
Bilateral Modified Woodward Procedure done simultaneously in a single operative setting is feasible and can achieve satisfactory functional and cosmetic outcomes. This approach helps reduce overall operative time, anesthesia exposure, hospital stay, and cost. Moreover, enable a single rehabilitation period and faster return to daily activities with improved shoulder range of motion, and better cosmetic symmetry, while avoiding staged surgeries.
Dr. Hayfaa Saud Alshaalan, Department of Orthopedics, College of Medicine, King Saud University, Riyadh, Saudi Arabia. E-mail: halshaalan@ksu.edu.sa
Abstract
Introduction: Sprengel’s deformity (SD) is a rare congenital scapular deformity, characterized by a small, elevated, or malpositioned scapula. Although it is rare, it is considered one of the most common congenital abnormalities of the shoulder in children. The scapula will be highly raised triangularly shaped, anteriorly and medially rotated, with limited scapulothoracic motion. As a result, patients will present with functional impairment, such as limited abduction and forward flexion, and cosmetic concerns. Various surgical approaches aiming for correction of SD have been established, including scapular osteotomy, parascapular muscles detachment and reattachment, and omovertebral bone resection. At present, Woodward procedure is among the most used surgical techniques to correct SD with good clinical outcomes. This aims for repositioning of the scapula and resection of the omovertebral bone or fibrous structures when identified, thereby enhancing both functional range of motion and cosmetic appearance. In this report, we present a case of a 6-year-old girl known to have Klippel-Feil Syndrome (KFS) with bilateral SD that was corrected by Bilateral Modified Woodward procedure simultaneously in a single operative setting.
Case Report: We described a 6-year-old female child, a known case of KFS Type 2 with bilateral SD. Examination revealed bilaterally elevated scapulae with limited abduction. Imaging, including computed tomography, revealed bilateral SD, more pronounced on the left side, characterized by elevated and axially rotated scapulae. She underwent bilateral Modified Woodward’s procedure done in the same operative setting in addition to anchoring the scapula to the relevant vertebrae.
Conclusion: Multiple surgical techniques have been described aiming to treat bilateral SD. In this case report, the patient was treated with bilateral Modified Woodward’s procedure done in the same operative setting in addition to anchoring the scapula to the relevant vertebrae to reduce the risk of recurrence, which showed excellent intraoperative outcomes without any complications.
Keywords: Sprengel’s deformity, bilateral modified Woodward procedure, scapula.
Sprengel’s deformity, “SD,” is a rare congenital scapular deformity, characterized by a small, elevated, or malpositioned scapula, primarily described by Eulenberg in 1863. Although it is rare, SD is considered one of the most common congenital abnormalities of the shoulder in children [1,2]. The scapula will be highly raised, triangularly shaped, anteriorly and medially rotated, with limited scapulothoracic motion. As a result, SD patients will present with functional impairment, such as limited abduction and forward flexion, and cosmetic concerns [3,4,5]. Usually, SD is associated with muscle hypoplasia or atrophy, and an omovertebral connection, cartilaginous, fibrous, or osseous. The etiology of interrupted caudal migration of the developing scapula remains uncertain [6]. Congenital elevated scapula is frequently associated with multiple congenital anomalies, including Klippel-Feil syndrome, rib malformations, hemivertebrae, scoliosis, and diastematomyelia [6,7,8]. In 1972, the Cavendish classification was introduced, which was categorizing the disease based on the shoulder deformity, not the functional impairment. Grade 1 represents a very mild deformity while the patient is dressed. Grade 2 represents a mild deformity visible as a prominent lump in the web of the neck while the patient is dressed. Grade 3 represents a moderate deformity easily visible with shoulder elevation 2–5 cm. Grade 4 represents a severe deformity with the shoulder joint elevated more than 5 cm or scapular superior angle near the occiput with or without neck webbing. Although this classification is widely used, it has a limited role in influencing the treatment decision and predicting the outcome, as it focuses only on the cosmetic appearance of the shoulder [3,9]. Cosmetic and functional improvement considered the two main goals of treatment. Surgical correction is the preferred choice of SD in moderate to severe cases, while mild cases can be managed by observation and physical therapy [3,4,5,10]. The management of SD is primarily based on the patient’s age, functional impairment, and cosmetic concerns. Various surgical approaches aiming for correction of SD have been established, including scapular osteotomy, parascapular muscles detachment and reattachment, and omovertebral bone resection. At present, Woodward procedure is among the most used surgical techniques to correct SD with good clinical outcomes. This aims for repositioning of the scapula and resection of the omovertebral bone or fibrous structures when identified, thereby enhancing both functional range of motion and cosmetic appearance [2,4,5,6,10]. In this report, we present a case of a 6-year-old girl known to have Klippel-Feil Syndrome with bilateral SD that was corrected by the Bilateral Modified Woodward procedure simultaneously in a single operative setting.
