
Chronic anterolateral ankle pain in young athletes should not always be attributed to common conditions such as sprains or ligament injuries. Careful clinical examination and appropriate imaging can reveal rare underlying pathologies such as tarsal coalition or soft-tissue tumors. The coexistence of a calcaneonavicular coalition and superficial ankle lipoma is extremely rare, and simultaneous surgical excision through a single approach with extensor digitorum brevis interposition can provide excellent functional outcomes and allow early return to sports.
Dr. Shubham Kalnawat, Department of Orthopedics, Suyog Hospital, Nagpur, Maharashtra, India. E-mail: shubham.kalnawat@gmail.com
Abstract
Introduction: Chronic anterolateral ankle pain in young athletes is commonly attributed to ligament sprains, stress injuries, or tendinopathies. However, uncommon underlying pathologies may occasionally be responsible for persistent symptoms. Calcaneonavicular coalition is a congenital condition that can lead to chronic ankle pain and restricted hindfoot motion. The coexistence of calcaneonavicular coalition with a superficial ankle lipoma is extremely rare.
Case Report: An 18-year-old female cricket athlete presented with gradually progressive swelling and pain over the anterolateral aspect of the right ankle for 5 years, affecting her sports performance. Clinical examination revealed a soft swelling with terminal restriction of dorsiflexion and limited hindfoot movements. Plain radiographs were obtained and demonstrated a calcaneonavicular coalition. Magnetic resonance imaging confirmed the presence of a superficial ankle lipoma along with the coalition. Surgical excision of the lipoma and resection of the calcaneonavicular coalition were performed through a single anterolateral approach. The extensor digitorum brevis muscle was interposed between the calcaneum and navicular to prevent re-ossification. Postoperatively, the patient regained full pain-free ankle motion and returned to sports within 12 weeks.
Conclusion: Persistent anterolateral ankle pain in young athletes should be carefully evaluated to rule out rare conditions such as tarsal coalition and soft-tissue tumors. Early diagnosis and appropriate surgical management can result in excellent functional recovery and return to athletic activity.
Keywords: Calcaneonavicular coalition, ankle lipoma, anterolateral ankle pain, tarsal coalition, young athlete.
We often come across athletes presenting with anterolateral ankle pain, which is usually due to ligament injuries, sprains, stress reactions, or tendinopathies. One such patient presented to our outpatient department with anterolateral ankle swelling and pain. On clinical examination, we initially suspected that the pain was due to a recurrent lipoma, as she had a history of lipoma at the same site. However, while assessing her hindfoot movements, we noticed a restriction in movements compared to the opposite side. This finding made us suspect a possible underlying bony pathology [1]. To confirm this, we advised magnetic resonance imaging (MRI), which surprisingly revealed a calcaneonavicular coalition [2]. This case turned out to be a rare presentation of anterolateral ankle pain in a young athlete caused by the coexistence of a recurrent lipoma and a calcaneonavicular coalition.
An 18-year-old female cricket athlete presented with a gradually increasing swelling and pain over the anterolateral aspect of the right ankle for 5 years. She had a history of a lipoma on the dorsum of the foot 5 years prior. Pain was aggravated during running and dorsiflexion, limiting sports activity. On examination, a soft, non-tender swelling was palpable over the anterolateral ankle with restriction of dorsiflexion, terminally with restricted hindfoot movements. On local examination, a soft, non-tender, well-defined swelling measuring approximately 6 × 3 cm was noted over the anterolateral aspect of the right ankle. The overlying skin was normal with no signs of inflammation. There was a terminal restriction of dorsiflexion as well as inversion–eversion. Distal neurovascular examination was normal. X-rays were taken for further evaluation, which showed calcaneonavicular coalition (Fig. 1).
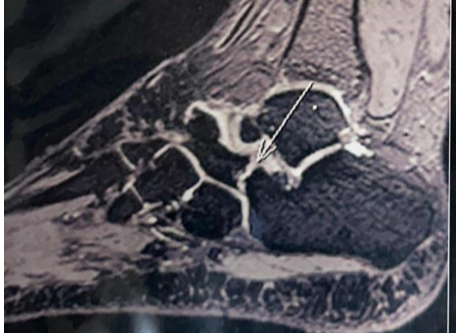
Figure 1: Calcaneonavicular coalition.
