Lee SW, Song GS. Comparative study of clinical and radiological outcomes of a zero-profile device concerning reduced postoperative Dysphagia after single level anterior cervical discectomy and fusion. J Korean Neurosurg Soc 2014;56:103-7. [Google Scholar] [PubMed]
- 26. Chen Y, Chen H, Cao P, Yuan W. Anterior cervical interbody fusion with the Zero-P spacer: Mid-term results of two-level fusion. Eur Spine J 2015;24:1666-72. [Google Scholar] [PubMed]
- 27. Kim SJ, Kim SD. Anterior cervical discectomy and fusion using a double cylindrical cage versus an anterior cervical plating system with iliac crest autografts for the treatment of cervical degenerative disc disease. J Korean Neurosurg Soc 2014;55:12-7. [Google Scholar] [PubMed]
- 28. Noh SH, Park JY, Kuh SU, Chin DK, Kim KS, Cho YE, et al. Comparison of zero-profile anchored spacer versus plate-and-cage after 1-Level ACDF with complete uncinate process resection: A 3-year assessment of radiographic and clinical outcomes. Clin Spine Surg 2021;34:176-82. [Google Scholar] [PubMed]
- 29. He S, Zhou Z, Lv N, Shao X, Zhou X, Wang Y, et al. Comparison of clinical outcomes following anterior cervical discectomy and fusion with zero-profile anchored spacer-ROI-C-fixation and combined intervertebral cage and anterior cervical discectomy and fusion: A retrospective study from a single center. Med Sci Monit 2021;27:e931050. [Google Scholar] [PubMed]
- 30. Lan T, Lin JZ, Hu SY, Yang XJ, Chen Y. Comparison between Zero-profile spacer and plate with cage in the treatment of single level cervical spondylosis. J Back Musculoskelet Rehabil 2018;31:299-304. [Google Scholar] [PubMed]
- 31. Zhu D, Zhang D, Liu B, Li C, Zhu J. Can self-locking cages offer the same clinical outcomes as anterior cage-with-plate fixation for 3-level anterior cervical discectomy and fusion (ACDF) in mid-term follow-up? Med Sci Monit 2019;25:547-57. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Evaluation of the Outcome of Zero-profile Implant in the Treatment of Single-level Cervical Spondylotic Myelopathy in the Indian Scenario – A Prospective Study
February 1, 2026 Evaluation of the Outcome of Zero-profile Implant in the Treatment of Single-level Cervical Spondylotic Myelopathy in the Indian Scenario – A Prospective Study July 1, 2026 Severe Aerodigestive Compromise Caused by Cervical Diffuse Idiopathic Skeletal Hyperostosis: A Case Report
July 1, 2026 Severe Aerodigestive Compromise Caused by Cervical Diffuse Idiopathic Skeletal Hyperostosis: A Case Report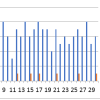 April 1, 2026 Unlocking the Effects of Neural Mobilization versus Transcutaneous Electrical Nerve Stimulation in Cervical Radiculopathy
April 1, 2026 Unlocking the Effects of Neural Mobilization versus Transcutaneous Electrical Nerve Stimulation in Cervical Radiculopathy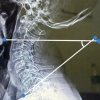 October 1, 2025 Alterartions of Cervical Lordosis in Neck Pain Patients
October 1, 2025 Alterartions of Cervical Lordosis in Neck Pain Patients