A 6-year-old female child, known case of KFS Type 2, was referred to the orthopedic service for evaluation and management of bilateral SD. She has a notable medical history, including short stature and intrauterine growth restriction at birth (birth weight: 2700 g). She is under regular follow-up for scoliosis and has undergone a right inguinal herniotomy in the past. The diagnosis of KFS was confirmed by genetic testing, revealing a homozygous pathogenic variant in the MOXI gene. Family history is significant for a male sibling with a confirmed diagnosis of KFS and a variant of uncertain significance in the AP3B2 gene. Examination revealed bilaterally elevated scapulae with limited abduction. Imaging, including computed tomography, revealed bilateral SD, more pronounced on the left side, characterized by elevated and axially rotated scapulae. There are bilateral omovertebral bones seen at the C3–C4 level, appearing as short, well-corticated bony structures medial to the scapulae, with no bony fusion to the scapulae. In addition, there is a posterior cervical fusion at C3–C4, consistent with underlying KFS. No evidence of aggressive osseous lesions is seen. The remaining visualized upper chest and cervical structures are grossly unremarkable. After multidisciplinary evaluation, the patient was scheduled for bilateral Modified Woodward’s procedure.
Surgical technique
The patient underwent bilateral Modified Woodward’s procedure under general anesthesia. She was placed in the prone position, and the surgical field was prepared in a sterile fashion with exposure of the posterior neck, back, and scapulae. A midline posterior incision was made extending from C2 to T12. Dissection was carried out through the posterior scapular line to access the left scapula. The periscapular muscles were reflected, and the cartilaginous portions of the scapula were resected (Fig. 1). Omovertebral bar was identified and resected (Fig. 2).
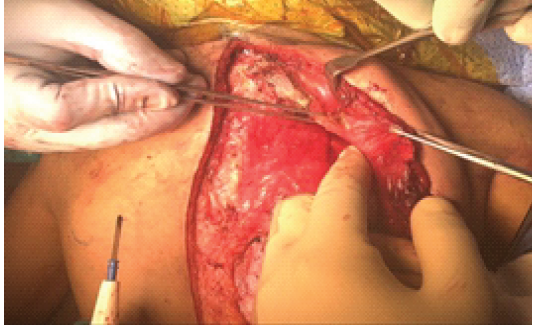
Figure 1: The omovertebral bar with the cartilaginous connection to the scapula (forceps holding cartilaginous part).
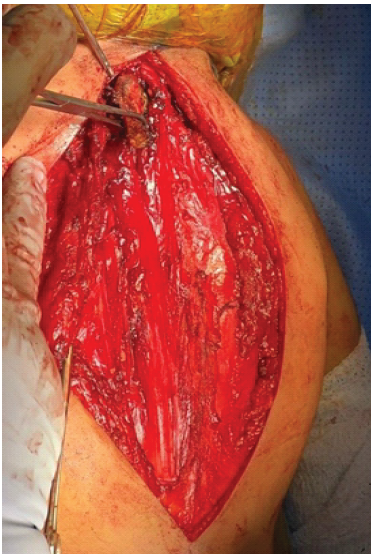
Figure 2: The omovertebral bar after resection.
Then moving on to the right side, the same procedure was carried out in a similar manner. Omovertebral sizes were noted: The right measured 2.5 × 4.5 cm, and the left measured 1.7 × 3.7 cm (Fig. 3).