To confirm our diagnosis, we went for further investigation with an MRI to get an exact diagnosis and to rule out any soft-tissue malignancy. MRI of the right ankle revealed a well-encapsulated, homogeneously hyperintense lesion on both T1- and T2-weighted sequences, consistent with a lipoma (Fig. 2), located superficial to the anterior capsule and deep to the inferior extensor retinaculum. There was no intra-articular extension.

Figure 2: Lipomatous tissue over the anterolateral aspect of the ankle.
A calcaneonavicular coalition was identified, appearing as a fibro-osseous connection between the anterior process of the calcaneum and the lateral aspect of the navicular bone. Surgery was performed under spinal anesthesia with the patient in the supine position and a pneumatic tourniquet applied to the thigh. An anterolateral incision was made, centered over the swelling and extending from the lateral malleolus toward the sinus tarsi. The superficial peroneal nerve was identified early and carefully protected within the skin flap throughout the procedure. Dissection was carried out through the subcutaneous tissue and the deep fascia. The extensor digitorum brevis (EDB) muscle belly was encountered and divided to expose deeper structures. The inferior extensor retinaculum was incised longitudinally to improve visualization. A well-encapsulated, yellowish, lobulated mass was identified, adherent to the anterior capsule of the ankle joint but with no intra-articular extension. The capsule was preserved. The lesion, measuring almost 6 × 3 cm, was meticulously dissected off the capsule and adjacent tissues and excised en masse (Fig. 3 and 4).
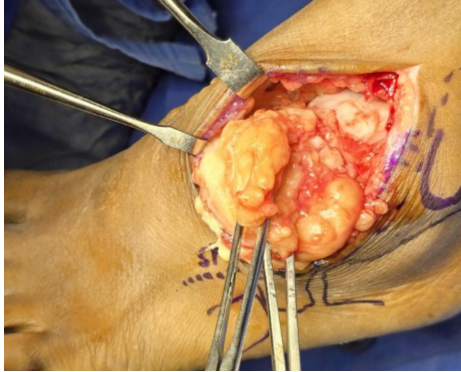
Figure 3: Incision showing lipomatous tissue surrounding the ankle.

Figure 4: Lipoma size approximately 6 by 3 cm.
Intraoperatively, the anterior talofibular and anteroinferior tibiofibular ligament and talar cartilage were normal. Hemostasis was achieved with bipolar cautery. The mass was sent for histopathological examination, which confirmed a benign lipoma composed of mature adipose tissue (Fig. 5 and 6).
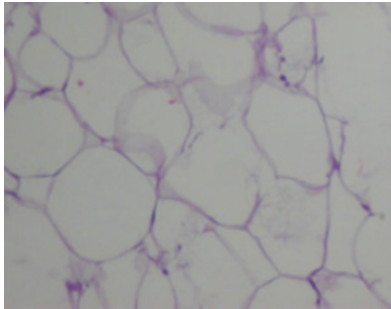
Figure 5: Histopathology of tissue showing adipocytes.
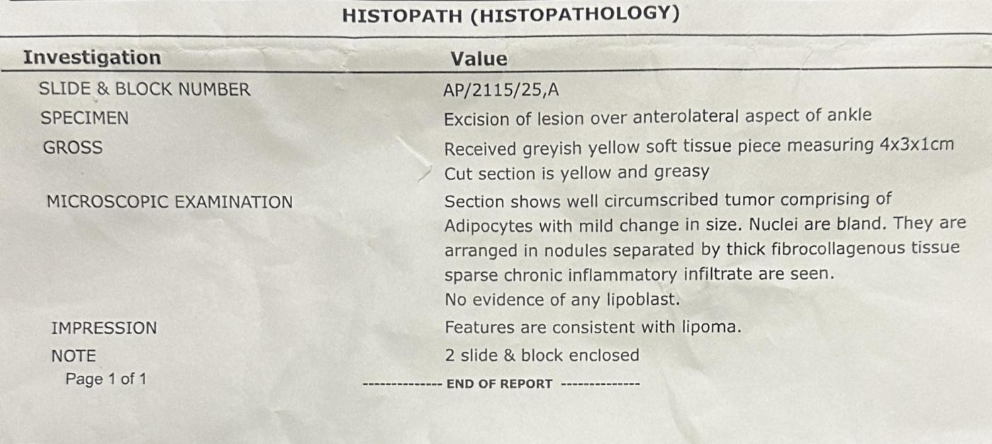
Figure 6: Lipoma size approximately 6 by 3 cm confirmed with histopathological examination.
Attention was then directed to the calcaneonavicular coalition. Through the same approach, the fibro-osseous bridge from calcaneum to navicular of size approximately 3×2 cm was exposed and excised completely (Fig. 7).

Figure 7: Intraoperative image showing a clear calcaneonavicular space after coalition excision.
After coalition excision, there was improvement in hindfoot movements. To prevent re-ossification, the cut belly of the EDB muscle was interposed between the calcaneal and navicular surfaces and sutured in position with absorbable material [3] (Fig. 8).

Figure 8: Extensor digitorum brevis muscle interposed between the calcaneum and naviculum.
After thorough irrigation, the wound was closed in layers: Deep fascia and retinaculum were approximated, subcutaneous tissue closed with absorbable sutures, and skin with interrupted non-absorbable sutures. A below-knee posterior slab was applied in neutral ankle position for 2 weeks. The post-operative course was uneventful. The patient was started on toe-touch walking the next day, immediately followed by gradual ankle mobilization and physiotherapy [4]. By 3 weeks, she achieved a full, pain-free range of motion, and by 12 weeks, she returned to sports training. There was no recurrence at 6-month and 1-year follow-ups (Fig. 9).

Figure 9: 12 months follow-up X-ray of the foot showing maintained space between calcaneum and naviculum.
Common causes of anterolateral ankle pain in young athletes include ligament injuries, cartilage lesions, and tendinopathies. Lipomas of the ankle are rare, likely due to the limited amount of adipose tissue in this region [5]. They may present as painless swellings or may cause discomfort due to compression of adjacent structures or mechanical restriction. In athletes, such swellings can significantly affect sports performance. In addition, the presence of a calcaneonavicular coalition can contribute to chronic ankle pain and altered hindfoot biomechanics. The coexistence of these two conditions is extremely rare and, to the best of our knowledge, has not been widely reported in the literature. MRI is the investigation of choice for differentiating soft-tissue masses and identifying associated pathologies such as tarsal coalition. Surgical excision of calcaneonavicular coalition with interposition of the EDB muscle is a well-established technique that reduces the risk of re-ossification and improves functional outcomes [6]. Surgical excision remains the preferred treatment for symptomatic calcaneonavicular coalition, particularly in young and active individuals who fail conservative management. Resection of the coalition has been shown to provide significant pain relief and restoration of hindfoot mobility in symptomatic patients [7]. To reduce the risk of recurrence and re-ossification following coalition excision, various interposition materials have been described in the literature. These include fat grafts, EDB muscle, and other soft-tissue barriers that help maintain separation between the calcaneum and navicular surfaces [8]. Among these, interposition of the EDB muscle is a commonly employed technique and has demonstrated favorable outcomes in preventing reformation of the coalition. Several studies have reported good long-term functional outcomes following coalition excision with soft-tissue interposition, particularly in young and active patients, enabling return to sports and normal daily activities [9]. Early physiotherapy also plays a crucial role in restoring full ankle range of motion and function after surgery [10].
Calcaneonavicular coalition is an important cause of chronic ankle pain and restricted hindfoot movement, particularly in young athletes. Early recognition through imaging and timely surgical excision can restore full functional mobility. Interposition of the EDB muscle between resected surfaces is crucial to prevent re-ossification and recurrence. While the incidental lipoma in this case contributed to the presentation, the primary source of mechanical limitation was the coalition. Successful management allowed complete recovery and return to competitive activity, underscoring the effectiveness of combined coalition excision and soft-tissue interposition.