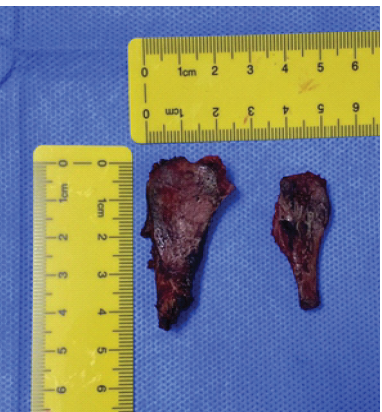
Figure 3: Both omovertebral bars after resection
After mobilization of both scapulae, they were caudally repositioned. Following the anchoring suture modification described by Alsiddiky AM et al., the scapulae were secured in their corrected position using No. 2 Vicryl anchoring sutures, passed from the lower scapular region (1 cm lateral to the vertebral edge) to the spinous processes of T11–T12 at an angle of 30–40° [6]. The scapulae were anchored at a point approximating the center of rotation, allowing both stabilization and rotation. The shoulders were abducted intraoperatively to confirm appropriate scapular mobility before final tightening of sutures. The patient tolerated the procedure well with preserved distal pulses and intact upper limb movements postoperatively. Bilateral body strapping for both upper limbs was applied.
SD refers to a rare congenital condition where the scapula fails to descend to its normal position during fetal development, which is seen more commonly in girls than boys [11]. Despite the rarity of this condition, it is one of the most common congenital anomaly affecting the scapula, which in turn results in limited shoulder range of motion due to an abnormal connection between the scapula and spine, disorientation, and/or dysplasia of the scapula, along with an abnormally high, cosmetically unpleasing appearance of the shoulder blade [12]. A connection between the superomedial aspect of the scapula and cervical spine has been seen in one third of the cases of SD in which the connection could be fibrous, cartilaginous, or bony [12]. Surgical intervention is preferred, aiming to correct the cosmetic appearance and restore the normal function of the scapula [12]. One of the most commonly used surgical techniques to treat SD are Green procedure and the Woodward procedure, where a resection is done of the fibrous band and/or omovertebral bone, with downward placement of the rhomboid and trapezius muscle is achieved [12]. The rate of major complications is seen in 2.5% of cases where surgical intervention is chosen, which indicates that surgical intervention as a treatment of SD was safe and effective [13]. One of the most devastating complications following the Woodward procedure is brachial plexus palsy (BPI), ranging from 0% to 12.5%, and seen more with older children [14]. Based on surgeon experience and preference, concomitant clavicle osteotomy, along with intraoperative neuromonitoring, has been used as a preventative measures to avoid BPI [14]. In our case, both measures were not used on our patient, and she did not show any signs or symptoms of BPI post-surgery. Rates of incomplete correction and recurrence of the deformity have been observed in previous studies [15]. Aiming to reduce the risk of deformity recurrence, a surgical technique was described previously were absorbable Vicryl sutures used to anchor the scapula to the spinous process of the relevant vertebrae has shown reduction of deformity recurrence in a long-term follow-up [16]. In the presented case, the same technique was used on both sides.
Multiple surgical techniques have been described aiming to treat bilateral SD. In this case report, the patient was treated with bilateral Modified Woodward procedure done in the same operative setting in addition to anchoring the scapula to the relevant vertebrae to reduce the risk of recurrence, which showed excellent intraoperative outcomes without any complications.
This case highlights that simultaneous bilateral correction of SD using the modified Woodward procedure in addition to anchoring the scapula to the relevant vertebrae is a safe, feasible, and effective alternative to staged unilateral surgeries with improved recurrence rates. Performing both sides in a single operative sitting can provide improved shoulder range of motion, better cosmetic symmetry, faster functional recovery, and reduced overall treatment burden while avoiding staged surgeries.
References
- 1. Eulenberg M. Contribution to the dislocation of the scapula. Proceedings of the Assembly of German Natural Scientists and Physicians, Karlsbad 1863;37:291–294. [Google Scholar] [PubMed]
- 2. Harvey EJ, Bernstein M, Desy NM, Saran N, Ouellet JA. Sprengel deformity: Pathogenesis and management. J Am Acad Orthop Surg 2012;20:177-86. [Google Scholar] [PubMed]
- 3. Pargas C, Santana A, Czoch WL, Rogers KJ, Mackenzie WG. Sprengel deformity in biological sisters. J Am Acad Orthop Surg Glob Res Rev 2020;4:e19.00120. [Google Scholar] [PubMed]
- 4. Bhatia DN, Dasgupta B, Kadavkolan AS, Bhosale PB. Sprengel’s deformity of the shoulder: Current perspectives in management. Int J Shoulder Surg 2011;5:1-8. [Google Scholar] [PubMed]
- 5. Poutoglidou F, Metaxiotis D, Alvanos D, Mpeletsiotis A. Bilateral sprengel’s deformity treated with the modified Woodward procedure: Technique and outcome of 3 consecutive case reports. SN Compr Clin Med 2021;3:754-8. [Google Scholar] [PubMed]
- 6. Jindal N, Gupta P. Sprengel’s shoulder treated by the Woodward procedure: Analysis of factors affecting functional and cosmetic outcome. J Child Orthop 2012;6:291-6. [Google Scholar] [PubMed]
- 7. Laasri K, Izi Z, El Harras Y , Marrakchi S, Laamrani FZ, Jroundi L, et al. Sprengel’s deformity. Radiol Case Rep 2024;20:133-5. [Google Scholar] [PubMed]
- 8. Ahmad AA. Surgical correction of severe sprengel deformity to allow greater postoperative range of shoulder abduction. J Pediatr Orthop 2010;30:575-81. [Google Scholar] [PubMed]
- 9. Stelzer JW, Flores MA, Mohammad W, Esplin N, Mayl JJ, Wasyliw C. Klippel-Feil syndrome with sprengel deformity and extensive upper extremity deformity: A case report and literature review. Case Rep Orthop 2018;2018:5796730. [Google Scholar] [PubMed]
- 10. Pinheiro JP, Fernandes P, Sarmento M. Bilateral sprengel deformity with bilateral omovertebral bone: An unusual case in an adult patient: A case report. JBJS Case Connect 2023;13:4. [Google Scholar] [PubMed]
- 11. Cury Da Cunha A, Magalhães Forni G, Storti ME, Polatto Pulino Palumbo P, Duarte ML. Sprengel deformity due to an omovertebral bone. Medicina (B Aires) 2025;85:467. [Google Scholar] [PubMed]
- 12. Pandey A, Kayastha SR, Pande P, Silwal P, Upadhyaya P, Pandey A, et al. Management of Sprengel deformity by modified Woodward approach and outcome: A case series and literature review. Ann Med Surg (Lond) 2024;87:43-8. [Google Scholar] [PubMed]
- 13. Zarantonello P, Di Gennaro GL, Todisco M, Cataldi P, Stallone S, Evangelista A, et al. Surgical treatment of Sprengel’s deformity: A systematic review and meta-analysis. Children (Basel) 2021;8:1142. [Google Scholar] [PubMed]
- 14. Zhang L, Cai H, Huang Y, Yang M, Huang S, Miao M, et al. Woodward procedure with intraoperative neuromonitoring for Sprengel deformity: A retrospective study with a mean 5-year follow-up. Front Pediatr 2025;13:1541132. [Google Scholar] [PubMed]
- 15. Grogan DP, Stanley EA, Bobechko WP. The congenital undescended scapula. Surgical correction by the Woodward procedure. J Bone Joint Surg Br 1983;65:598-605. [Google Scholar] [PubMed]
- 16. Alsiddiky AM, Rafiq Z, Bakarman KA, Alhuzaimi FS, Asif M. A novel modification of Woodward procedure for correction of sprengel deformity by application of anchoring sutures. Indian J Orthop 2020;55(Suppl 1):189-98. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor July 1, 2026 “Sprengel’s Deformity in Children” – A Case Series with an Evidence-Based Approach in Diagnosis and its Surgical Management
July 1, 2026 “Sprengel’s Deformity in Children” – A Case Series with an Evidence-Based Approach in Diagnosis and its Surgical Management February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report
December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report