Persistent anterolateral ankle pain with swelling in young athletes warrants thorough evaluation beyond routine ligament injuries. Advanced imaging, such as MRI, is essential to detect associated conditions such as tarsal coalition or soft-tissue masses. Surgical excision of calcaneonavicular coalition with interposition of the extensor digitorum brevis muscle effectively prevents recurrence and restores hindfoot mobility. Early diagnosis and appropriate surgical management enable complete recovery and successful return to athletic activity.
References
- 1. Masquijo J, Turazza F. Tarsal coalition: Surgical management in the young athlete. HSS J 2024;20:383-9. [Google Scholar] [PubMed]
- 2. Marth AA, Feuerriegel GC, Marcus RP, Sutter R. How accurate is MRI for diagnosing tarsal coalitions? A retrospective diagnostic accuracy study. Eur Radiol 2024;34:3493-502. [Google Scholar] [PubMed]
- 3. Masquijo J, Mosca VS. Calcaneonavicular coalition resection with fat-graft. J Posna 2024;7:100050. [Google Scholar] [PubMed]
- 4. Abdomari MM, El Kady R, Hider AK, Elhewala TA. Early functional and anatomical results of surgical management of symptomatic tarsal coalition. Zagazig Univ Med J 2024;30:4172-83. [Google Scholar] [PubMed]
- 5. Korumilli RK, Wattamwar A, Veludandi NN. A rare location of lipoma on the sole of foot. J Evid Based Med Healthc 2018;5:383-4. [Google Scholar] [PubMed]
- 6. Gonzalez P, Kumar SJ. Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-7. [Google Scholar] [PubMed]
- 7. Scott AT, Tuten HR. Calcaneonavicular coalition resection with extensor digitorum brevis interposition in adults. Foot Ankle Int 2007;28:890-5. [Google Scholar] [PubMed]
- 8. Mubarak SJ, Patel PN, Upasani VV, Moor MA, Wenger DR. Calcaneonavicular coalition: Treatment by excision and fat graft. J Pediatr Orthop 2009;29:418-26. [Google Scholar] [PubMed]
- 9. Angelis S, Myrgiotis D, Apostolopoulos AP, Mandragos E, Statyris NC, Filippou DK, et al. Surgical removal of bone bridge and interposition of the extensor digitorum brevis in the treatment of calcaneonavicular coalition in pediatric patients: A case series and review. J Long Term Eff Med Implants 2022;32:27-37. [Google Scholar] [PubMed]
- 10. Garg V, Nasim O, Kumar S, Khan MN, Durrani A, Karim A. Resection of bar in the management of calcaneonavicular coalition: A systematic review. Cureus 2023;15:e39275. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 4, 2020 Bilateral Traumatic Proximal Humeral Physeal Fracture in an Adolescent Child – A Rare Case Report and Review of Literature
December 4, 2020 Bilateral Traumatic Proximal Humeral Physeal Fracture in an Adolescent Child – A Rare Case Report and Review of Literature February 5, 2012 Isolated Quadrilateral Plate Fracture of the Acetabulum – a unique case Scenario
February 5, 2012 Isolated Quadrilateral Plate Fracture of the Acetabulum – a unique case Scenario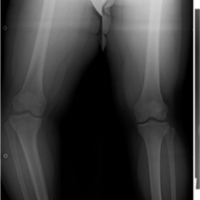 September 10, 2021 Inversed V-shaped High Tibial Osteotomy for Severe Varus Deformity due to Blount Disease: A Case Report
September 10, 2021 Inversed V-shaped High Tibial Osteotomy for Severe Varus Deformity due to Blount Disease: A Case Report November 1, 2024 Minimally Invasive Percutaneous Plate Osteosynthesis with Proximal Humerus Locking Plate for Pediatric Comminuted Subtrochanteric Femur Fracture: A Case Report
November 1, 2024 Minimally Invasive Percutaneous Plate Osteosynthesis with Proximal Humerus Locking Plate for Pediatric Comminuted Subtrochanteric Femur Fracture: A Case Report